
Interim Estimates of COVID-19 Vaccine Effectiveness in a Mass Vaccination Setting: Data from an Italian Province

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
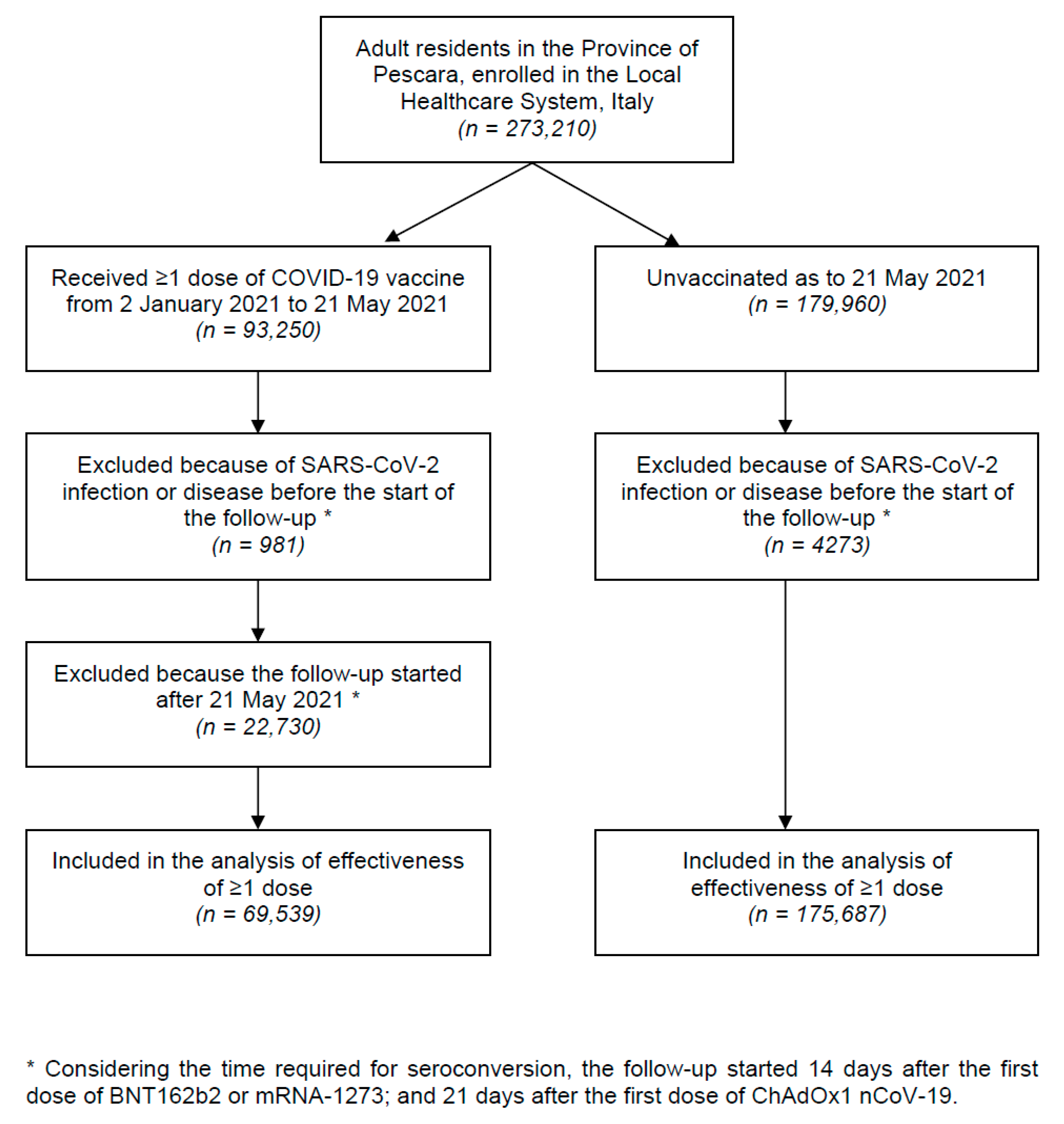
2.1. Study Design, Population and Outcomes
2.2. Public Health Surveillance
2.3. Data Analysis
3. Results
3.1. Characteristics of the Sample
3.2. Vaccine Effectiveness
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Worldometer. COVID-19 Coronavirus Outbreak. 2020. Available online: https://www.worldometers.info/coronavirus/ (accessed on 8 June 2021).
- Acuti Martellucci, C.; Flacco, M.E.; Cappadona, R.; Bravi, F.; Mantovani, L.; Manzoli, L. SARS-CoV-2 pandemic: An overview. Adv. Biol. Regul. 2020, 77, 100736. [Google Scholar] [CrossRef]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Voysey, M.; Clemens, S.A.C.; Madhi, S.A.; Weckx, L.Y.; Folegatti, P.M.; Aley, P.K.; Angus, B.; Baillie, V.L.; Barnabas, S.L.; Bhorat, Q.E.; et al. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: An interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet 2021, 397, 99–111. [Google Scholar] [CrossRef]
- Sadoff, J.; Gray, G.; Vandebosch, A.; Cárdenas, V.; Shukarev, G.; Grinsztejn, B.; Goepfert, P.A.; Truyers, C.; Fennema, H.; Spiessens, B.; et al. Safety and Efficacy of Single-Dose Ad26.COV2.S Vaccine against Covid-19. N. Engl. J. Med. 2021. [Google Scholar] [CrossRef] [PubMed]
- Pormohammad, A.; Zarei, M.; Ghorbani, S.; Mohammadi, M.; Razizadeh, M.H.; Turner, D.L.; Turner, R.J. Efficacy and Safety of COVID-19 Vaccines: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Vaccines 2021, 9, 467. [Google Scholar] [CrossRef] [PubMed]
- Italian Ministry of Health. Piano Vaccini Anti COVID-19 [Italian Mational Immunization Plan against COVID-19]. 2020. Available online: https://www.salute.gov.it/portale/nuovocoronavirus/dettaglioContenutiNuovoCoronavirus.jsp?lingua=italiano&id=5452&area=nuovoCoronavirus&menu=vuoto (accessed on 8 June 2021).
- European Centre for Disease Prevention and Control. COVID-19 Vaccine Tracker. Available online: https://vaccinetracker.ecdc.europa.eu/public/extensions/COVID-19/vaccine-tracker.html#uptake-tab (accessed on 5 May 2021).
- Fabiani, M.; Ramigni, M.; Gobbetto, V.; Mateo-Urdiales, A.; Pezzotti, P.; Piovesan, C. Effectiveness of the Comirnaty (BNT162b2, BioNTech/Pfizer) vaccine in preventing SARS-CoV-2 infection among healthcare workers, Treviso province, Veneto region, Italy, 27 December 2020 to 24 March 2021. Euro Surveill. 2021, 26. [Google Scholar] [CrossRef] [PubMed]
- Hall, V.J.; Foulkes, S.; Saei, A.; Andrews, N.; Oguti, B.; Charlett, A.; Wellington, E.; Stowe, J.; Gillson, N.; Atti, A.; et al. COVID-19 vaccine coverage in health-care workers in England and effectiveness of BNT162b2 mRNA vaccine against infection (SIREN): A prospective, multicentre, cohort study. Lancet 2021. [Google Scholar] [CrossRef]
- Thompson, M.G.; Burgess, J.L.; Naleway, A.L.; Tyner, H.L.; Yoon, S.K.; Meece, J.; Olsho, L.E.W.; Caban-Martinez, A.J.; Fowlkes, A.; Lutrick, K.; et al. Interim Estimates of Vaccine Effectiveness of BNT162b2 and mRNA-1273 COVID-19 Vaccines in Preventing SARS-CoV-2 Infection Among Health Care Personnel, First Responders, and Other Essential and Frontline Workers—Eight U.S. Locations, December 2020-March 2021. MMWR Morb, Mortal Wkly, Rep. 2021, 70, 495–500. [Google Scholar] [CrossRef]
- Abu-Raddad, L.J.; Chemaitelly, H.; Butt, A.A. Effectiveness of the BNT162b2 Covid-19 vaccine against the B.1.1.7 and B.1.351 variants. N. Engl. J. Med. 2021. [Google Scholar] [CrossRef]
- Dagan, N.; Barda, N.; Kepten, E.; Miron, O.; Perchik, S.; Katz, M.A.; Hernan, M.A.; Lipsitch, M.; Reis, B.; Balicer, R.D. BNT162b2 mRNA Covid-19 Vaccine in a Nationwide Mass Vaccination Setting. N. Engl. J. Med. 2021, 384, 1412–1423. [Google Scholar] [CrossRef]
- Reno, C.; Maietti, E.; Fantini, M.P.; Savoia, E.; Manzoli, L.; Montalti, M.; Gori, D. Enhancing COVID-19 Vaccines Acceptance: Results from a Survey on Vaccine Hesitancy in Northern Italy. Vaccines 2021, 9, 378. [Google Scholar] [CrossRef]
- Bravi, F.; Flacco, M.E.; Carradori, T.; Volta, C.A.; Cosenza, G.; De Togni, A.; Acuti Martellucci, C.; Parruti, G.; Mantovani, L.; Manzoli, L. Predictors of severe or lethal COVID-19, including Angiotensin Converting Enzyme inhibitors and Angiotensin II Receptor Blockers, in a sample of infected Italian citizens. PLoS ONE 2020, 15, e0235248. [Google Scholar] [CrossRef]
- Riccardo, F.; Andrianou, X.; Bella, A.; Del Manso, M.; Urdiales, A.M.; Fabiani, M.; Bellino, S.; Boros, S.; D’Ancona, F.; Rota, M.C.; et al. Italian National Institute of Health. COVID-19 Integrated Surveillance System. Available online: https://www.epicentro.iss.it/coronavirus/sars-cov-2-sorveglianza (accessed on 2 June 2021).
- Flacco, M.E.; Acuti Martellucci, C.; Bravi, F.; Parruti, G.; Mascitelli, A.; Mantovani, L.; Boccia, S.; Manzoli, L. Severe Acute Respiratory Syndrome Coronavirus 2 Lethality Did not Change Over Time in Two Italian Provinces. Open Forum Infect. Dis. 2020, 7, ofaa556. [Google Scholar] [CrossRef] [PubMed]
- Kriss, J.L.; Reynolds, L.E.; Wang, A.; Stokley, S.; Cole, M.M.; Harris, L.Q.; Shaw, L.K.; Black, C.L.; Singleton, J.A.; Fitter, D.L.; et al. COVID-19 Vaccine Second-Dose Completion and Interval between First and Second Doses Among Vaccinated Persons—United States, December 14, 2020–February 14, 2021. MMWR Morb. Mortal Wkly. Rep. 2021, 70, 389–395. [Google Scholar] [CrossRef]
- Haas, E.J.; Angulo, F.J.; McLaughlin, J.M.; Anis, E.; Singer, S.R.; Khan, F.; Brooks, N.; Smaja, M.; Mircus, G.; Pan, K.; et al. Impact and effectiveness of mRNA BNT162b2 vaccine against SARS-CoV-2 infections and COVID-19 cases, hospitalisations, and deaths following a nationwide vaccination campaign in Israel: An observational study using national surveillance data. Lancet 2021, 397, 1819–1829. [Google Scholar] [CrossRef]
- Vasileiou, E.; Simpson, C.R.; Shi, T.; Kerr, S.; Agrawal, U.; Akbari, A.; Bedston, S.; Beggs, J.; Bradley, D.; Chuter, A.; et al. Interim findings from first-dose mass COVID-19 vaccination roll-out and COVID-19 hospital admissions in Scotland: A national prospective cohort study. Lancet 2021, 397, 1646–1657. [Google Scholar] [CrossRef]
- Gee, J.; Marquez, P.; Su, J.; Calvert, G.M.; Liu, R.; Myers, T.; Nair, N.; Martin, S.; Clark, T.; Markowitz, L.; et al. First Month of COVID-19 Vaccine Safety Monitoring—United States, December 14, 2020–January 13, 2021. MMWR Morb. Mortal Wkly. Rep. 2021, 70, 283–288. [Google Scholar] [CrossRef] [PubMed]
- Bae, S.; Lee, Y.W.; Lim, S.Y.; Lee, J.H.; Lim, J.S.; Lee, S.; Park, S.; Kim, S.K.; Lim, Y.J.; Kim, E.O.; et al. Adverse Reactions Following the First Dose of ChAdOx1 nCoV-19 Vaccine and BNT162b2 Vaccine for Healthcare Workers in South Korea. J. Korean Med. Sci. 2021, 36, e115. [Google Scholar] [CrossRef]
- Torjesen, I. Covid-19: Risk of cerebral blood clots from disease is 10 times that from vaccination, study finds. BMJ 2021, 373, n1005. [Google Scholar] [CrossRef]
- Taquet, M.; Husain, M.; Geddes, J.R.; Luciano, S.; Harrison, P.J. Cerebral Venous Thrombosis: A Retrospective Cohort Study of 513,284 Confirmed COVID-19 Cases and a Comparison with 489,871 People Receiving a COVID-19 mRNA Vaccine. Center for Open Science Preprint. 2021. Available online: https://osf.io/a9jdq/ (accessed on 8 June 2021).
- Kelly, B.J.; Southwell, B.G.; McCormack, L.A.; Bann, C.M.; MacDonald, P.D.M.; Frasier, A.M.; Bevc, C.A.; Brewer, N.T.; Squiers, L.B. Predictors of willingness to get a COVID-19 vaccine in the U.S. BMC Infect. Dis 2021, 21, 338. [Google Scholar] [CrossRef]
- Killgore, W.D.S.; Cloonan, S.A.; Taylor, E.C.; Dailey, N.S. The COVID-19 Vaccine Is Here-Now Who Is Willing to Get It? Vaccines 2021, 9, 339. [Google Scholar] [CrossRef] [PubMed]
- Nohl, A.; Afflerbach, C.; Lurz, C.; Brune, B.; Ohmann, T.; Weichert, V.; Zeiger, S.; Dudda, M. Acceptance of COVID-19 Vaccination among Front-Line Health Care Workers: A Nationwide Survey of Emergency Medical Services Personnel from Germany. Vaccines 2021, 9, 424. [Google Scholar] [CrossRef] [PubMed]
- Paul, E.; Steptoe, A.; Fancourt, D. Attitudes towards vaccines and intention to vaccinate against COVID-19: Implications for public health communications. Lancet Reg. Health Eur. 2021, 1, 100012. [Google Scholar] [CrossRef]
- Norwegian Medicines Agency. Report on Suspected Side Effects of SARS-CoV-2 Vaccines 2021. Available online: https://legemiddelverket.no/Documents/Bivirkninger%20og%20sikkerhet/Rapporter%20og%20oversikter/Koronavaksiner/20210408%20Rapport%20over%20meldte%20bivirkninger%20av%20koronavaksine.pdf (accessed on 8 June 2021).
- Mahase, E. Covid-19: Medical community split over vaccine interval policy as WHO recommends six weeks. BMJ 2021, 372, n226. [Google Scholar] [CrossRef]
- Reuters Staff. Second Vaccine Dose Can Be Delayed, Research Says—Italy’s AIFA Head to Paper. Reuters 2021. Available online: https://www.reuters.com/article/us-health-coronavirus-italy-aifa-idUSKBN2C00I4 (accessed on 8 June 2021).
- Iacobucci, G.; Mahase, E. Covid-19 vaccination: What’s the evidence for extending the dosing interval? BMJ 2021, 372, n18. [Google Scholar] [CrossRef]
- Pimenta, D.; Yates, C.; Pagel, C.; Gurdasani, D. Delaying the second dose of covid-19 vaccines. BMJ 2021, 372, n710. [Google Scholar] [CrossRef]
- Parry, H.; Bruton, R.; Stephens, C.; Brown, K.; Amirthalingam, G.; Hallis, B.; Otter, A.; Zuo, J.; Moss, P. Extended interval BNT162b2 vaccination enhances peak antibody generation in older people. MedRxiv 2021. [Google Scholar] [CrossRef]
- Abdool Karim, S.S.; de Oliveira, T. New SARS-CoV-2 Variants—Clinical, Public Health, and Vaccine Implications. N. Engl. J. Med. 2021, 384, 1866–1868. [Google Scholar] [CrossRef]
- Planas, D.; Bruel, T.; Grzelak, L.; Guivel-Benhassine, F.; Staropoli, I.; Porrot, F.; Planchais, C.; Buchrieser, J.; Rajah, M.M.; Bishop, E.; et al. Sensitivity of infectious SARS-CoV-2 B.1.1.7 and B.1.351 variants to neutralizing antibodies. Nat. Med. 2021, 27, 917–924. [Google Scholar] [CrossRef]
- Stamatatos, L.; Czartoski, J.; Wan, Y.H.; Homad, L.J.; Rubin, V.; Glantz, H.; Neradilek, M.; Seydoux, E.; Jennewein, M.F.; MacCamy, A.J.; et al. mRNA vaccination boosts cross-variant neutralizing antibodies elicited by SARS-CoV-2 infection. Science 2021. [Google Scholar] [CrossRef]
- Italian National Institute of Health. COVID-19 Vaccines FAQ. Available online: https://www.iss.it/covid19-faq/ (accessed on 2 June 2021).
- Robertson, E.; Reeve, K.S.; Niedzwiedz, C.L.; Moore, J.; Blake, M.; Green, M.; Katikireddi, S.V.; Benzeval, M.J. Predictors of COVID-19 vaccine hesitancy in the UK household longitudinal study. Brain Behav. Immun. 2021, 94, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Troiano, G.; Nardi, A. Vaccine hesitancy in the era of COVID-19. Public Health 2021, 194, 245–251. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Lu, X.; Lai, X.; Lyu, Y.; Zhang, H.; Fenghuang, Y.; Jing, R.; Li, L.; Yu, W.; Fang, H. The Changing Acceptance of COVID-19 Vaccination in Different Epidemic Phases in China: A Longitudinal Study. Vaccines 2021, 9, 191. [Google Scholar] [CrossRef] [PubMed]
- Freeman, D.; Loe, B.S.; Yu, L.M.; Freeman, J.; Chadwick, A.; Vaccari, C.; Shanyinde, M.; Harris, V.; Waite, F.; Rosebrock, L.; et al. Effects of different types of written vaccination information on COVID-19 vaccine hesitancy in the UK (OCEANS-III): A single-blind, parallel-group, randomised controlled trial. Lancet Public Health 2021. [Google Scholar] [CrossRef]


{kind=link}
| Overall Sample | ≥1 Vaccine Dose | Unvaccinated | ||
|---|---|---|---|---|
| Variables | (n = 245,226) | (n = 69,539) | (n = 175,687) | p * |
| Mean age in years (SD) | 53.2 (19.8) | 67.6 (16.7) | 47.5 (18.0) | <0.001 |
| Male gender, % | 47.9 | 43.1 | 49.7 | <0.001 |
| Priority category, % A | ||||
| - Elderly | 35.8 | 70.2 | 22.2 | <0.001 |
| - Fragile individuals | 2.5 | 8.7 | -- | -- |
| - School workers | 2.2 | 7.7 | -- | -- |
| - Healthcare workers | 1.9 | 6.9 | -- | -- |
| - Armed forces and civil operators | 1.1 | 4.1 | -- | -- |
| - Others | 0.7 | 2.4 | -- | -- |
| - Unknown | 55.7 | 0.0 | 77.8 | <0.001 |
| Risk factors and comorbidities B | ||||
| - Hypertension | 13.9 | 30.4 | 7.4 | <0.001 |
| - Diabetes | 5.8 | 12.6 | 3.1 | <0.001 |
| - Major cardio/cerebrovascular diseases | 7.1 | 15.2 | 3.8 | <0.001 |
| - COPD | 3.0 | 5.1 | 2.1 | <0.001 |
| - Kidney diseases | 1.9 | 3.5 | 1.3 | <0.001 |
| - Cancer | 5.0 | 10.3 | 3.0 | <0.001 |
| N. of vaccine doses, % C | ||||
| - One or two (n = 69,539) | 28.4 | 100.0 | -- | -- |
| - One only (n = 36,684) | 15.0 | 52.8 | -- | -- |
| - Two (n = 32,855) | 13.4 | 47.2 | -- | -- |
| Vaccine type-1st dose, % C | ||||
| - BNT162b2 (n = 47,654) | 19.4 | 68.5 | -- | -- |
| - ChAdOx1 nCoV-19 (n = 16,997) | 6.9 | 24.4 | -- | -- |
| - mRNA-1273 (n = 4888) | 2.0 | 7.0 | -- | -- |
| - None (n = 175,687) | 71.6 | -- | 100.0 | -- |
| Vaccine type-2nd dose D | ||||
| - BNT162b2 (n = 30,817) | 12.6 | 93.8 | -- | -- |
| - ChAdOx1 nCoV-19 (n = 18) | 0.0 | 0.1 | -- | -- |
| - mRNA-1273 (n = 2020) | 0.8 | 6.1 | -- | -- |
| - None (n = 212,371) | 86.6 | -- | 100.0 | -- |
| Average days between the start of the follow-up and SARS-CoV infection, (SD) E | 98 (43) | 38 (29) | 122 (17) | <0.001 |
| Average days between the start of the follow-up and COVID-19, (SD) F | 100 (42) | 38 (29) | 125 (6) | <0.001 |
| Average days between the start of the follow-up and death, (SD) G | 100 (42) | 38 (29) | 125 (3) | <0.001 |
| SARS-CoV-2 positive swab, % (n) D | 2.87 (7033) | 0.12 (85) | 4.00 (6948) | <0.001 |
| Covid-19 disease, % (n) D | 0.39 (951) | 0.03 (18) | 0.53 (933) | <0.001 |
| Death, % (n) D | 0.10 (244) | 0.00 (3) | 0.14 (241) | <0.001 |
| Cox Model * | SARS-CoV-2 | COVID-19 | Death |
|---|---|---|---|
| HR (95% CI) | HR (95% CI) | HR (95% CI) | |
| ≥1 Vaccine dose vs. none A | |||
| - None (n = 175,687) | 1 (Ref. cat.) | 1 (Ref. cat.) | 1 (Ref. cat.) |
| - All vaccines (n = 69,539) | 0.05 (0.04–0.06) | 0.04 (0.02–0.06) | 0.03 (0.01–0.08) |
| - BNT162b2 (n = 47,654) | 0.05 (0.04–0.07) | 0.05 (0.03–0.08) | 0.03 (0.01–0.09) |
| - ChAdOx1 nCoV-19 (n = 16,997) | 0.05 (0.03–0.08) | 0.00 (NE) | 0.00 (NE) |
| - mRNA-1273 (n = 4888) | 0.02 (0.01–0.07) | 0.00 (NE) | 0.00 (NE) |
| Only one vaccine dose vs. none B | |||
| - None (n = 175,687) | 1 (Ref. cat.) | 1 (Ref. cat.) | 1 (Ref. cat.) |
| - All vaccines (n = 36,684) | 0.16 (0.13–0.20) | 0.31 (0.19–0.49) | 0.27 (0.07–1.10) |
| - BNT162b2 (n = 16,837) | 0.45 (0.34–0.60) | NE ψ | NE ψ |
| - ChAdOx1 nCoV-19 (n = 16,979) | 0.05 (0.03–0.08) | 0.00 (NE) | 0.00 (NE) |
| - mRNA-1273 (n = 2868) | 0.07 (0.02–0.26) | NE ψ | NE ψ |
| Two vaccine doses only vs. none C | |||
| - None (n = 174,023) | 1 (Ref. cat.) | 1 (Ref. cat.) | 1 (Ref. cat.) |
| - All vaccines (n = 32,855) | 0.02 (0.01–0.03) | 0.01 (0.00–0.04) | 0.02 (0.00–0.12) |
| - BNT162b2 (n = 30,817) | 0.02 (0.01–0.04) | 0.01 (0.00–0.04) | 0.02 (0.00–0.13) |
| - ChAdOx1 nCoV-19 (n = 18) | -- | -- | -- |
| - mRNA-1273 (n = 2020) | 0.00 (NE) | 0.00 (NE) | 0.00 (NE) |
| Variables | Overall Sample | ≥1 Vaccine Dose | Unvaccinated |
|---|---|---|---|
| SARS-CoV-2 positive swab, % (n) A | |||
| - Females (n = 127,839) | 2.76 (3527) | 0.13 (53) | 3.93 (3474) |
| - Males (n = 117,387) | 2.99 (3506) | 0.11 (32) | 3.97 (3474) |
| Covid-19 disease, % (n) A | |||
| - Females | 0.31 (401) | 0.03 (12) | 0.44 (389) |
| - Males | 0.47 (550) | 0.02 (6) | 0.62 (544) |
| Death, % (n) A | |||
| - Females | 0.09 (109) | 0.01 (2) | 0.12 (107) |
| - Males | 0.12 (135) | 0.00 (1) | 0.15 (134) |
| Cox model * | SARS-CoV-2 | COVID-19 | Death |
| HR (95% CI) | HR (95% CI) | HR (95% CI) | |
| ≥1 Vaccine dose vs. none B | |||
| - Females (n = 39,550) | 0.06 (0.04–0.08) | 0.06 (0.03–0.11) | 0.04 (0.01–0.15) |
| - Males (n = 29,989) | 0.04 (0.03–0.06) | 0.02 (0.01–0.05) | 0.02 (0.00–0.11) |
| Only one vaccine dose vs. none C | |||
| - Females (n = 20,529) | 0.16 (0.12–0.22) | 0.44 (0.24–0.79) | 0.28 (0.04–2.04) |
| - Males (n = 16,155) | 0.16 (0.11–0.23) | 0.20 (0.09–0.44) | 0.27 (0.04–1.94) |
| Two vaccine doses only vs. none D | |||
| - Females (n = 19,021) | 0.03 (0.02–0.05) | 0.01 (0.00–0.06) | 0.04 (0.01–0.27) |
| - Males (n = 13,834) | 0.01 (0.01–0.03) | 0.00 (NE) | 0.00 (NE) |
| Variables | Recommended Schedule * | Delayed Schedule * | p ** |
|---|---|---|---|
| (n = 32,164; 97.9%) | (n = 691; 2.1%) | ||
| SARS-CoV-2 positive swab, % (n) A | 0.05 (17) | 0.00 (0) | 0.5 |
| Covid-19 disease, % (n) A | 0.00 (1) | 0.00 (0) | 0.9 |
| Death, % (n) A | 0.00 (1) | 0.00 (0) | 0.9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Flacco, M.E.; Soldato, G.; Acuti Martellucci, C.; Carota, R.; Di Luzio, R.; Caponetti, A.; Manzoli, L. Interim Estimates of COVID-19 Vaccine Effectiveness in a Mass Vaccination Setting: Data from an Italian Province. Vaccines 2021, 9, 628. https://doi.org/10.3390/vaccines9060628
Flacco ME, Soldato G, Acuti Martellucci C, Carota R, Di Luzio R, Caponetti A, Manzoli L. Interim Estimates of COVID-19 Vaccine Effectiveness in a Mass Vaccination Setting: Data from an Italian Province. Vaccines. 2021; 9(6):628. https://doi.org/10.3390/vaccines9060628
Chicago/Turabian StyleFlacco, Maria Elena, Graziella Soldato, Cecilia Acuti Martellucci, Roberto Carota, Rossano Di Luzio, Antonio Caponetti, and Lamberto Manzoli. 2021. "Interim Estimates of COVID-19 Vaccine Effectiveness in a Mass Vaccination Setting: Data from an Italian Province" Vaccines 9, no. 6: 628. https://doi.org/10.3390/vaccines9060628