Pre-Antiretroviral Therapy Serum Selenium Concentrations Predict WHO Stages 3, 4 or Death but not Virologic Failure Post-Antiretroviral Therapy

Abstract
:1. Introduction
2. Methods
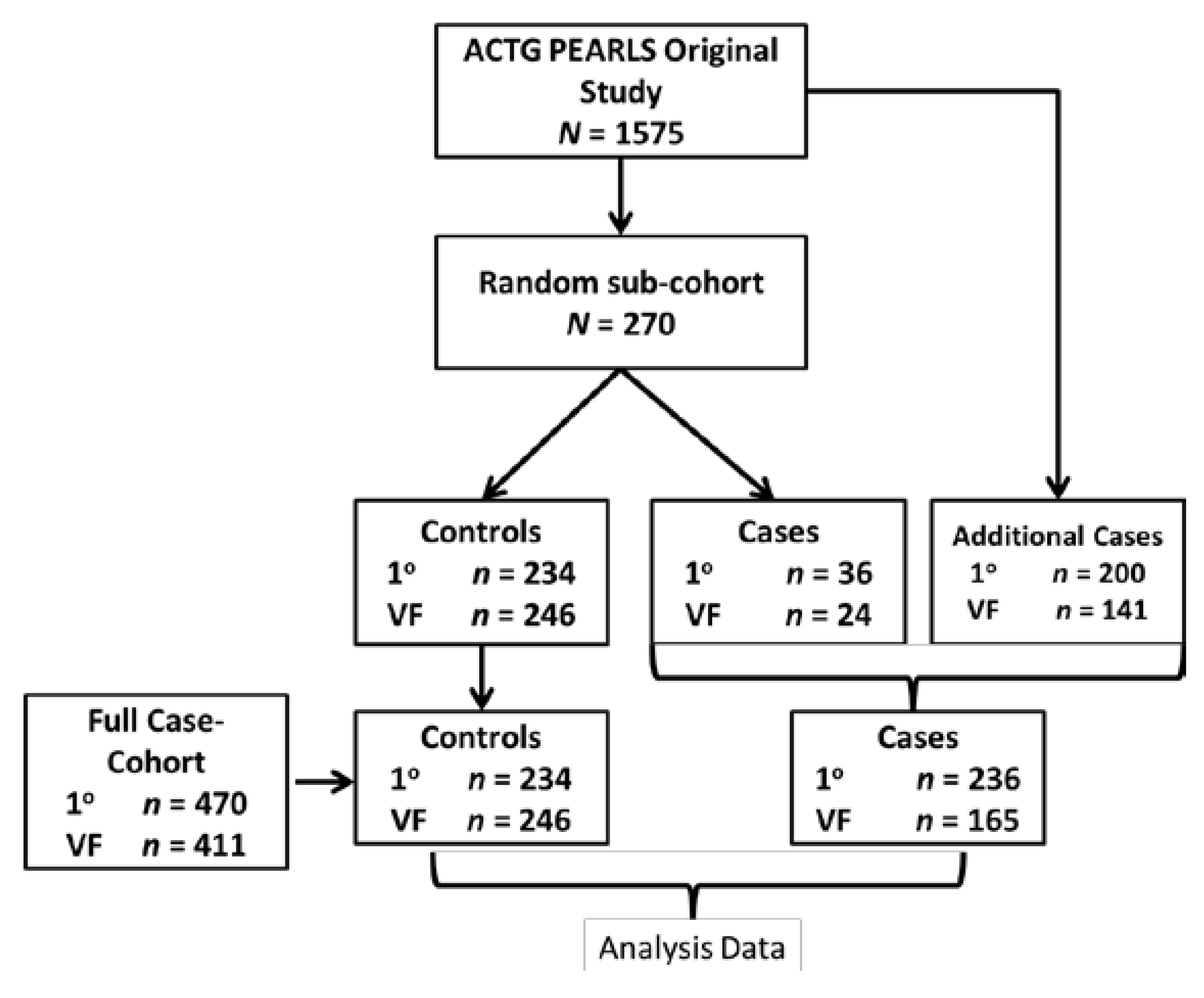
2.1. Study Population
2.2. Ethics Statement
2.3. Data Collection and Laboratory Analysis

2.4. Statistical Analysis
3. Results
3.1. Description of Study Population
3.2. Risk Factors for Baseline Serum Selenium Deficiency

{kind=link}
{kind=link}
| Characteristic | Selenium Levels | p-Value | |||
|---|---|---|---|---|---|
| All (n = 252) n (%) | All (n = 252) Median (IQR) | Deficient (n = 134) n (%) | Normal (n = 118) n (%) | ||
| Gender | |||||
| Male | 131 (52) | 88 (58–107) | 60 (46) | 71 (54) | 0.02 |
| Female | 121 (48) | 78 (57–95) | 74 (61) | 47 (39) | |
| Age, median (IQR) | 35 (30–41) | 35 (30–41) | 34.5 (29–41) | 0.26 | |
| Country | |||||
| Brazil | 30 (12) | 53 (46–61) | 26 (87) | 4 (13) | <0.001 |
| Haiti | 30 (12) | 109 (99–126) | 2 (7) | 28 (93) | |
| India | 18 (7) | 88 (67–106) | 8 (44) | 10 (56) | |
| Malawi | 30 (12) | 58 (49–73) | 28 (93) | 2 (7) | |
| Peru | 29 (12) | 92 (83–101) | 10 (34) | 19 (66) | |
| South Africa | 29 (12) | 73 (67–84) | 22 (76) | 7 (24) | |
| Thailand | 27 (11) | 93 (84–97) | 9 (33) | 18 (67) | |
| US | 30 (12) | 118 (108–128) | 0 (0) | 30 (100) | |
| Zimbabwe | 29 (12) | 50 (41–59) | 29 (100) | 0 (0) | |
| Race | |||||
| White | 15 (6) | 103 (46–125) | 7 (47) | 8 (53) | 0.007 |
| Black | 133 (53) | 73 (54–99) | 84 (63) | 49 (37) | |
| Hispanic | 57 (23) | 87 (67–101) | 26 (46) | 31 (54) | |
| Asian | 46 (18) | 91 (79–97) | 17 (37) | 29 (63) | |
| Body mass index (kg/m2) | |||||
| <18.5 | 19 (8) | 63 (45–97) | 13 (68) | 6 (32) | 0.16 |
| 18.5–25 | 166 (66) | 83 (57–99) | 91 (55) | 75 (45) | |
| ≥25 | 67 (27) | 88 (67–108) | 30 (45) | 37 (55) | |
| Treatment | |||||
| A | 94 (37) | 84 (57–96) | 48 (51) | 46 (49) | 0.61 |
| B | 83 (33) | 76 (58–100) | 48 (58) | 35 (42) | |
| C | 75 (30) | 85 (59–104) | 38 (51) | 37 (49) | |
| Prior TB diagnosis | 45 (18) | 84 (57–96) | 45 (18) | 35 (78) | <0.001 |
| CD4 count, median (IQR), cells/μL | 179 (88, 231) | 179 (88, 231) | 171 (71, 233) | 0.53 | |
| Viral load, median (IQR), log10 copies/mL | 5.1 (4.6, 5.5) | 5.1 (4.7, 5.5) | 5.0 (4.5, 5.5) | 0.26 | |
| Hemoglobin, median (IQR), g/dL | 12.4 (10.9, 13.8) | 12.1 (10.6, 13.7) | 12.8 (11.4, 14.1) | 0.008 | |
| Albumin, median (IQR), g/dL | 3.9 (3.6, 4.3) | 3.8 (3.3, 4.1) | 4.1 (3.9, 4.4) | <0.0001 | |
| Log CRP, median (IQR), mg/L | 3.4 (1.4, 10.3) | 5.0 (1.4, 16.2) | 2.4 (1.2, 7.1) | 0.006 | |

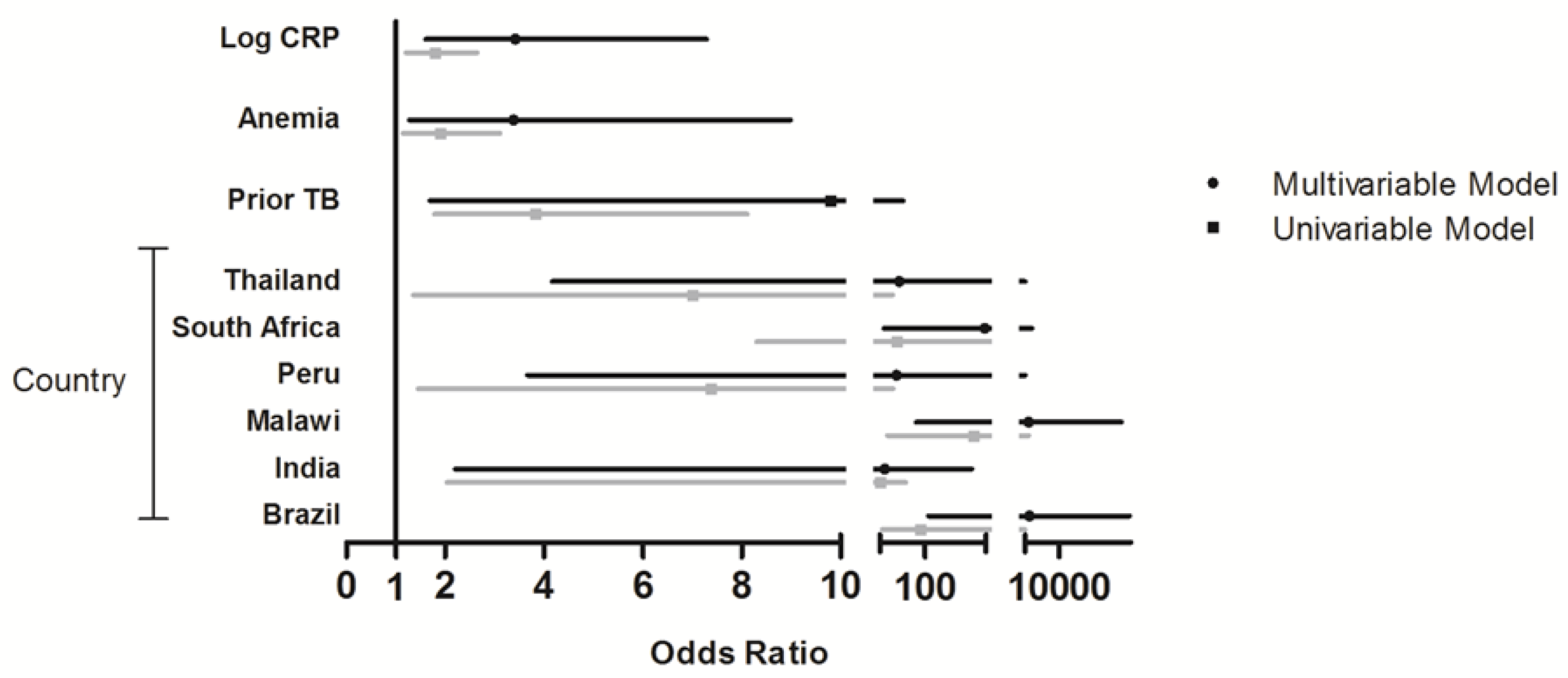
3.3. Association of Baseline Serum Selenium with Clinical Failure and Virologic Failure
| a | ||||
|---|---|---|---|---|
| n (%) | Univariable | Multivariable 1 (Adjusted for Gender, Age, BMI, CD4 Count, Viral Load, Hemoglobin and Albumin) | Multivariable 2 (Adjusted for Variables in Multivariable Model 1 + CRP) | |
| By selenium deficiency status | ||||
| Normal (≥85 μg/L) | 173 (42) | Reference | Reference | Reference |
| Selenium Deficient ( | 240 (58) | 1.85 (0.92–3.70) | 1.43 (0.68–3.02) | 1.14 (0.49–2.61) |
| By quartiles of selenium | ||||
| Quartile 1 ( | 98 (24) | 3.51 (1.06–11.60) | 2.71 (0.70–10.45) | 2.25 (0.57–8.79) |
| Quartile 2 (55.60–75.52 μg/L) | 94 (23) | 2.57 (1.04–6.35) | 1.74 (0.60–5.03) | 1.46 (0.49–4.35) |
| Quartile 3 (75.52–97.45 μg/L) | 111 (27) | Reference | Reference | Reference |
| Quartile 4 (>97.45 μg/L) | 110 (26) | 2.16 (0.88–5.30) | 3.50 (1.30–9.42) | 4.13 (1.65–10.35) |
| b | ||||
| n (%) | Univariable | Multivariable 3 (Adjusted for Gender, Age, BMI, CD4 Count, Viral Load, Treatment Arm) | Multivariable 4 (Adjusted for Variables in Multivariable Model 3 + CRP) | |
| By selenium deficiency status | ||||
| Normal (≥85 μg/L) | 221 (58) | Reference | Reference | Reference |
| Selenium Deficient (<85 µg/L) | 160 (42) | 0.88 (0.43–1.8) | 0.68 (0.31–1.48) | 0.64 (0.28–1.46) |
| By quartiles of selenium | ||||
| Quartile 1 (<55.73 µg/L) | 89 (23) | 1.37 (0.47–3.98) | 1.32 (0.45–3.91) | 1.29 (0.44–3.79) |
| Quartile 2 (55.73–74.86 μg/L) | 85 (23) | 1.11 (0.50–2.51) | 0.97 (0.43–2.22) | 0.91 (0.39–2.13) |
| Quartile 3 (74.86–95.10 μg/L) | 99 (26) | Reference | Reference | Reference |
| Quartile 4 (>95.10 μg/L) | 108 (28) | 0.84 (0.31–2.33) | 0.92 (0.34–2.50) | 0.87 (0.30–2.49) |
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- The Joint United Nations Programme on HIV/AIDS (UNAIDS). Global Report: Unaids Report on the Global Aids Epidemic; Joint United Nations Programme on HIV/AIDS: Geneva, Switzerland, 2013. [Google Scholar]
- Moh, R.; Danel, C.; Messou, E.; Ouassa, T.; Gabillard, D.; Anzian, A.; Abo, Y.; Salamon, R.; Bissagnene, E.; Seyler, C.; et al. Incidence and determinants of mortality and morbidity following early antiretroviral therapy initiation in HIV-infected adults in West Africa. AIDS 2007, 21, 2483–2491. [Google Scholar] [CrossRef] [PubMed]
- Moore, D.; Liechty, C.; Ekwaru, P.; Were, W.; Mwima, G.; Solberg, P.; Rutherford, G.; Mermin, J. Prevalence, incidence and mortality associated with tuberculosis in HIV-infected patients initiating antiretroviral therapy in rural Uganda. AIDS 2007, 21, 713–719. [Google Scholar] [CrossRef] [PubMed]
- Paton, N.I.; Sangeetha, S.; Earnest, A.; Bellamy, R. The impact of malnutrition on survival and the CD4 count response in HIV-infected patients starting antiretroviral therapy. HIV Med. 2006, 7, 323–330. [Google Scholar] [CrossRef] [PubMed]
- Irlam, J.H.; Visser, M.M.; Rollins, N.N.; Siegfried, N. Micronutrient supplementation in children and adults with HIV infection. Cochrane Database Syst. Rev. 2010, 10. [Google Scholar] [CrossRef]
- Stone, C.A.; Kawai, K.; Kupka, R.; Fawzi, W.W. Role of selenium in HIV infection. Nutr. Rev. 2010, 68, 671–681. [Google Scholar] [CrossRef] [PubMed]
- Kupka, R.; Mugusi, F.; Aboud, S.; Msamanga, G.I.; Finkelstein, J.L.; Spiegelman, D.; Fawzi, W.W. Randomized, double-blind, placebo-controlled trial of selenium supplements among HIV-infected pregnant women in Tanzania: Effects on maternal and child outcomes. Am. J. Clin. Nutr. 2008, 87, 1802–1808. [Google Scholar] [PubMed]
- Hurwitz, B.E.; Klaus, J.R.; Llabre, M.M.; Gonzalez, A.; Lawrence, P.J.; Maher, K.J.; Greeson, J.M.; Baum, M.K.; Shor-Posner, G.; Skyler, J.S.; et al. Suppression of human immunodeficiency virus type 1 viral load with selenium supplementation: A randomized controlled trial. Arch. Intern. Med. 2007, 167, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Burbano, X.; Miguez-Burbano, M.J.; McCollister, K.; Zhang, G.; Rodriguez, A.; Ruiz, P.; Lecusay, R.; Shor-Posner, G. Impact of a selenium chemoprevention clinical trial on hospital admissions of HIV-infected participants. HIV Clin. Trials 2002, 3, 483–491. [Google Scholar] [CrossRef] [PubMed]
- Baum, M.K.; Campa, A.; Lai, S.; Martinez, S.S.; Tsalaile, L.; Burns, P.; Farahani, M.; Li, Y.; van Widenfelt, E.; Page, J.B.; et al. Effect of micronutrient supplementation on disease progression in asymptomatic, antiretroviral-naive, HIV-infected adults in Botswana: A randomized clinical trial. JAMA 2013, 310, 2154–2163. [Google Scholar] [CrossRef] [PubMed]
- Rayman, M.P. Selenium and human health. Lancet 2012, 379, 1256–1268. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, R.L.; Simonovic, M. Synthesis and decoding of selenocysteine and human health. Croat. Med. J. 2012, 53, 535–550. [Google Scholar] [CrossRef] [PubMed]
- Reeves, M.A.; Hoffmann, P.R. The human selenoproteome: Recent insights into functions and regulation. Cell. Mol. Life Sci. CMLS 2009, 66, 2457–2478. [Google Scholar] [CrossRef]
- Blas-Garcia, A.; Apostolova, N.; Esplugues, J.V. Oxidative stress and mitochondrial impairment after treatment with anti-HIV drugs: Clinical implications. Curr. Pharm. Des. 2011, 17, 4076–4086. [Google Scholar] [CrossRef] [PubMed]
- Sappey, C.; Legrand-Poels, S.; Best-Belpomme, M.; Favier, A.; Rentier, B.; Piette, J. Stimulation of glutathione peroxidase activity decreases HIV type 1 activation after oxidative stress. AIDS Res. Hum. Retrovir. 1994, 10, 1451–1461. [Google Scholar] [CrossRef] [PubMed]
- Kalantari, P.; Narayan, V.; Natarajan, S.K.; Muralidhar, K.; Gandhi, U.H.; Vunta, H.; Henderson, A.J.; Prabhu, K.S. Thioredoxin reductase-1 negatively regulates HIV-1 transactivating protein tat-dependent transcription in human macrophages. J. Biol. Chem. 2008, 283, 33183–33190. [Google Scholar] [CrossRef] [PubMed]
- Rayman, M.P. Food-chain selenium and human health: Emphasis on intake. Br. J. Nutr. 2008, 100, 254–268. [Google Scholar] [PubMed]
- Duntas, L.H. Selenium and inflammation: Underlying anti-inflammatory mechanisms. Horm. Metab. Res. 2009, 41, 443–447. [Google Scholar] [CrossRef] [PubMed]
- Drain, P.K.; Baeten, J.M.; Overbaugh, J.; Wener, M.H.; Bankson, D.D.; Lavreys, L.; Mandaliya, K.; Ndinya-Achola, J.O.; McClelland, R.S. Low serum albumin and the acute phase response predict low serum selenium in HIV-1 infected women. BMC Infect. Dis. 2006, 6. [Google Scholar] [CrossRef]
- Campbell, T.B.; Smeaton, L.M.; Kumarasamy, N.; Flanigan, T.; Klingman, K.L.; Firnhaber, C.; Grinsztejn, B.; Hosseinipour, M.C.; Kumwenda, J.; Lalloo, U.; et al. Efficacy and safety of three antiretroviral regimens for initial treatment of HIV-1: A randomized clinical trial in diverse multinational settings. PLoS Med. 2012, 9. [Google Scholar] [CrossRef]
- Barlow, W.E.; Ichikawa, L.; Rosner, D.; Izumi, S. Analysis of case-cohort designs. J. Clin. Epidemiol. 1999, 52, 1165–1172. [Google Scholar] [CrossRef] [PubMed]
- Onland-Moret, N.C.; van der A, D.L.; van der Schouw, Y.T.; Buschers, W.; Elias, S.G.; van Gils, C.H.; Koerselman, J.; Roest, M.; Grobbee, D.E.; Peeters, P.H. Analysis of case-cohort data: A comparison of different methods. J. Clin. Epidemiol. 2007, 60, 350–355. [Google Scholar] [CrossRef] [PubMed]
- Campa, A.; Shor-Posner, G.; Indacochea, F.; Zhang, G.; Lai, H.; Asthana, D.; Scott, G.B.; Baum, M.K. Mortality risk in selenium-deficient HIV-positive children. J. Acquir. Immune Defic. Syndr. Hum. Retrovirol. 1999, 20, 508–513. [Google Scholar] [CrossRef] [PubMed]
- Baum, M.K.; Shor-Posner, G.; Lai, S.; Zhang, G.; Lai, H.; Fletcher, M.A.; Sauberlich, H.; Page, J.B. High risk of HIV-related mortality is associated with selenium deficiency. J. Acquir. Immune Defic. Syndr. Hum. Retrovirol. 1997, 15, 370–374. [Google Scholar] [CrossRef] [PubMed]
- Baeten, J.M.; Mostad, S.B.; Hughes, M.P.; Overbaugh, J.; Bankson, D.D.; Mandaliya, K.; Ndinya-Achola, J.O.; Bwayo, J.J.; Kreiss, J.K. Selenium deficiency is associated with shedding of HIV-1—Infected cells in the female genital tract. J. Acquir. Immune Defic. Syndr. 2001, 26, 360–364. [Google Scholar] [CrossRef] [PubMed]
- Maehira, F.; Luyo, G.A.; Miyagi, I.; Oshiro, M.; Yamane, N.; Kuba, M.; Nakazato, Y. Alterations of serum selenium concentrations in the acute phase of pathological conditions. Clin. Chim. Acta 2002, 316, 137–146. [Google Scholar] [CrossRef] [PubMed]
- Fairweather-Tait, S.J.; Bao, Y.; Broadley, M.R.; Collings, R.; Ford, D.; Hesketh, J.E.; Hurst, R. Selenium in human health and disease. Antioxid. Redox Signal. 2011, 14, 1337–1383. [Google Scholar] [CrossRef] [PubMed]
- Semba, R.D.; Ricks, M.O.; Ferrucci, L.; Xue, Q.L.; Guralnik, J.M.; Fried, L.P. Low serum selenium is associated with anemia among older adults in the United States. Eur. J. Clin. Nutr. 2009, 63, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Nichol, C.; Herdman, J.; Sattar, N.; O’Dwyer, P.J.; O’Reilly, D.S.J.; Littlejohn, D.; Fell, G. Changes in the concentrations of plasma selenium and selenoproteins after minor elective surgery: Further evidence for a negative acute phase response? Clin. Chem. 1998, 44, 1764–1766. [Google Scholar]
- Ford, E.S.; Liu, S.; Mannino, D.M.; Giles, W.H.; Smith, S.J. C-reactive protein concentration and concentrations of blood vitamins, carotenoids, and selenium among United States adults. Eur. J. Clin. Nutr. 2003, 57, 1157–1163. [Google Scholar] [CrossRef] [PubMed]
- Drain, P.K.; Kupka, R.; Msamanga, G.I.; Urassa, W.; Mugusi, F.; Fawzi, W.W. C-reactive protein independently predicts HIV-related outcomes among women and children in a resource-poor setting. AIDS 2007, 21, 2067–2075. [Google Scholar] [CrossRef] [PubMed]
- Van Lettow, M.; West, C.E.; van der Meer, J.W.; Wieringa, F.T.; Semba, R.D. Low plasma selenium concentrations, high plasma human immunodeficiency virus load and high interleukin-6 concentrations are risk factors associated with anemia in adults presenting with pulmonary tuberculosis in Zomba district, Malawi. Eur. J. Clin. Nutr. 2005, 59, 526–532. [Google Scholar] [CrossRef] [PubMed]
- Sheehan, H.B.; Benetucci, J.; Muzzio, E.; Redini, L.; Naveira, J.; Segura, M.; Weissenbacher, M.; Tang, A.M. High rates of serum selenium deficiency among HIV- and HCV-infected and uninfected drug users in Buenos Aires, Argentina. Public Health Nutr. 2012, 15, 538–545. [Google Scholar] [CrossRef] [PubMed]
- Look, M.P.; Rockstroh, J.K.; Rao, G.S.; Kreuzer, K.A.; Barton, S.; Lemoch, H.; Sudhop, T.; Hoch, J.; Stockinger, K.; Spengler, U.; et al. Serum selenium, plasma glutathione (GSH) and erythrocyte glutathione peroxidase (GSH-Px)-levels in asymptomatic versus symptomatic human immunodeficiency virus-1 (HIV-1)-infection. Eur. J. Clin. Nutr. 1997, 51, 266–272. [Google Scholar] [CrossRef] [PubMed]
- Kupka, R.; Msamanga, G.I.; Spiegelman, D.; Rifai, N.; Hunter, D.J.; Fawzi, W.W. Selenium levels in relation to morbidity and mortality among children born to HIV-infected mothers. Eur. J. Clin. Nutr. 2005, 59, 1250–1258. [Google Scholar] [CrossRef] [PubMed]
- Kupka, R.; Msamanga, G.I.; Spiegelman, D.; Morris, S.; Mugusi, F.; Hunter, D.J.; Fawzi, W.W. Selenium status is associated with accelerated HIV disease progression among HIV-1-infected pregnant women in Tanzania. J. Nutr. 2004, 134, 2556–2560. [Google Scholar] [PubMed]
- Kupka, R.; Garland, M.; Msamanga, G.; Spiegelman, D.; Hunter, D.; Fawzi, W. Selenium status, pregnancy outcomes, and mother-to-child transmission of HIV-1. J. Acquir. Immune Defic. Syndr. 2005, 39, 203–210. [Google Scholar] [PubMed]
- Shor-Posner, G.; Miguez, M.J.; Pineda, L.M.; Rodriguez, A.; Ruiz, P.; Castillo, G.; Burbano, X.; Lecusay, R.; Baum, M. Impact of selenium status on the pathogenesis of mycobacterial disease in HIV-1-infected drug users during the era of highly active antiretroviral therapy. J. Acquir. Immune Defic. Syndr. 2002, 29, 169–173. [Google Scholar] [CrossRef] [PubMed]
- Constans, J.; Pellegrin, J.L.; Sergeant, C.; Simonoff, M.; Pellegrin, I.; Fleury, H.; Leng, B.; Conri, C. Serum selenium predicts outcome in HIV infection. J. Acquir. Immune Defic. Syndr. Hum. Retrovirol. 1995, 10, 392. [Google Scholar] [CrossRef] [PubMed]
- Stephensen, C.B.; Marquis, G.S.; Douglas, S.D.; Wilson, C.M. Immune activation and oxidative damage in HIV-positive and HIV-negative adolescents. J. Acquir. Immune Defic. Syndr. 2005, 38, 180–190. [Google Scholar] [CrossRef] [PubMed]
- Stephensen, C.B.; Marquis, G.S.; Douglas, S.D.; Kruzich, L.A.; Wilson, C.M. Glutathione, glutathione peroxidase, and selenium status in HIV-positive and HIV-negative adolescents and young adults. Am. J. Clin. Nutr. 2007, 85, 173–181. [Google Scholar] [PubMed]
- Stambullian, M.; Feliu, S.; Slobodianik, N.H. Nutritional status in patients with HIV infection and aids. Br. J. Nutr. 2007, 98, 140–143. [Google Scholar] [CrossRef] [PubMed]
- Rousseau, M.C.; Molines, C.; Moreau, J.; Delmont, J. Influence of highly active antiretroviral therapy on micronutrient profiles in HIV-infected patients. Ann. Nutr. Metab. 2000, 44, 212–216. [Google Scholar] [CrossRef] [PubMed]
- Look, M.P.; Rockstroh, J.K.; Rao, G.S.; Kreuzer, K.A.; Spengler, U.; Sauerbruch, T. Serum selenium vs lymphocyte subsets and markers of disease progression and inflammatory response in human immunodeficiency virus-1 infection. Biol. Trace Elem. Res. 1997, 56, 31–41. [Google Scholar] [CrossRef] [PubMed]
- Jones, C.Y.; Tang, A.M.; Forrester, J.E.; Huang, J.; Hendricks, K.M.; Knox, T.A.; Spiegelman, D.; Semba, R.D.; Woods, M.N. Micronutrient levels and HIV disease status in HIV-infected patients on highly active antiretroviral therapy in the nutrition for healthy living cohort. J. Acquir. Immune Defic. Syndr. 2006, 43, 475–482. [Google Scholar] [CrossRef] [PubMed]
- Baum, M.K.; Shor-Posner, G.; Zhang, G.; Lai, H.; Quesada, J.A.; Campa, A.; Jose-Burbano, M.; Fletcher, M.A.; Sauberlich, H.; Page, J.B. HIV-1 infection in women is associated with severe nutritional deficiencies. J. Acquir. Immune Defic. Syndr. Hum. Retrovirol. 1997, 16, 272–278. [Google Scholar] [CrossRef] [PubMed]
- Shenkin, A. Micronutrients in health and disease. Postgrad. Med. J. 2006, 82, 559–567. [Google Scholar] [CrossRef] [PubMed]
- Nathan, C.; Cunningham-Bussel, A. Beyond oxidative stress: An immunologist’s guide to reactive oxygen species. Nat. Rev. Immunol. 2013, 13, 349–361. [Google Scholar] [CrossRef] [PubMed]
- Kohen, R.; Nyska, A. Oxidation of biological systems: Oxidative stress phenomena, antioxidants, redox reactions, and methods for their quantification. Toxicol. Pathol. 2002, 30, 620–650. [Google Scholar] [CrossRef] [PubMed]
- Duffield, A.J.; Thomson, C.D.; Hill, K.E.; Williams, S. An estimation of selenium requirements for new zealanders. Am. J. Clin. Nutr. 1999, 70, 896–903. [Google Scholar] [PubMed]
- Thomson, C.D.; Robinson, M.F.; Butler, J.A.; Whanger, P.D. Long-term supplementation with selenate and selenomethionine: Selenium and glutathione peroxidase (ec 1.11.1.9) in blood components of New Zealand women. Br. J. Nutr. 1993, 69, 577–588. [Google Scholar] [CrossRef] [PubMed]
- Bunupuradah, T.; Ubolyam, S.; Hansudewechakul, R.; Kosalaraksa, P.; Ngampiyaskul, C.; Kanjanavanit, S.; Wongsawat, J.; Luesomboon, W.; Pinyakorn, S.; Kerr, S.; et al. Correlation of selenium and zinc levels to antiretroviral treatment outcomes in Thai HIV-infected children without severe HIV symptoms. Eur. J. Clin. Nutr. 2012, 66, 900–905. [Google Scholar] [CrossRef] [PubMed]
- Dillon, D.M.; Stapleton, J.T. Selenium effects on HIV rna and CD4 cell counts. Arch. Intern. Med. 2007, 167, 1556–1557. [Google Scholar] [CrossRef] [PubMed]
- Ross, D.A.; Cousens, S.; Wedner, S.H.; Sismanidis, C. Does selenium supplementation slow progression of HIV? Potentially misleading presentation of the results of a trial. Arch. Intern. Med. 2007, 167, 1555–1556. [Google Scholar] [PubMed]
- Passaretti, C.; Gupta, A. Selenium and HIV-1: Hope or hype? Arch. Intern. Med. 2007, 167, 2530–2531. [Google Scholar]
- Safren, S.A.; Biello, K.B.; Smeaton, L.; Mimiaga, M.J.; Walawander, A.; Lama, J.R.; Rana, A.; Nyirenda, M.; Kayoyo, V.M.; Samaneka, W.; et al. Psychosocial predictors of non-adherence and treatment failure in a large scale multi-national trial of antiretroviral therapy for HIV: Data from the actg a5175/pearls trial. PLoS One 2014, 9. [Google Scholar] [CrossRef] [PubMed]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shivakoti, R.; Gupte, N.; Yang, W.-T.; Mwelase, N.; Kanyama, C.; Tang, A.M.; Pillay, S.; Samaneka, W.; Riviere, C.; Berendes, S.; et al. Pre-Antiretroviral Therapy Serum Selenium Concentrations Predict WHO Stages 3, 4 or Death but not Virologic Failure Post-Antiretroviral Therapy. Nutrients 2014, 6, 5061-5078. https://doi.org/10.3390/nu6115061
Shivakoti R, Gupte N, Yang W-T, Mwelase N, Kanyama C, Tang AM, Pillay S, Samaneka W, Riviere C, Berendes S, et al. Pre-Antiretroviral Therapy Serum Selenium Concentrations Predict WHO Stages 3, 4 or Death but not Virologic Failure Post-Antiretroviral Therapy. Nutrients. 2014; 6(11):5061-5078. https://doi.org/10.3390/nu6115061
Chicago/Turabian StyleShivakoti, Rupak, Nikhil Gupte, Wei-Teng Yang, Noluthando Mwelase, Cecilia Kanyama, Alice M. Tang, Sandy Pillay, Wadzanai Samaneka, Cynthia Riviere, Sima Berendes, and et al. 2014. "Pre-Antiretroviral Therapy Serum Selenium Concentrations Predict WHO Stages 3, 4 or Death but not Virologic Failure Post-Antiretroviral Therapy" Nutrients 6, no. 11: 5061-5078. https://doi.org/10.3390/nu6115061