The Effect of Low-Carbohydrate Diet on Macrovascular and Microvascular Endothelial Function Is Not Affected by the Provision of Caloric Restriction in Women with Obesity: A Randomized Study

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
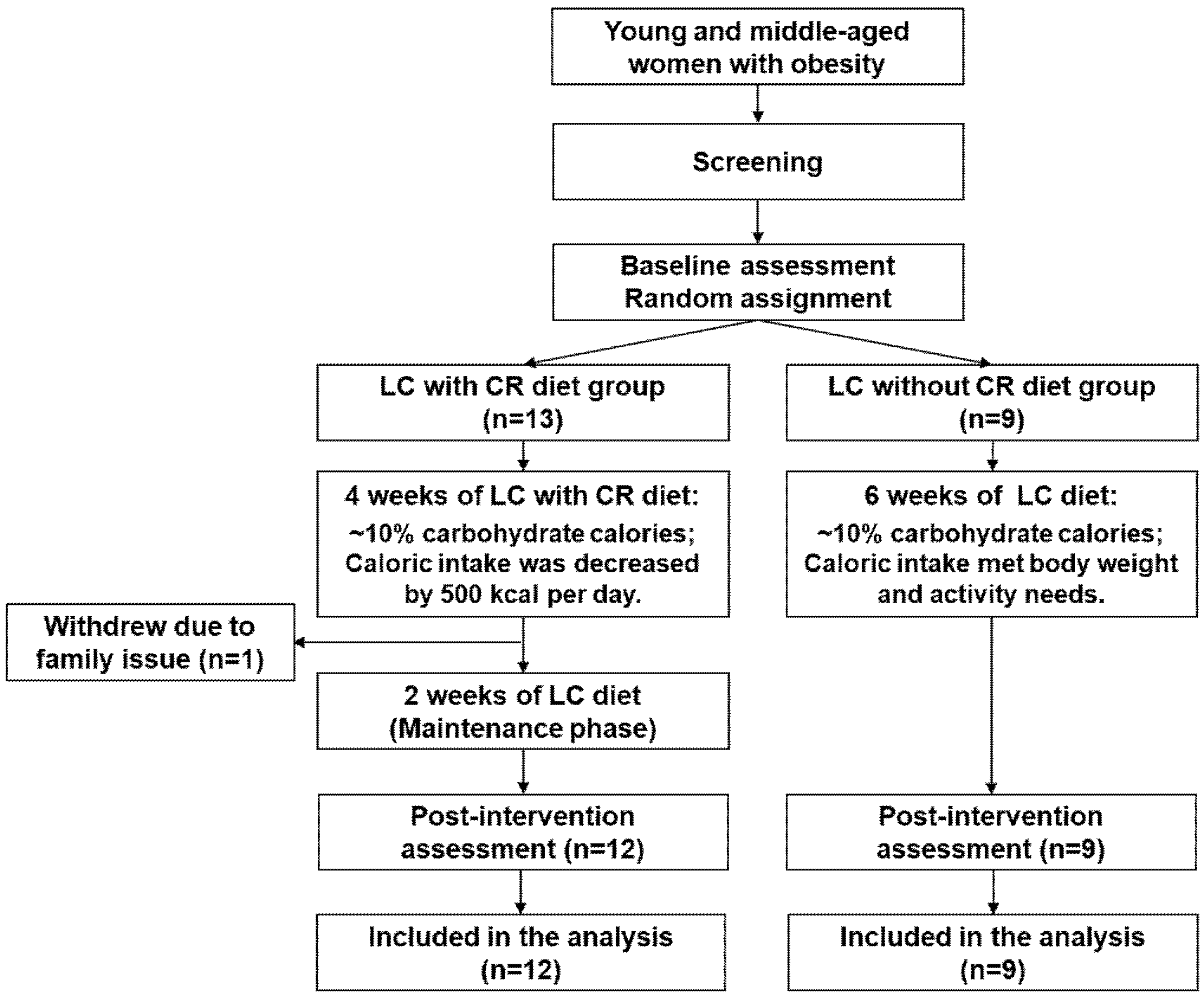
2.1. Study Design
2.2. Study Participants
2.3. Low-Carbohydrate Diet Intervention
2.4. Randomization
2.5. Study Procedures
2.5.1. Macrovascular Endothelial Function
2.5.2. Microvascular Endothelial Function
2.5.3. Cardiovascular Risks
2.6. Statistical Analysis
3. Results
3.1. Dietary Intake and Physical Activity
3.2. Participant Characteristics and Baseline Values
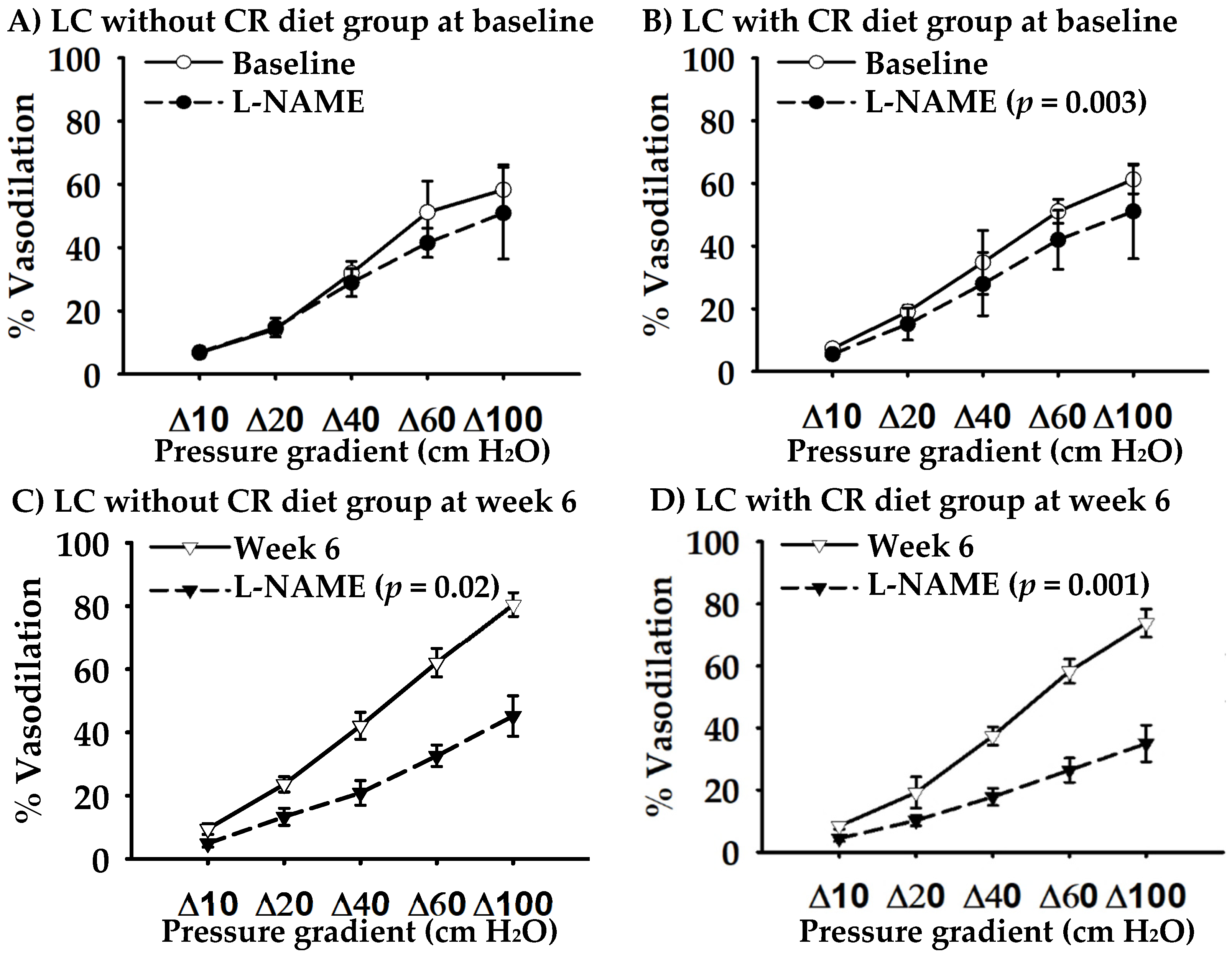
3.3. Effect of LC Diet on Macro- and Micro-Vascular Endothelial Function
3.4. Effect of LC Diet on Cardiovascular Risks
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- With Special Feature on Mortality; Health, United States: Hyattsville, MD, USA, 2017.
- Heymsfield, S.B.; Wadden, T.A. Mechanisms, Pathophysiology, and Management of Obesity. N. Engl. J. Med. 2017, 376, 254–266. [Google Scholar] [CrossRef]
- Fan, J.; Song, Y.; Chen, Y.; Hui, R.; Zhang, W. Combined effect of obesity and cardio-metabolic abnormality on the risk of cardiovascular disease: A meta-analysis of prospective cohort studies. Int J. Cardiol. 2013, 168, 4761–4768. [Google Scholar] [CrossRef]
- Benjamin, E.J.; Muntner, P.; Alonso, A.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Das, S.R.; et al. Heart Disease and Stroke Statistics-2019 Update: A Report From the American Heart Association. Circulation 2019, 139, e56–e528. [Google Scholar] [CrossRef]
- Bonetti, P.O.; Lerman, L.O.; Lerman, A. Endothelial dysfunction: A marker of atherosclerotic risk. Arterioscler Thromb. Vasc. Biol. 2003, 23, 168–175. [Google Scholar] [CrossRef]
- Vanhoutte, P.M.; Zhao, Y.; Xu, A.; Leung, S.W. Thirty Years of Saying NO: Sources, Fate, Actions, and Misfortunes of the Endothelium-Derived Vasodilator Mediator. Circ. Res. 2016, 119, 375–396. [Google Scholar] [CrossRef] [Green Version]
- Ne, J.Y.A.; Cai, T.Y.; Celermajer, D.S.; Caterson, I.D.; Gill, T.; Lee, C.M.Y.; Skilton, M.R. Obesity, arterial function and arterial structure - a systematic review and meta-analysis. Obes. Sci. Pract. 2017, 3, 171–184. [Google Scholar] [CrossRef]
- Virdis, A.; Masi, S.; Colucci, R.; Chiriaco, M.; Uliana, M.; Puxeddu, I.; Bernardini, N.; Blandizzi, C.; Taddei, S. Microvascular Endothelial Dysfunction in Patients with Obesity. Curr. Hypertens. Rep. 2019, 21, 32. [Google Scholar] [CrossRef]
- Keogh, J.B.; Brinkworth, G.D.; Clifton, P.M. Effects of weight loss on a low-carbohydrate diet on flow-mediated dilatation, adhesion molecules and adiponectin. Br. J. Nutr. 2007, 98, 852–859. [Google Scholar] [CrossRef] [Green Version]
- Keogh, J.B.; Brinkworth, G.D.; Noakes, M.; Belobrajdic, D.P.; Buckley, J.D.; Clifton, P.M. Effects of weight loss from a very-low-carbohydrate diet on endothelial function and markers of cardiovascular disease risk in subjects with abdominal obesity. Am. J. Clin. Nutr. 2008, 87, 567–576. [Google Scholar] [CrossRef] [Green Version]
- Wycherley, T.P.; Brinkworth, G.D.; Keogh, J.B.; Noakes, M.; Buckley, J.D.; Clifton, P.M. Long-term effects of weight loss with a very low carbohydrate and low fat diet on vascular function in overweight and obese patients. J. Intern. Med. 2010, 267, 452–461. [Google Scholar] [CrossRef]
- Wycherley, T.P.; Thompson, C.H.; Buckley, J.D.; Luscombe-Marsh, N.D.; Noakes, M.; Wittert, G.A.; Brinkworth, G.D. Long-term effects of weight loss with a very-low carbohydrate, low saturated fat diet on flow mediated dilatation in patients with type 2 diabetes: A randomised controlled trial. Atherosclerosis 2016, 252, 28–31. [Google Scholar] [CrossRef] [Green Version]
- Buscemi, S.; Verga, S.; Tranchina, M.R.; Cottone, S.; Cerasola, G. Effects of hypocaloric very-low-carbohydrate diet vs. Mediterranean diet on endothelial function in obese women*. Eur. J. Clin. Invest. 2009, 39, 339–347. [Google Scholar] [CrossRef]
- Ballard, K.D.; Quann, E.E.; Kupchak, B.R.; Volk, B.M.; Kawiecki, D.M.; Fernandez, M.L.; Seip, R.L.; Maresh, C.M.; Kraemer, W.J.; Volek, J.S. Dietary carbohydrate restriction improves insulin sensitivity, blood pressure, microvascular function, and cellular adhesion markers in individuals taking statins. Nutr. Res. 2013, 33, 905–912. [Google Scholar] [CrossRef]
- Phillips, S.A.; Jurva, J.W.; Syed, A.Q.; Syed, A.Q.; Kulinski, J.P.; Pleuss, J.; Hoffmann, R.G.; Gutterman, D.D. Benefit of low-fat over low-carbohydrate diet on endothelial health in obesity. Hypertension 2008, 51, 376–382. [Google Scholar] [CrossRef] [Green Version]
- Varady, K.A.; Bhutani, S.; Klempel, M.C.; Phillips, S.A. Improvements in vascular health by a low-fat diet, but not a high-fat diet, are mediated by changes in adipocyte biology. Nutr. J. 2011, 10, 8. [Google Scholar] [CrossRef] [Green Version]
- Volek, J.S.; Ballard, K.D.; Silvestre, R.; Judelson, D.A.; Quann, E.E.; Forsythe, C.E.; Fernandez, M.L.; Kraemer, W.J. Effects of dietary carbohydrate restriction versus low-fat diet on flow-mediated dilation. Metabolism 2009, 58, 1769–1777. [Google Scholar] [CrossRef]
- Raitakari, M.; Ilvonen, T.; Ahotupa, M.; Lehtimaki, T.; Harmoinen, A.; Suominen, P.; Elo, J.; Hartiala, J.; Raitakari, O.T. Weight reduction with very-low-caloric diet and endothelial function in overweight adults: Role of plasma glucose. Arterioscler Thromb. Vasc. Biol. 2004, 24, 124–128. [Google Scholar] [CrossRef] [Green Version]
- Pierce, G.L.; Beske, S.D.; Lawson, B.R.; Southall, K.L.; Benay, F.J.; Donato, A.J.; Seals, D.R. Weight loss alone improves conduit and resistance artery endothelial function in young and older overweight/obese adults. Hypertension 2008, 52, 72–79. [Google Scholar] [CrossRef] [Green Version]
- Sasaki, S.; Higashi, Y.; Nakagawa, K.; Kimura, M.; Noma, K.; Sasaki, S.; Hara, K.; Matsuura, H.; Goto, C.; Oshima, T.; et al. A low-calorie diet improves endothelium-dependent vasodilation in obese patients with essential hypertension. Am. J. Hypertens. 2002, 15, 302–309. [Google Scholar] [CrossRef]
- Dengel, D.R.; Kelly, A.S.; Olson, T.P.; Kaiser, D.R.; Dengel, J.L.; Bank, A.J. Effects of weight loss on insulin sensitivity and arterial stiffness in overweight adults. Metabolism 2006, 55, 907–911. [Google Scholar] [CrossRef]
- Brook, R.D.; Bard, R.L.; Glazewski, L.; Kehrer, C.; Bodary, P.F.; Eitzman, D.L.; Rajagopalan, S. Effect of short-term weight loss on the metabolic syndrome and conduit vascular endothelial function in overweight adults. Am. J. Cardiol. 2004, 93, 1012–1016. [Google Scholar] [CrossRef] [PubMed]
- Wycherley, T.P.; Brinkworth, G.D.; Noakes, M.; Buckley, J.D.; Clifton, P.M. Effect of caloric restriction with and without exercise training on oxidative stress and endothelial function in obese subjects with type 2 diabetes. Diabetes. Obes. Metab. 2008, 10, 1062–1073. [Google Scholar] [CrossRef] [PubMed]
- Focardi, M.; Dick, G.M.; Picchi, A.; Zhang, C.; Chilian, W.M. Restoration of coronary endothelial function in obese Zucker rats by a low-carbohydrate diet. Am. J. Physiol. Heart. Circ. Physiol. 2007, 292, H2093–H2099. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mifflin, M.D.; St Jeor, S.T.; Hill, L.A.; Scott, B.J.; Daugherty, S.A.; Koh, Y.O. A new predictive equation for resting energy expenditure in healthy individuals. Am. J. Clin. Nutr. 1990, 51, 241–247. [Google Scholar] [CrossRef]
- Hoddy, K.K.; Bhutani, S.; Phillips, S.A.; Varady, K.A. Effects of different degrees of insulin resistance on endothelial function in obese adults undergoing alternate day fasting. Nutr. Healthy Aging 2016, 4, 63–71. [Google Scholar] [CrossRef] [Green Version]
- Goslawski, M.; Piano, M.R.; Bian, J.T.; Church, E.C.; Szczurek, M.; Phillips, S.A. Binge drinking impairs vascular function in young adults. J. Am. Coll. Cardiol. 2013, 62, 201–207. [Google Scholar] [CrossRef] [Green Version]
- Thijssen, D.H.; Black, M.A.; Pyke, K.E.; Padilla, J.; Atkinson, G.; Harris, R.A.; Parker, B.; Widlansky, M.E.; Tschakovsky, M.E.; Green, D.J. Assessment of flow-mediated dilation in humans: A methodological and physiological guideline. Am. J. Physiol. Heart. Circ. Physiol. 2011, 300, H2–H12. [Google Scholar] [CrossRef] [Green Version]
- Hwang, C.L.; Bian, J.T.; Thur, L.A.; Peters, T.A.; Piano, M.R.; Phillips, S.A. Tetrahydrobiopterin Restores Microvascular Dysfunction in Young Adult Binge Drinkers. Alcohol. Clin. Exp. Res. 2020, 44, 407–414. [Google Scholar] [CrossRef]
- Inaba, Y.; Chen, J.A.; Bergmann, S.R. Prediction of future cardiovascular outcomes by flow-mediated vasodilatation of brachial artery: A meta-analysis. Int. J. Cardiovasc. Imaging 2010, 26, 631–640. [Google Scholar] [CrossRef]
- Durrer, C.; Lewis, N.; Wan, Z.; Ainslie, P.N.; Jenkins, N.T.; Little, J.P. Short-Term Low-Carbohydrate High-Fat Diet in Healthy Young Males Renders the Endothelium Susceptible to Hyperglycemia-Induced Damage, An Exploratory Analysis. Nutrients 2019, 11, 489. [Google Scholar] [CrossRef] [Green Version]
- Alian, Z.; Hashemipour, M.; Dehkordi, E.H.; Hovsepian, S.; Amini, M.; Moadab, M.H.; Javanmard, S.H. The effects of folic acid on markers of endothelial function in patients with type 1 diabetes mellitus. Med. Arh. 2012, 66, 12–15. [Google Scholar] [CrossRef] [Green Version]
- Verhaar, M.C.; Wever, R.M.; Kastelein, J.J.; van Dam, T.; Koomans, H.A.; Rabelink, T.J. 5-methyltetrahydrofolate, the active form of folic acid, restores endothelial function in familial hypercholesterolemia. Circulation 1998, 97, 237–241. [Google Scholar] [CrossRef] [Green Version]
- Whisner, C.M.; Angadi, S.S.; Weltman, N.Y.; Weltman, A.; Rodriguez, J.; Patrie, J.T.; Gaesser, G.A. Effects of Low-Fat and High-Fat Meals, with and without Dietary Fiber, on Postprandial Endothelial Function, Triglyceridemia, and Glycemia in Adolescents. Nutrients 2019, 11, 2626. [Google Scholar] [CrossRef] [Green Version]
- Robinson, A.T.; Franklin, N.C.; Norkeviciute, E.; Bian, J.T.; Babana, J.C.; Szczurek, M.R.; Phillips, S.A. Improved arterial flow-mediated dilation after exertion involves hydrogen peroxide in overweight and obese adults following aerobic exercise training. J. Hypertens. 2016, 34, 1309–1316. [Google Scholar] [CrossRef]
- Cavka, A.; Cosic, A.; Jukic, I.; Jelakovic, B.; Lombard, J.H.; Phillips, S.A.; Seric, V.; Mihaljevic, I.; Drenjancevic, I. The role of cyclo-oxygenase-1 in high-salt diet-induced microvascular dysfunction in humans. J. Physiol. 2015, 593, 5313–5324. [Google Scholar] [CrossRef]
- Mahmoud, A.M.; Hwang, C.L.; Szczurek, M.R.; Bian, J.T.; Ranieri, C.; Gutterman, D.D.; Phillips, S.A. Low-Fat Diet Designed for Weight Loss But Not Weight Maintenance Improves Nitric Oxide-Dependent Arteriolar Vasodilation in Obese Adults. Nutrients 2019, 11, 1339. [Google Scholar] [CrossRef] [Green Version]
- Ntaios, G.; Gatselis, N.K.; Makaritsis, K.; Dalekos, G.N. Adipokines as mediators of endothelial function and atherosclerosis. Atherosclerosis 2013, 227, 216–221. [Google Scholar] [CrossRef]
- Korda, M.; Kubant, R.; Patton, S.; Malinski, T. Leptin-induced endothelial dysfunction in obesity. Am. J. Physiol. Heart Circ. Physiol. 2008, 295, H1514–H1521. [Google Scholar] [CrossRef] [Green Version]
- Chen, H.; Montagnani, M.; Funahashi, T.; Shimomura, I.; Quon, M.J. Adiponectin stimulates production of nitric oxide in vascular endothelial cells. J. Biol. Chem. 2003, 278, 45021–45026. [Google Scholar] [CrossRef] [Green Version]
- Gardner, C.D.; Trepanowski, J.F.; Del Gobbo, L.C.; Hauser, M.E.; Rigdon, J.; Ioannidis, J.P.A.; Desai, M.; King, A.C. Effect of Low-Fat vs Low-Carbohydrate Diet on 12-Month Weight Loss in Overweight Adults and the Association With Genotype Pattern or Insulin Secretion: The DIETFITS Randomized Clinical Trial. JAMA 2018, 319, 667–679. [Google Scholar] [CrossRef]
- Yannoutsos, A.; Levy, B.I.; Safar, M.E.; Slama, G.; Blacher, J. Pathophysiology of hypertension: Interactions between macro and microvascular alterations through endothelial dysfunction. J. Hypertens. 2014, 32, 216–224. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| LC without CR Diet (n = 9) | LC with CR Diet (n = 12) | P Between-Groups | |
|---|---|---|---|
| Baseline dietary intake | |||
| Caloric intake, kcal/day | 1993 ± 109 | 2032 ± 161 | 0.9 |
| Carbohydrate, %kcal | 45.8 ± 2.4 | 43.5 ± 1.7 | 0.4 |
| Fat, %kcal | 33.7 ± 3.4 | 36.6 ± 2.9 | 0.5 |
| Protein, %kcal | 18.3 ± 2.5 | 18.5 ± 1.3 | 0.95 |
| Planned/provided diet | |||
| Caloric intake (6 weeks), kcal/day | 2328 ± 129 | 1782 ± 42 | <0.0005 |
| Caloric intake (Week 1–4), kcal/day | - | 1616 ± 46 | - |
| Caloric intake (Week 5–6), kcal/day | - | 2163 ± 57 | - |
| Carbohydrate, %kcal | 10 | - | |
| Fat, %kcal | 60–62 | - | |
| Protein, %kcal | 28–30 | - | |
| Actual dietary intake | |||
| Caloric intake (6 weeks), kcal/day | 2090 ± 132 | 1724 ± 43 | 0.03 |
| Caloric intake (Week 1–4), kcal/day | - | 1596 ± 59 | - |
| Caloric intake (Week 5–6), kcal/day | - | 2054 ± 55 | - |
| Compliance, % | 89.9 ± 2.9 | 96.8 ± 1.7 * | 0.04 |
| Carbohydrate, %kcal | 10.3 ± 0.3 | 10.9 ± 0.4 | 0.5 |
| Fat, %kcal | 60.4 ± 0.3 | 59.9 ± 0.3 | 0.3 |
| Protein, %kcal | 29.3 ± 2.8 | 28.7 ± 0.3 | 0.1 |
| Dietary fiber, g | 24.0 ± 1.7 | 19.4 ± 1.0 * | 0.03 |
| Folate/Folic acid, mcg | 141.2 ± 10.7 | 122.9 ± 7.0 | 0.2 |
| Vitamin C, mg | 80.2 ± 4.8 | 78.2 ± 3.5 | 0.8 |
| Sodium, mg | 3292 ± 195 | 2924 ± 86 | 0.1 |
| Potassium, mg | 2184 ± 342 | 2101 ± 226 | 0.8 |
| Physical activity-step counts | 0.3 | ||
| Baseline, steps/day | 5924 ± 813 | 5587 ± 702 | |
| Week 2, steps/day | 8787 ± 1002 | 6552 ± 797 | |
| Week 4, steps/day | 8622 ± 1251 | 6943 ± 855 | |
| Week 6, steps/day | 7887 ± 1342 | 6868 ± 835 | |
| LC without CR Diet (n = 9) | LC with CR Diet (n = 12) | |||||
|---|---|---|---|---|---|---|
| Baseline | Week 4 | Week 6 | Baseline | Week 4 | Week 6 | |
| Age, year | 33 ± 3 | 32 ± 2 | ||||
| Race | ||||||
| Caucasian, n | 4 (44) | 5 (42) | ||||
| African American, n | 3 (33) | 4 (33) | ||||
| Hispanic, n | 1 (11) | 2 (17) | ||||
| Asian, n | 1 (11) | 1 (8) | ||||
| Body weight, kg b | 89.1 ± 4.6 | 85.7 ± 5.2 * | 85.6 ± 4.5 | 90.0 ± 3.8 | 86.5 ± 3.9 * | 87.5 ± 4.3 |
| BMI, kg/m2 a,b | 33.5 ± 1.0 | 32.8 ± 1.1 | 32.3 ± 0.9 | 32.6 ± 0.8 | 31.2 ± 0.9 | 31.7 ± 0.9 |
| Waist circumference, cm | 96.1 ± 3.0 | 92.7 ± 3.3 | 92.2 ± 2.9 | 95.5 ± 2.7 | 93.6 ± 3.1 | 93.1 ± 3.2 |
| Waist-to-hip ratio | 0.88 ± 0.07 | 0.84 ± 0.05 | 0.84 ± 0.04 | 0.85 ± 0.02 | 0.81 ± 0.02 | 0.79 ± 0.03 |
| Body fat, % b | 44.5 ± 0.7 | 44.1 ± 1.3 | 43.4 ± 0.9 | 43.7 ± 0.9 | 43.9 ± 1.1 | 42.5 ± 1.0 |
| SBP, mmHg | 115 ± 2 | 113 ± 3 | 115 ± 4 | 118 ± 5 | 112 ± 4 | 112 ± 3 |
| DBP, mmHg b | 70 ± 1 | 68 ± 3 | 68 ± 2 | 72 ± 4 | 70 ± 3 | 67 ± 3 |
| Total cholesterol, mg/dL | 180 ± 14 | 194 ± 15 | 190 ± 14 | 185 ± 7 | 181 ± 8 | 182 ± 7 |
| LDL cholesterol, mg/dL | 106 ± 10 | 121 ± 12 | 117 ± 12 | 104 ± 7 | 110 ± 8 | 110 ± 7 |
| HDL cholesterol, mg/dL | 51 ± 4 | 56 ± 3 | 55 ± 3 | 60 ± 4 | 56 ± 3 | 58 ± 3 |
| Triglycerides, mg/Dl a,b | 116 ± 23 | 92 ± 15 | 85 ± 13 | 104 ± 21 | 72 ± 6 | 71 ± 6 |
| Glucose, mg/dL | 89 ± 3 | 93 ± 3 | 91 ± 4 | 93 ± 4 | 89 ± 4 | 87 ± 3 |
| Insulin, μU/mL | 13.9 ± 2.6 | 12.5 ± 2.4 | 12.3 ± 1.7 | 13.5 ± 2.4 | 10.2 ± 2.2 | 11.8 ± 3 |
| HOMA-IR | 3.0 ± 0.6 | 3.0 ± 0.6 | 2.8 ± 0.4 | 3.2 ± 0.7 | 2.4 ± 0.6 | 2.6 ± 0.7 |
| LC without CR Diet (n = 9) | LC with CR Diet (n = 12) | P Group × Time | P Group | P Time | |||
|---|---|---|---|---|---|---|---|
| Brachial Artery | Baseline | Week 6 | Baseline | Week 6 | |||
| FMD, % | 6.5 ± 1.1 | 5.9 ± 1.5 | 7.8 ± 1.4 | 9.6 ± 1.6 | 0.4 | 0.1 | 0.7 |
| Baseline diameter, mm | 3.05 ± 0.17 | 3.15 ± 0.25 | 3.28 ± 0.15 | 3.24 ± 0.12 | 0.4 | 0.5 | 0.7 |
| Maximum diameter, mm | 3.26 ± 0.19 | 3.32 ± 0.24 | 3.52 ± 0.14 | 3.56 ± 0.14 | 0.8 | 0.3 | 0.4 |
| Peak flow, cm/s | 105 ± 12 | 120 ± 12 | 94 ± 10 | 106 ± 10 | 0.8 | 0.4 | 0.08 |
| Peak shear rate, | 334 ± 42 | 373 ± 40 | 269 ± 27 | 300 ± 29 | 0.9 | 0.1 | 0.2 |
| NTG-mediated dilation, % | 25.8 ± 3.8 | 24.7 ± 1.9 | 24.6 ± 2.5 | 28.5 ± 2.3 | 0.9 | 0.99 | 0.4 |
| Baseline diameter, mm | 3.01 ± 0.17 | 3.01 ± 0.20 | 3.34 ± 0.14 | 3.26 ± 0.14 | 0.6 | 0.2 | 0.6 |
| Maximum diameter, mm | 3.83 ± 0.21 | 3.76 ± 0.21 | 4.11 ± 0.13 | 4.16 ± 0.13 | 0.2 | 0.2 | 0.8 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hwang, C.-L.; Ranieri, C.; Szczurek, M.R.; Ellythy, A.M.; Elokda, A.; Mahmoud, A.M.; Phillips, S.A. The Effect of Low-Carbohydrate Diet on Macrovascular and Microvascular Endothelial Function Is Not Affected by the Provision of Caloric Restriction in Women with Obesity: A Randomized Study. Nutrients 2020, 12, 1649. https://doi.org/10.3390/nu12061649
Hwang C-L, Ranieri C, Szczurek MR, Ellythy AM, Elokda A, Mahmoud AM, Phillips SA. The Effect of Low-Carbohydrate Diet on Macrovascular and Microvascular Endothelial Function Is Not Affected by the Provision of Caloric Restriction in Women with Obesity: A Randomized Study. Nutrients. 2020; 12(6):1649. https://doi.org/10.3390/nu12061649
Chicago/Turabian StyleHwang, Chueh-Lung, Christine Ranieri, Mary R. Szczurek, Assem M. Ellythy, Ahmed Elokda, Abeer M. Mahmoud, and Shane A. Phillips. 2020. "The Effect of Low-Carbohydrate Diet on Macrovascular and Microvascular Endothelial Function Is Not Affected by the Provision of Caloric Restriction in Women with Obesity: A Randomized Study" Nutrients 12, no. 6: 1649. https://doi.org/10.3390/nu12061649