
User Participatory Design of a Wearable Focal Vibration Device for Home-Based Stroke Rehabilitation

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design Approach
2.2. Design Requirements
- (1)
- Individualized shape molding around the whole arm with six vibration motors to deliver vibratory stimuli in six different muscle locations.
- (2)
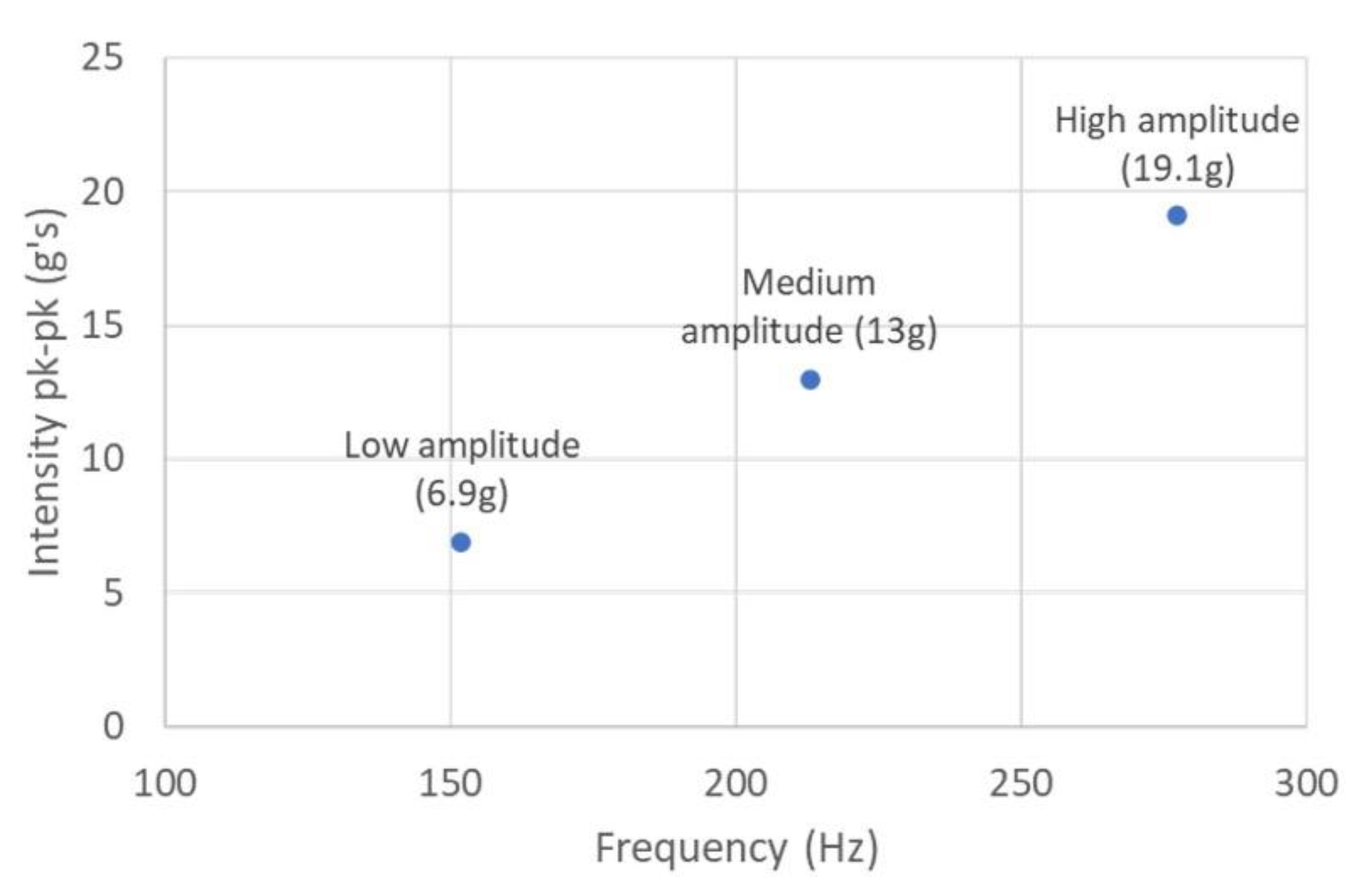
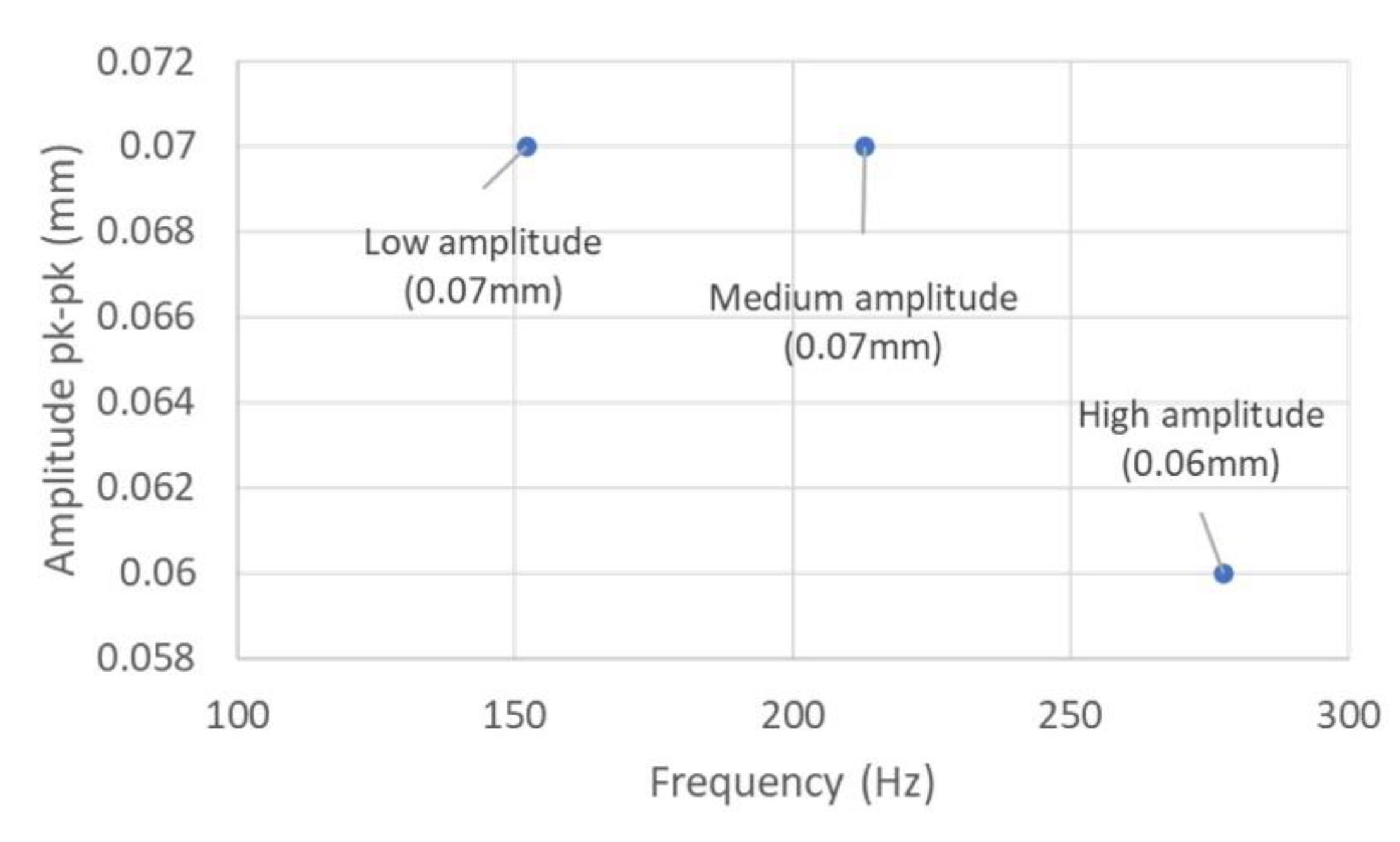
- Each vibration motor delivers a frequency between 60–300 Hz and amplitude between 0.1–10 mm.
- (3)
- Controllable activation and deactivation of each vibration motor and adjustable vibration parameters.
- (4)
- The FoVi should be comfortable, easy to wear, affordable, and flexible.
- (5)
- Easy to use interface for therapists to track the device usage and remotely adjust the vibration intensity and dosage. Based on rehabilitation progress, the therapist needs to change the settings to enable optimum recovery for the stroke survivors.
- (6)
- Rechargeable, with a battery lasting for at least 30 min.
3. Results
3.1. Iterative Design Process
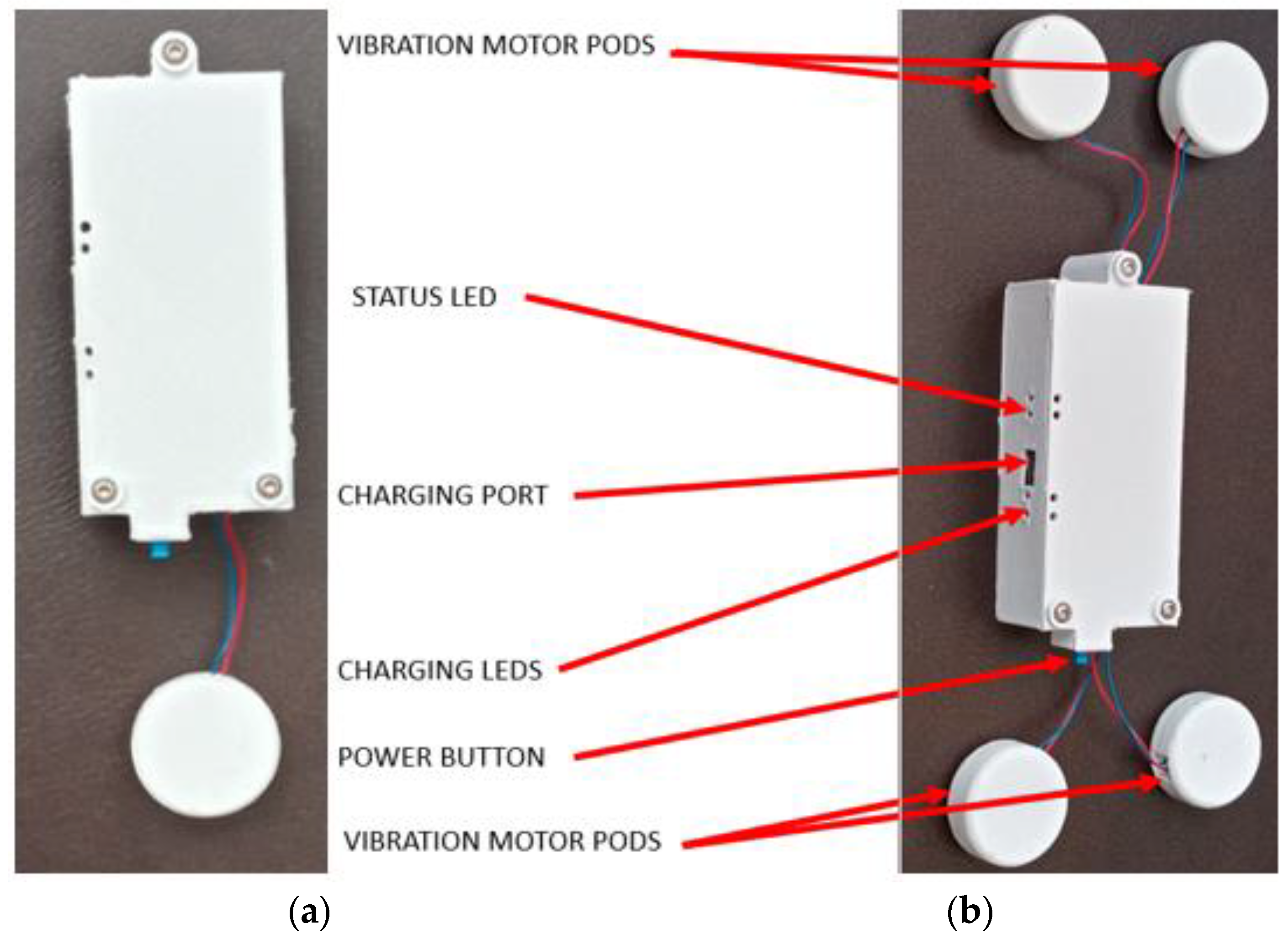
3.2. Vibration Pod Design
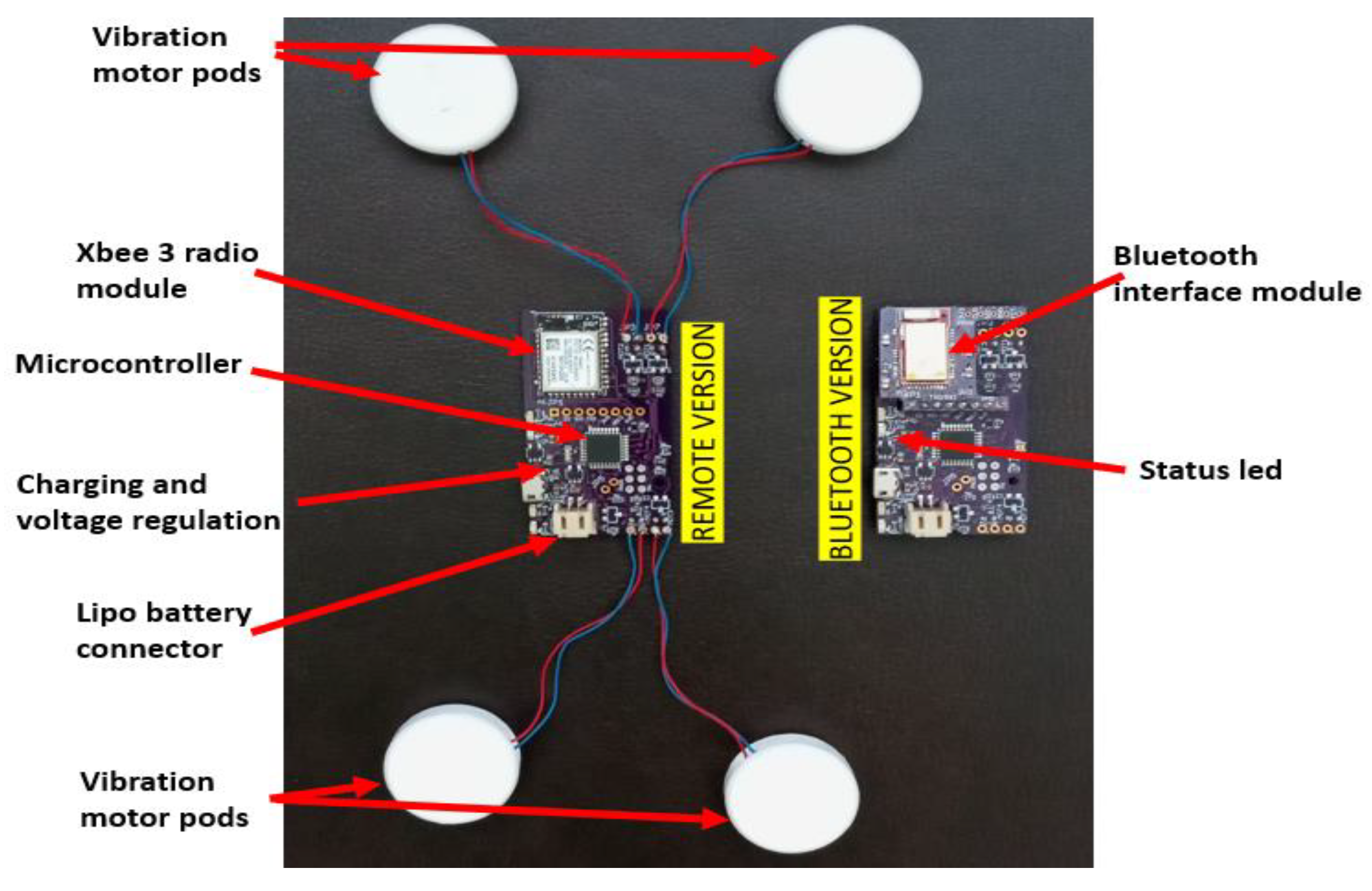
3.3. Electronics Design
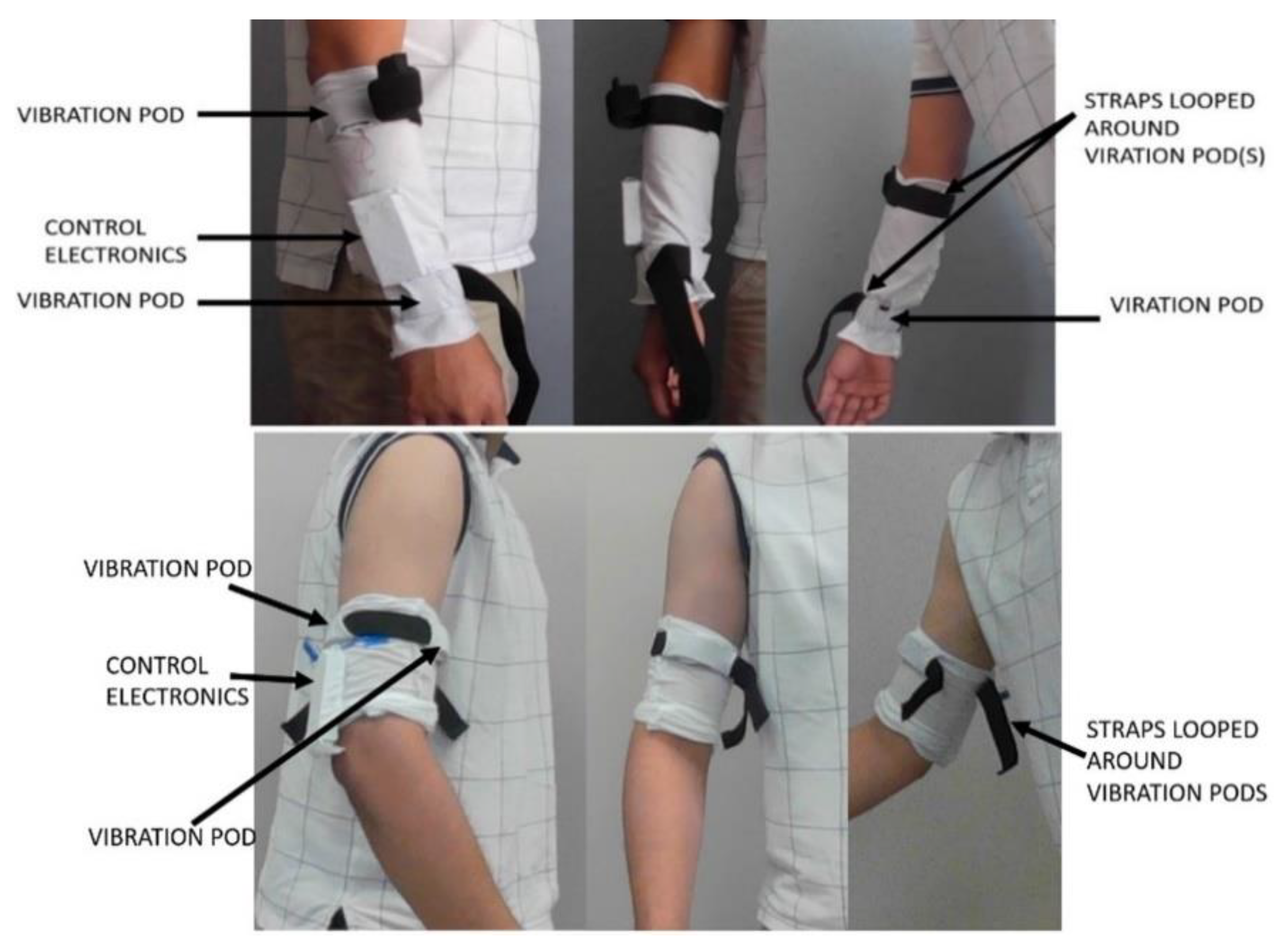
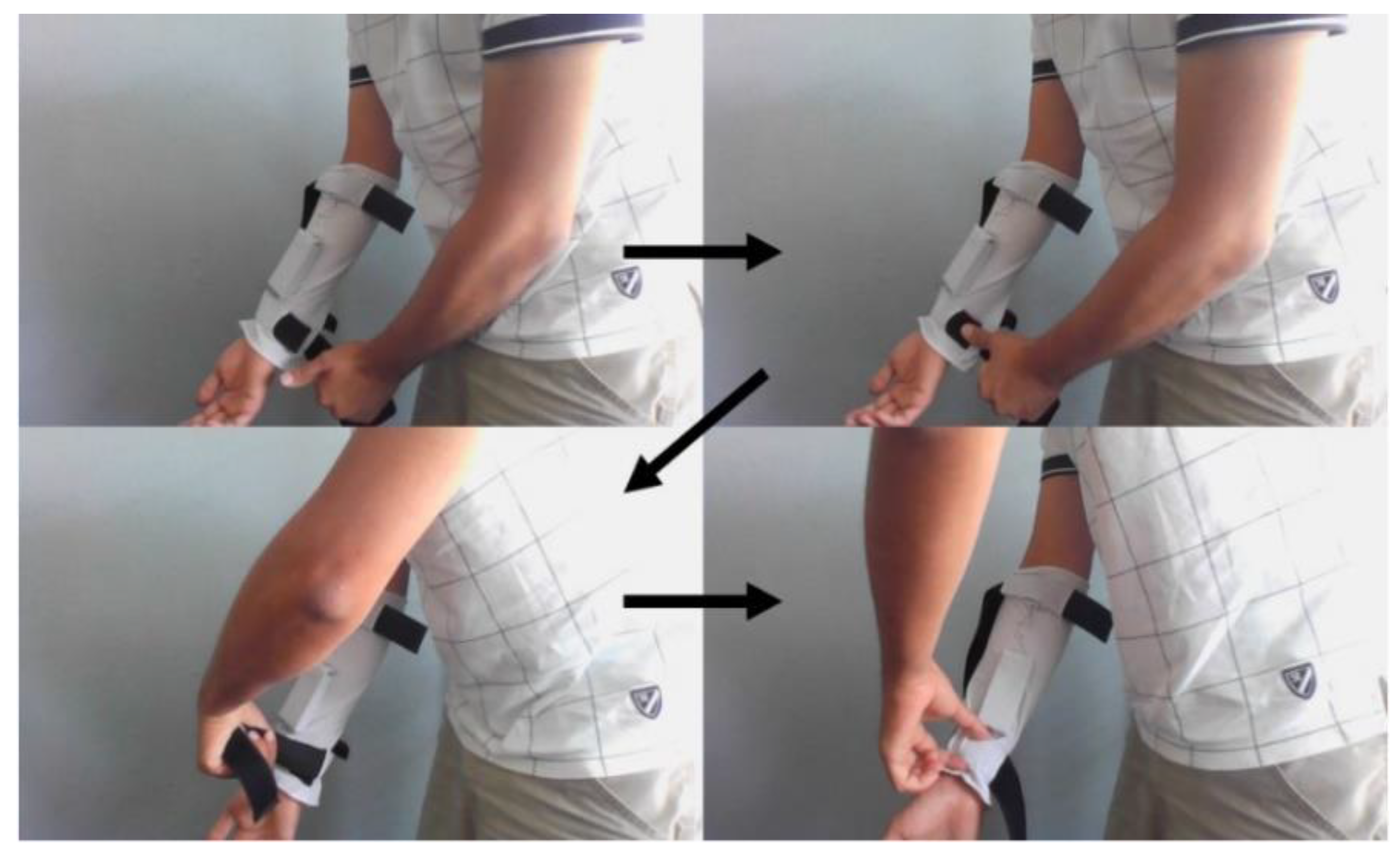
3.4. Ergonomics and Sleeve Design
3.5. Interface and Webportal
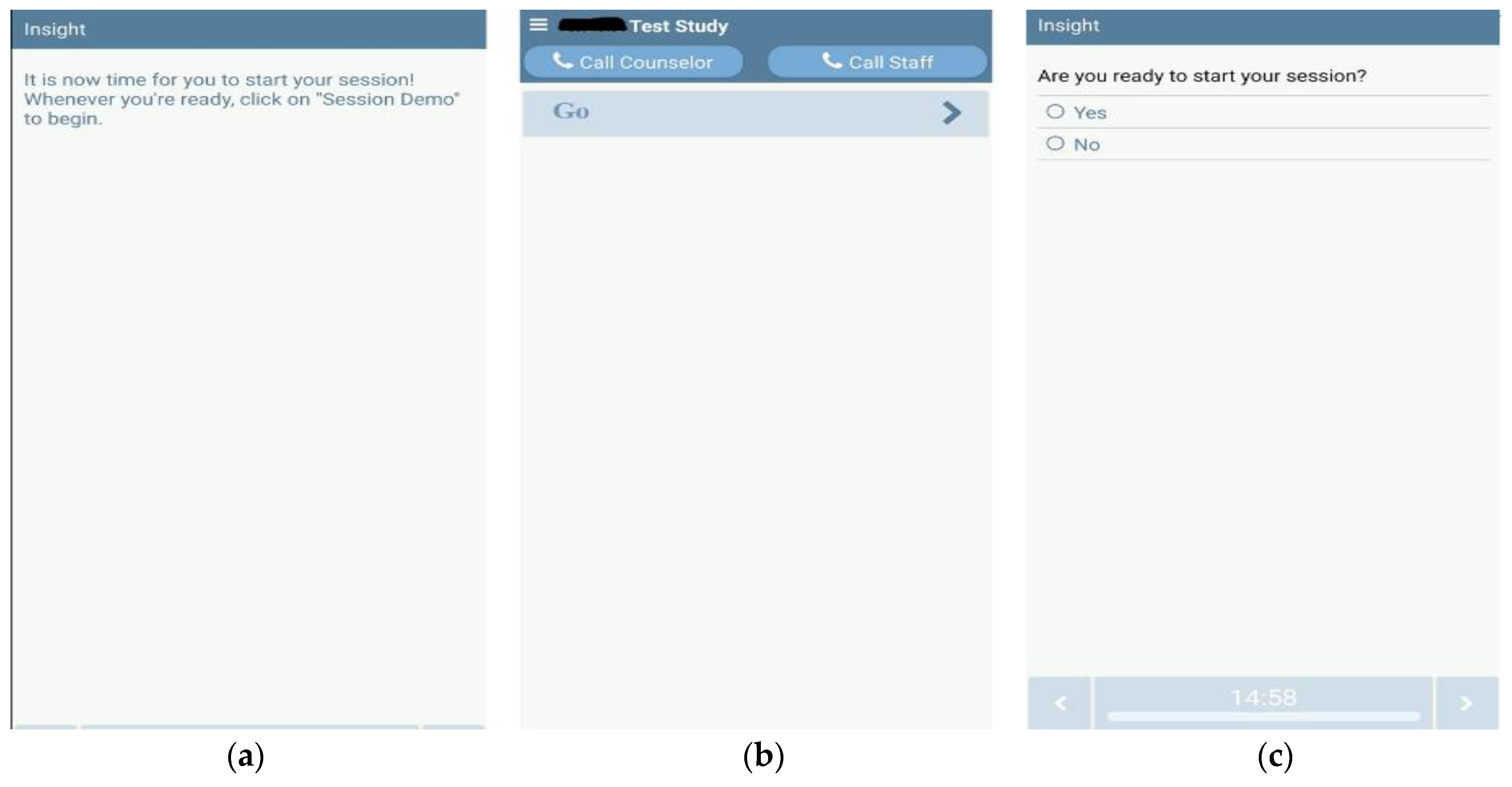
3.5.1. User Interface (Smartphone App via Bluetooth)
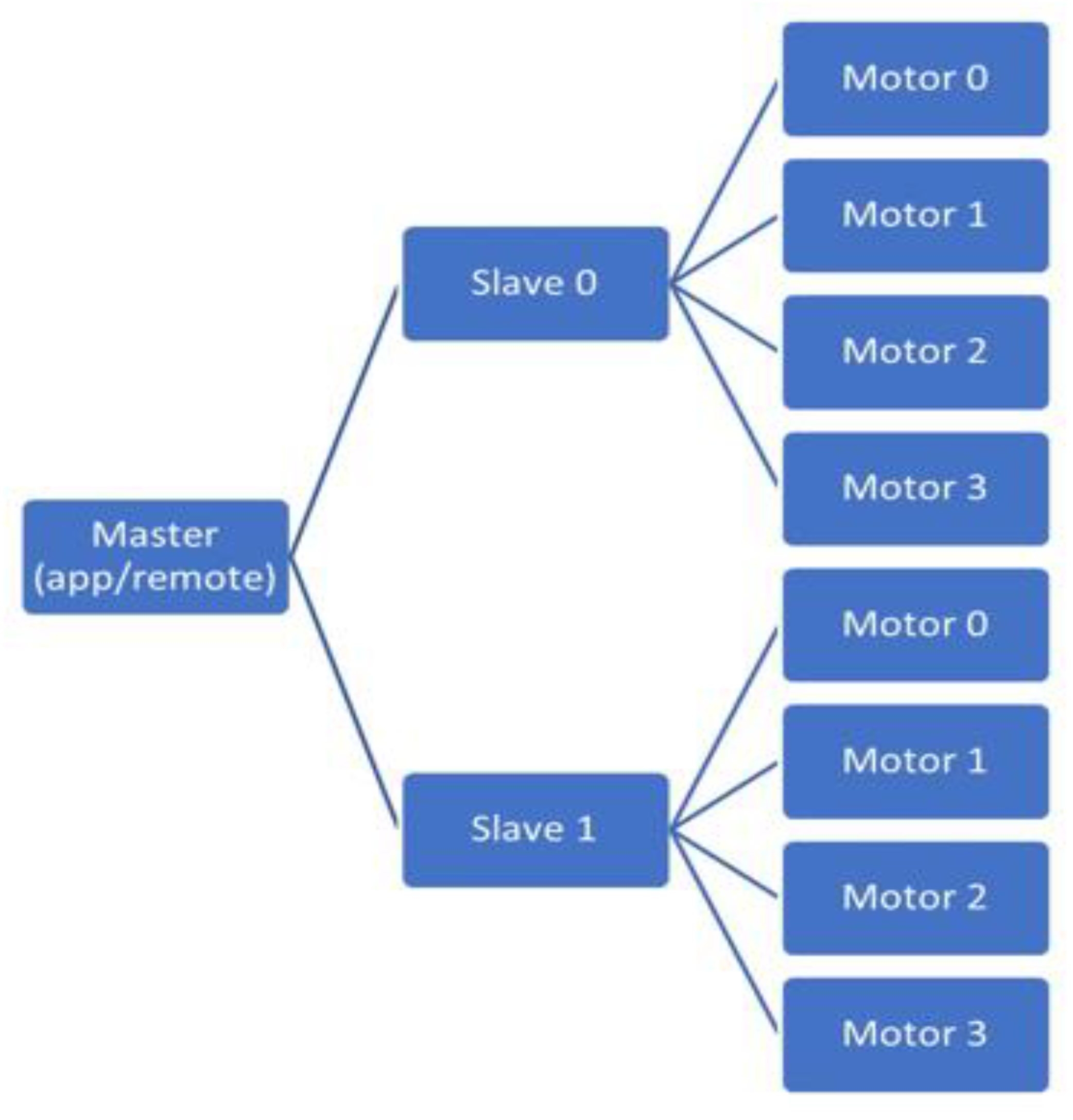
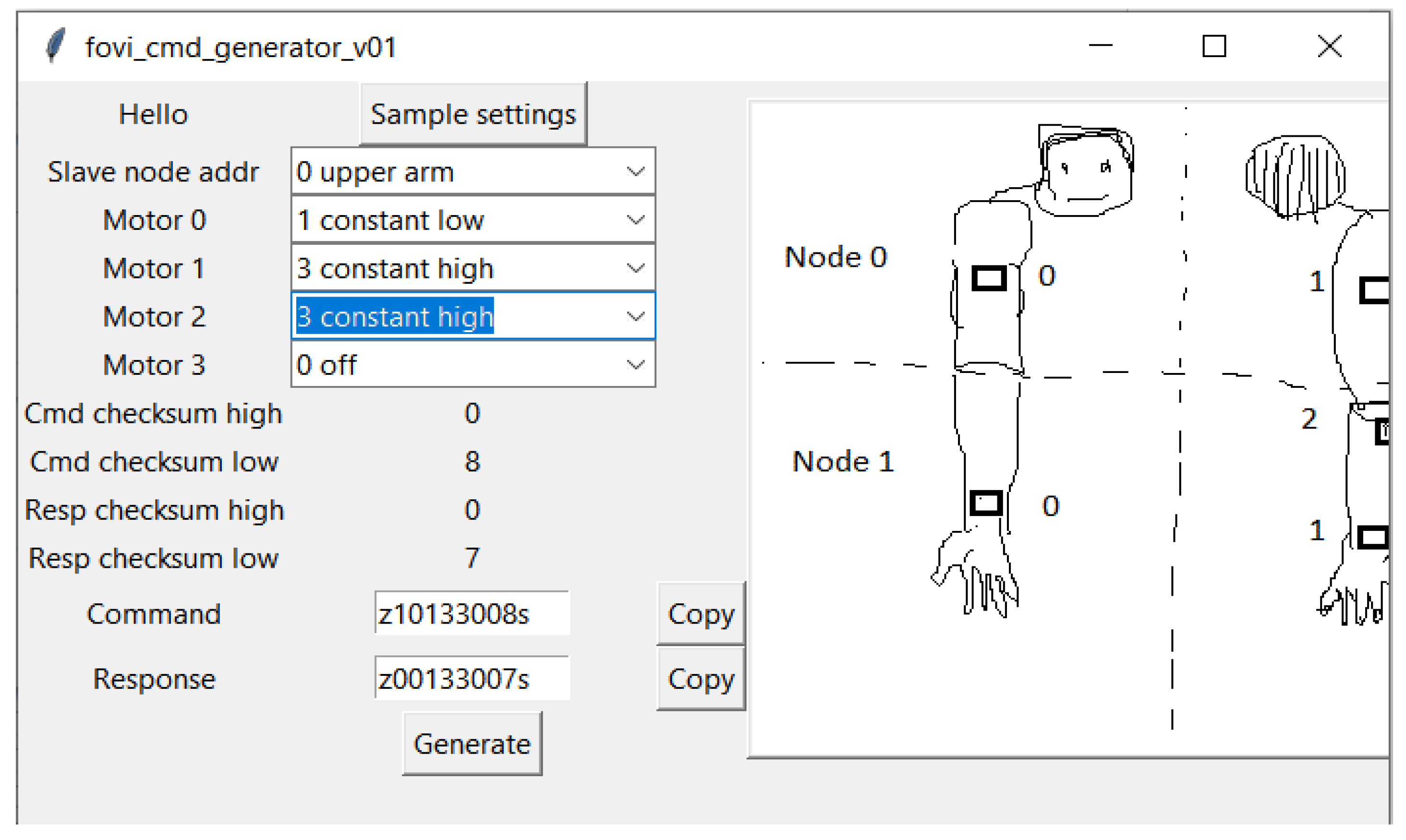
3.5.2. User Interface (Remote via Xbee)
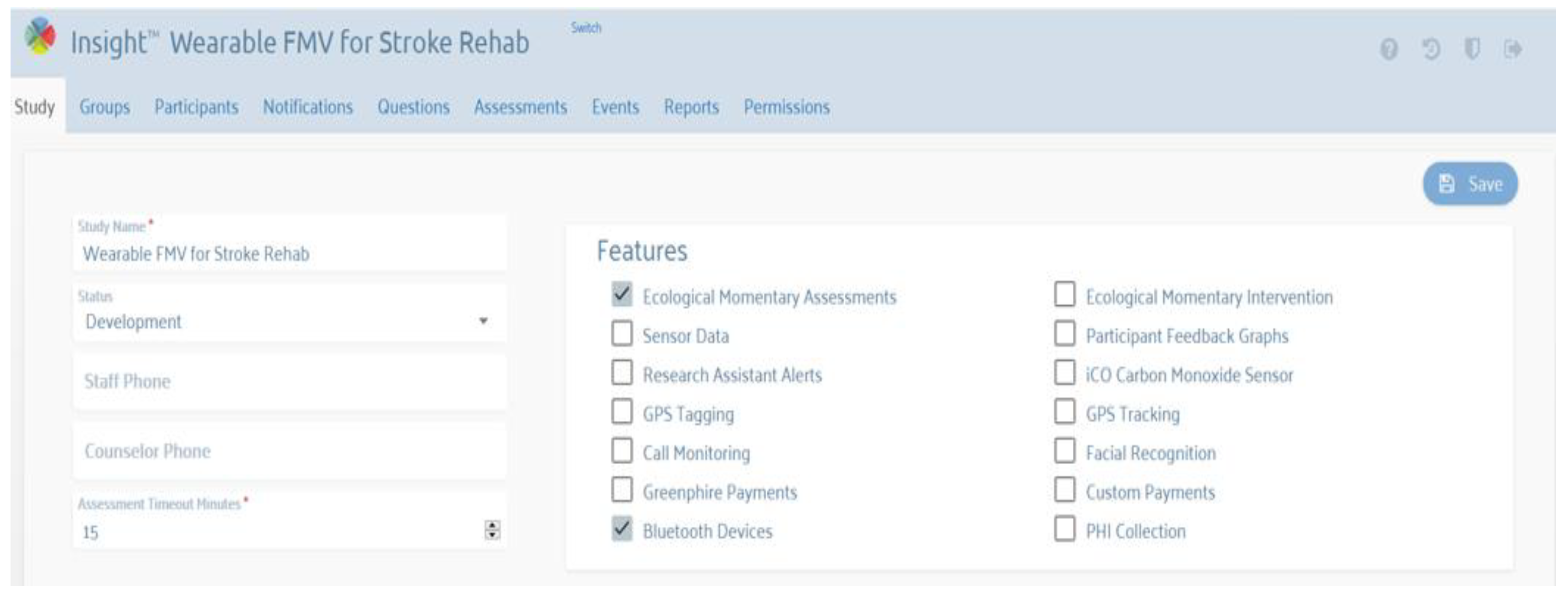
3.5.3. Therapist Interface (Web Portal)
- Set slave 0 motors 0 and 1 to 80% intensity, and set all others to off (for 5 min);
- Set all motors to off (for a 5 min break);
- Set slave one motors 0, 1, and 3 to 50% intensity, and set all others to off (for 5 min);
- Set all motors to off (for a 5 min break);
- Set slave 0 motors 0 and 1 to 80% intensity, and set all others to off (for 5 min);
- Set all motors to off (end of session).
3.6. Initial Test and User Evaluation
4. Discussion
5. Conclusions and Future Research
6. Patents
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Langhorne, P.; Bernhardt, J.; Kwakkel, G. Stroke rehabilitation. Lancet 2011, 377, 1693–1702. [Google Scholar] [CrossRef]
- Jorgensen, H.S.; Nakayama, H.; Raaschou, H.O.; Olsen, T.S. Stroke. Neurologic and functional recovery the Copenhagen Stroke Study. Phys. Med. Rehabil. Clin. N. Am. 1999, 10, 887–906. [Google Scholar] [CrossRef]
- Kwakkel, G.; Kollen, B.J.; van der Grond, J.; Prevo, A.J. Probability of regaining dexterity in the flaccid upper limb: Impact of severity of paresis and time since onset in acute stroke. Stroke 2003, 34, 2181–2186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simonsick, E.M.; Kasper, J.D.; Guralnik, J.M.; Bandeen-Roche, K.; Ferrucci, L.; Hirsch, R.; Leveille, S.; Rantanen, T.; Fried, L.P. Severity of upper and lower extremity functional limitation: Scale development and validation with self-report and performance-based measures of physical function. WHAS Research Group. Women’s Health and Aging Study. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2001, 56, S10–S19. [Google Scholar]
- Clarke, P.; Black, S.E. Quality of Life Following Stroke: Negotiating Disability, Identity, and Resources. J. Appl. Gerontol. 2005, 24, 319–336. [Google Scholar] [CrossRef]
- Franceschini, M.; La Porta, F.; Agosti, M.; Massucci, M. Is health-related-quality of life of stroke patients influenced by neurological impairments at one year after stroke? Eur. J. Phys. Rehabil. Med. 2010, 46, 389–399. [Google Scholar]
- Wyller, T.B.; Sveen, U.; Sodring, K.M.; Pettersen, A.M.; Bautz-Holter, E. Subjective well-being one year after stroke. Clin. Rehabil. 1997, 11, 139–145. [Google Scholar] [CrossRef]
- Juckett, L.A.; Wengerd, L.R.; Faieta, J.; Griffin, C.E. Evidence-Based Practice Implementation in Stroke Rehabilitation: A Scoping Review of Barriers and Facilitators. Am. J. Occup. Ther. 2019, 74, 7401205050p1–7401205050p14. [Google Scholar] [CrossRef]
- Stinear, C.M.; Lang, C.E.; Zeiler, S.; Byblow, W.D. Advances and challenges in stroke rehabilitation. Lancet Neurol. 2020, 19, 348–360. [Google Scholar] [CrossRef]
- Gowland, C.; Stratford, P.; Ward, M.; Moreland, J.; Torresin, W.; Van Hullenaar, S.; Sanford, J.; Barreca, S.; Vanspall, B.; Plews, N. Measuring physical impairment and disability with the Chedoke-McMaster Stroke Assessment. Stroke 1993, 24, 58–63. [Google Scholar] [CrossRef] [Green Version]
- Bayley, M.T.; Hurdowar, A.; Richards, C.L.; Korner-Bitensky, N.; Wood-Dauphinee, S.; Eng, J.J.; McKay-Lyons, M.; Harrison, E.; Teasell, R.; Harrison, M.; et al. Barriers to implementation of stroke rehabilitation evidence: Findings from a multi-site pilot project. Disabil. Rehabil. 2012, 34, 1633–1638. [Google Scholar] [CrossRef] [PubMed]
- Lang, C.E.; Lohse, K.R.; Birkenmeier, R.L. Dose and timing in neurorehabilitation: Prescribing motor therapy after stroke. Curr. Opin. Neurol. 2015, 28, 549–555. [Google Scholar] [PubMed] [Green Version]
- Celletti, C.; Camerota, F. Preliminary evidence of focal muscle vibration effects on spasticity due to cerebral palsy in a small sample of Italian children. Clin. Ter. 2011, 162, e125-8. [Google Scholar] [PubMed]
- Paoloni, M.; Giovannelli, M.; Mangone, M.; Leonardi, L.; Tavernese, E.; Di Pangrazio, E.; Bernetti, A.; Santilli, V.; Pozzilli, C. Does giving segmental muscle vibration alter the response to botulinum toxin injections in the treatment of spasticity in people with multiple sclerosis? A single-blind randomized controlled trial. Clin. Rehabil. 2013, 27, 803–812. [Google Scholar] [CrossRef]
- Sadeghi, M.; Sawatzky, B. Effects of vibration on spasticity in individuals with spinal cord injury: A scoping systematic review. Am. J. Phys. Med. Rehabil. 2014, 93, 995–1007. [Google Scholar] [CrossRef]
- Seo, H.G.; Oh, B.M.; Leigh, J.H.; Chun, C.; Park, C.; Kim, C.H. Effect of Focal Muscle Vibration on Calf Muscle Spasticity: A Proof-of-Concept Study. PM R J. Inj. Funct. Rehabil. 2016, 8, 1083–1089. [Google Scholar] [CrossRef]
- Marconi, B.; Filippi, G.M.; Koch, G.; Pecchioli, C.; Salerno, S.; Don, R.; Camerota, F.; Saraceni, V.M.; Caltagirone, C. Long-term effects on motor cortical excitability induced by repeated muscle vibration during contraction in healthy subjects. J. Neurol. Sci. 2008, 275, 51–59. [Google Scholar] [CrossRef]
- Ribot-Ciscar, E.; Butler, J.E.; Thomas, C.K. Facilitation of triceps brachii muscle contraction by tendon vibration after chronic cervical spinal cord injury. J. Appl. Physiol. 2003, 94, 2358–2367. [Google Scholar] [CrossRef] [Green Version]
- Cordo, P.; Gurfinkel, V.S.; Bevan, L.; Kerr, G.K. Proprioceptive consequences of tendon vibration during movement. J. Neurophysiol. 1995, 74, 1675–1688. [Google Scholar]
- Bento, V.F.; Cruz, V.T.; Ribeiro, D.D.; Cunha, J.P. The vibratory stimulus as a neurorehabilitation tool for stroke patients: Proof of concept and tolerability test. NeuroRehabilitation 2012, 30, 287–293. [Google Scholar] [CrossRef]
- Conrad, M.O.; Scheidt, R.A.; Schmit, B.D. Effects of wrist tendon vibration on arm tracking in people poststroke. J. Neurophysiol. 2011, 106, 1480–1488. [Google Scholar]
- Murillo, N.; Valls-Sole, J.; Vidal, J.; Opisso, E.; Medina, J.; Kumru, H. Focal vibration in neurorehabilitation. Eur. J. Phys. Rehabil. Med. 2014, 50, 231–242. [Google Scholar]
- Conrad, M.O.; Scheidt, R.A.; Schmit, B.D. Effects of wrist tendon vibration on targeted upper-arm movements in poststroke hemiparesis. Neurorehabilit. Neural Repair 2011, 25, 61–70. [Google Scholar] [CrossRef] [PubMed]
- Paoloni, M.; Tavernese, E.; Fini, M.; Sale, P.; Franceschini, M.; Santilli, V.; Mangone, M. Segmental muscle vibration modifies muscle activation during reaching in chronic stroke: A pilot study. NeuroRehabilitation 2014, 35, 405–414. [Google Scholar] [PubMed]
- Calabrò, R.S.; Naro, A.; Russo, M.; Milardi, D.; Leo, A.; Filoni, S.; Trinchera, A.; Bramanti, P. Is two better than one? Muscle vibration plus robotic rehabilitation to improve upper limb spasticity and function: A pilot randomized controlled trial. PLoS ONE 2017, 12, e0185936. [Google Scholar] [CrossRef] [PubMed]
- Caliandro, P.; Celletti, C.; Padua, L.; Minciotti, I.; Russo, G.; Granata, G.; La Torre, G.; Granieri, E.; Camerota, F. Focal muscle vibration in the treatment of upper limb spasticity: A pilot randomized controlled trial in patients with chronic stroke. Arch. Phys. Med. Rehabil. 2012, 93, 1656–1661. [Google Scholar] [CrossRef] [PubMed]
- Casale, R.; Damiani, C.; Maestri, R.; Fundaro, C.; Chimento, P.; Foti, C. Localized 100 Hz vibration improves function and reduces upper limb spasticity: A double-blind controlled study. Eur. J. Phys. Rehabil. Med. 2014, 50, 495–504. [Google Scholar] [PubMed]
- Celletti, C.; Sinibaldi, E.; Pierelli, F.; Monari, G.; Camerota, F. Focal Muscle Vibration and Progressive Modular Rebalancing with neurokinetic facilitations in post- stroke recovery of upper limb. Clin. Ter. 2017, 168, e33–e36. [Google Scholar]
- Etoh, S.; Noma, T.; Takiyoshi, Y.; Arima, M.; Ohama, R.; Yokoyama, K.; Hokazono, A.; Amano, Y.; Shimodozono, M.; Kawahira, K. Effects of repetitive facilitative exercise with neuromuscular electrical stimulation, vibratory stimulation and repetitive transcranial magnetic stimulation of the hemiplegic hand in chronic stroke patients. Int. J. Neurosci. 2016, 126, 1007–1012. [Google Scholar] [CrossRef]
- Liepert, J.; Binder, C. Vibration-induced effects in stroke patients with spastic hemiparesis—A pilot study. Restor. Neurol. Neurosci. 2010, 28, 729–735. [Google Scholar] [CrossRef]
- Marconi, B.; Filippi, G.M.; Koch, G.; Giacobbe, V.; Pecchioli, C.; Versace, V.; Camerota, F.; Saraceni, V.M.; Caltagirone, C. Long-term effects on cortical excitability and motor recovery induced by repeated muscle vibration in chronic stroke patients. Neurorehabilit. Neural Repair 2011, 25, 48–60. [Google Scholar] [CrossRef] [PubMed]
- Noma, T.; Matsumoto, S.; Shimodozono, M.; Etoh, S.; Kawahira, K. Anti-spastic effects of the direct application of vibratory stimuli to the spastic muscles of hemiplegic limbs in post-stroke patients: A proof-of-principle study. J. Rehabil. Med. 2012, 44, 325–330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jung, S.-M. The effects of vibratory stimulation employed to forearm and arm flexor muscles on upper limb function in patients with chronic stroke. J. Phys. Ther. Sci. 2017, 29, 1620–1622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costantino, C.; Galuppo, L.; Romiti, D. Short-term effect of local muscle vibration treatment versus sham therapy on upper limb in chronic post-stroke patients: A randomized controlled trial. Eur. J. Phys. Rehabil. Med. 2017, 53, 32–40. [Google Scholar] [CrossRef]
- Wang, H.; Chandrashekhar, R.; Rippetoe, J.; Ghazi, M. Focal Muscle Vibration for Stroke Rehabilitation: A Review of Vibration Parameters and Protocols. Appl. Sci. 2020, 10, 8270. [Google Scholar] [CrossRef]
- MyoVolt MyoVolt: Wearable Vibration Therapy. Available online: https://myovolt.com/wearable-vibration-therapy (accessed on 10 March 2022).
- Chandrashekhar, R.; Wang, H.; Dionne, C.; James, S.; Burzycki, J. Wearable Focal Muscle Vibration on Pain, Balance, Mobility, and Sensation in Individuals with Diabetic Peripheral Neuropathy: A Pilot Study. Int. J. Environ. Res. Public Health 2021, 18, 2415. [Google Scholar] [CrossRef]
- Rippetoe, J.; Wang, H.; James, S.A.; Dionne, C.; Block, B.; Beckner, M. Improvement of Gait after 4 Weeks of Wearable Focal Muscle Vibration Therapy for Individuals with Diabetic Peripheral Neuropathy. J. Clin. Med. 2020, 9, 3767. [Google Scholar] [CrossRef]
- Wang, H.; Dionne, C.; Anadani, N.A.; Brown, S.C.; Shuping, M.; Wilson, L. An Exploratory Study of Wearable Vibration Therapy on Gait and Mobility in People with Multiple Sclerosis. In Assistive Technology; Taylor & Francis Inc.: Philadelphia, PA, USA, 2021; p. 159. [Google Scholar]
- Daveler, B.; Salatin, B.; Grindle, G.G.; Candiotti, J.; Wang, H.; Cooper, R.A. Participatory design and validation of mobility enhancement robotic wheelchair. J. Rehabil. Res. Dev. 2015, 52, 739–750. [Google Scholar] [CrossRef]
- Wang, H.; Chung, C.; Candiotti, J.; Grindle, G.G.; Ding, D.; Cooper, R.A. User Participatory Design: Lessons Learned from PerMMA Development. In Proceedings of the Rehabilitation Engineering and Assistive Technology Society of North America, Seattle, WA, USA, 20–24 June 2013. [Google Scholar]
- Chiri, A.; Cempini, M.; De Rossi, S.M.M.; Lenzi, T.; Giovacchini, F.; Vitiello, N.; Carrozza, M.C. On the design of ergonomic wearable robotic devices for motion assistance and rehabilitation. In Proceedings of the 2012 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, San Diego, CA, USA, 28 August–1 September 2012; pp. 6124–6127. [Google Scholar]
- Francés-Morcillo, L.; Morer-Camo, P.; Rodríguez-Ferradas, M.I.; Cazón-Martín, A. Wearable design requirements identification and evaluation. Sensors 2020, 20, 2599. [Google Scholar] [CrossRef]
- Meng, Y.; Choi, H.-K.; Kim, H.-C. Exploring the user requirements for wearable healthcare systems. In Proceedings of the 2011 IEEE 13th International Conference on e-Health Networking, Applications and Services, Columbia, MO, USA, 13–15 June 2011; pp. 74–77. [Google Scholar]
- Motti, V.G.; Caine, K. Human factors considerations in the design of wearable devices. Proc. Hum. Factors Ergon. Soc. Annu. Meet. 2014, 58, 1820–1824. [Google Scholar]
- Oklahoma Tobacco Research Center Insight Platform. Available online: http://otrc.stephensoncancercenter.org/MobileHealth/InsightPlatform.aspx (accessed on 25 March 2022).
- Ghazi, M.; Rippetoe, J.; Chandrashekhar, R.; Wang, H. Focal vibration therapy: Vibration parameters of effective wearable devices. Appl. Sci. 2021, 11, 2969. [Google Scholar] [CrossRef]
- Axio Bionics Wearable Therapy Surface Electrical Stimulation System User Guide, Care & Instructions. Available online: https://www.axiobionics.com/wp-content/uploads/2019/05/WearableTherapyUserGuideV2.0.pdf (accessed on 15 March 2022).











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Requirements | Definition |
| Comfort (shape) | Acceptable temperature, texture, shape, and tightness [43,45]. |
| Comfort (ease of use) | Easy to set up and control for users with different needs [42,45]. |
| Comfort (usability) | Easy to put on and take off, considering full use of one arm and very little mobility on the affected arm [44,45]. |
| Comfort (obtrusiveness) | Enable and not hinder the natural body movements and functions [45]. |
| Comfort (sizing) | Customizable to fit different users’ sizes or sides (right or left) [42,43,44,45]. |
| Safety (harm) | Should not cause harm or pain [43,45]. |
| Safety (security) | Should attach securely with no risk of the device coming off. [44,45]. |
| Questions Asked to the Therapists | Responses (# of the Therapist) | ||||
|---|---|---|---|---|---|
| SD | D | N | A | SA | |
| Q1. Would like to use the app and web portal to monitor the usage of FoVi | 0 | 0 | 0 | 1 | 4 |
| Q2. The app and web portal are easy to use | 0 | 2 | 0 | 3 | 0 |
| Q3. May need a technical person while using the device long-term | 0 | 0 | 0 | 5 | 0 |
| Q4. Most people will use the device quickly | 0 | 1 | 0 | 0 | 4 |
| Source (# of Participants) | Comment/Suggestion |
|---|---|
| Therapist (5) | Concerned about the storage of data and reliability of web portal. |
| Therapist (5) | Integrate the web portal into the system used by the hospital. |
| Therapist (5) | Use some common selection of frequency and amplitude settings instead of individually adjusting each parameter. |
| Therapist (5) | Provide more evidence-based settings for users with different levels of severity and functional capacity. |
| Therapist (1) | User app could be challenge for less smartphone experience. |
| Stroke survivors (5) | Liked the feel of the vibration. |
| Stroke survivors (5) | The feature for adjusting vibration was very helpful. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, H.; Ghazi, M.; Chandrashekhar, R.; Rippetoe, J.; Duginski, G.A.; Lepak, L.V.; Milhan, L.R.; James, S.A. User Participatory Design of a Wearable Focal Vibration Device for Home-Based Stroke Rehabilitation. Sensors 2022, 22, 3308. https://doi.org/10.3390/s22093308
Wang H, Ghazi M, Chandrashekhar R, Rippetoe J, Duginski GA, Lepak LV, Milhan LR, James SA. User Participatory Design of a Wearable Focal Vibration Device for Home-Based Stroke Rehabilitation. Sensors. 2022; 22(9):3308. https://doi.org/10.3390/s22093308
Chicago/Turabian StyleWang, Hongwu, Mustafa Ghazi, Raghuveer Chandrashekhar, Josiah Rippetoe, Grace A. Duginski, Louis V. Lepak, Lisa R. Milhan, and Shirley A. James. 2022. "User Participatory Design of a Wearable Focal Vibration Device for Home-Based Stroke Rehabilitation" Sensors 22, no. 9: 3308. https://doi.org/10.3390/s22093308