Modulation of Exercise-Induced Muscle Damage, Inflammation, and Oxidative Markers by Curcumin Supplementation in a Physically Active Population: A Systematic Review

 ,
,  ,
,  ,
,
Abstract
:1. Introduction
2. Material and Methods
2.1. Search Strategy
2.2. Selection of Articles: Inclusion and Exclusion Criteria
3. Results
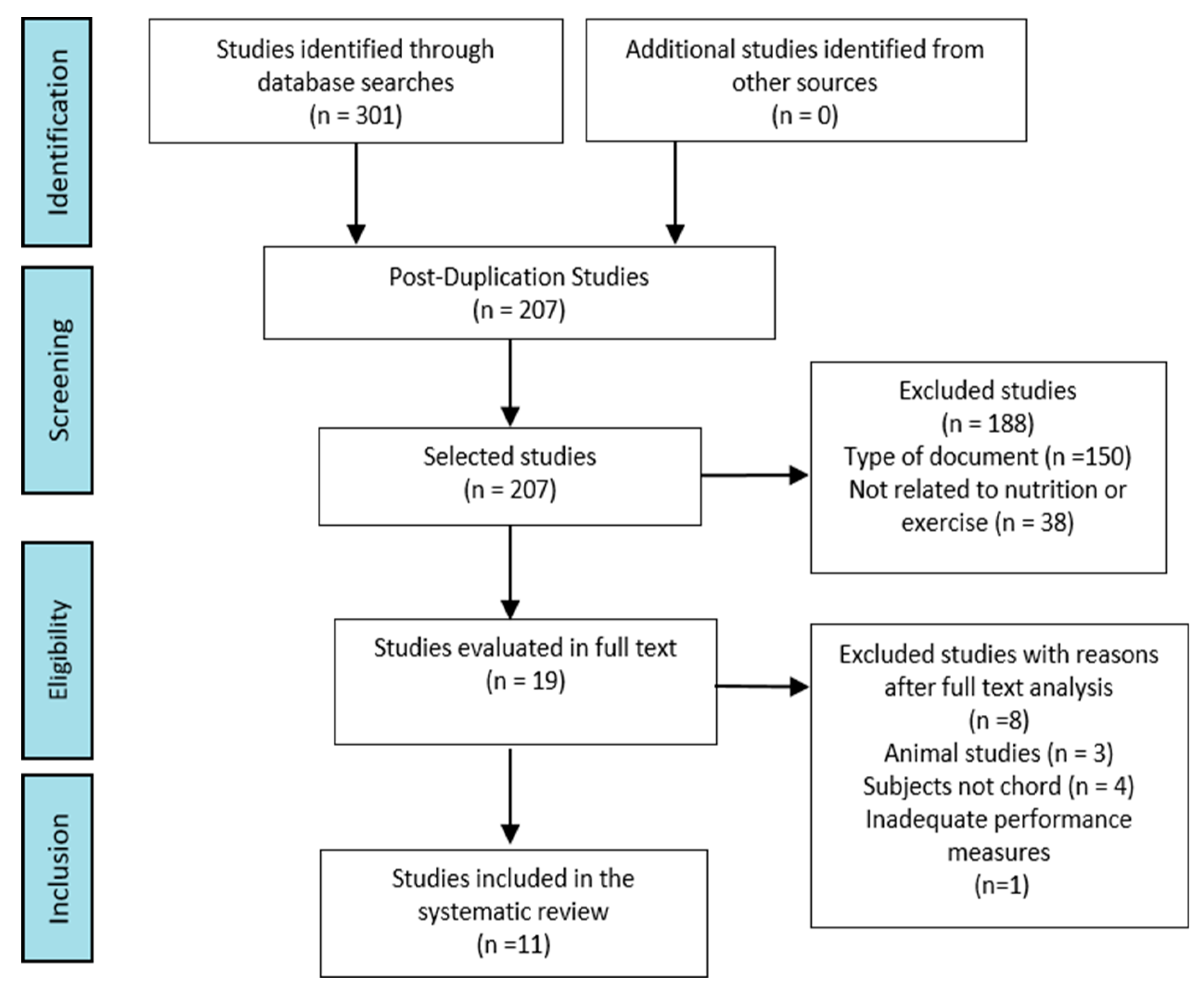
3.1. Selection of Studies
3.2. Characteristics of the Studies
3.3. Outcome Measures
4. Discussion
4.1. Curcumin Supplementation
4.2. Exercise-Induced Muscle Damage (EIMD)
4.2.1. Effect on Muscle Pain
4.2.2. Effect on Muscle Performance
4.2.3. Effect on Muscle Enzyme Activity
4.3. Effect on Inflammatory Markers
4.4. Effect on Oxidative Markers
5. Limitations, Strengths, and Future Lines of Research
6. Practical Applications
7. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Tanabe, Y.; Chino, K.; Ohnishi, T.; Ozawa, H.; Sagayama, H.; Maeda, S.; Takahashi, H. Effects of oral curcumin ingested before or after eccentric exercise on markers of muscle damage and inflammation. Scand. J. Med. Sci. Sport 2018, 29, 524–534. [Google Scholar] [CrossRef]
- Tanabe, Y.; Maeda, S.; Akazawa, N.; Zempo-Miyaki, A.; Choi, Y.; Ra, S.G.; Nosaka, K. Attenuation of indirect markers of eccentric exercise-induced muscle damage by curcumin. Eur. J. Appl. Physiol. 2015, 115, 1949–1957. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fatouros, I.G.; Jamurtas, A.Z. Insights into the molecular etiology of exercise-induced inflammation: Opportunities for optimizing performance. J. Inflamm. Res. 2016, 9, 175–186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sciberras, J.N.; Galloway, S.D.; Fenech, A.; Grech, G.; Farrugia, C.; Duca, D.; Mifsud, J. The effect of turmeric (Curcumin) supplementation on cytokine and inflammatory marker responses following 2 hours of endurance cycling. J. Int. Soc. Sports Nutr. 2015, 12, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drobnic, F.; Riera, J.; Appendino, G.; Togni, S.; Franceschi, F.; Valle, X.; Tur, J. Reduction of delayed onset muscle soreness by a novel curcumin delivery system (Meriva®): A randomised, placebo-controlled trial. J. Int. Soc. Sports Nutr. 2014, 11, 31. [Google Scholar] [CrossRef] [Green Version]
- Schieber, M.; Chandel, N.S. ROS function in redox signaling and oxidative stress. Curr. Biol. 2014, 24, R453–R462. [Google Scholar] [CrossRef] [Green Version]
- He, F.; Li, J.; Liu, Z.; Chuang, C.-C.; Yang, W.; Zuo, L. Redox mechanism of reactive oxygen species in exercise. Front. Physiol. 2016, 7, 486. [Google Scholar] [CrossRef] [Green Version]
- Córdova Martínez, A. Sports Physiology, 1st ed.; Synthesis: Madrid, Spain, 2013; pp. 65–74. [Google Scholar]
- Braakhuis, A.J.; Hopkins, W.G. Impact of dietary antioxidants on sport performance: A review. Sports Med. 2015, 45, 939–955. [Google Scholar] [CrossRef]
- Jäger, R.; Purpura, M.; Kerksick, C.M. Eight Weeks of a High Dose of Curcumin Supplementation May Attenuate Performance Decrements Following Muscle-Damaging Exercise. Nutrients 2019, 11, 1692. [Google Scholar]
- Kocaadam, B.; Şanlier, N. Curcumin, an active component of turmeric (Curcuma longa), and its effects on health. Crit. Rev. Food Sci. Nutr. 2017, 57, 2889–2895. [Google Scholar] [CrossRef]
- Administration USFaD. Generally Recognized as Safe (GRAS) FDA; FDA: Silver Spring, MD, USA, 2016.
- Gaffey, A.; Slater, H.; Porritt, K.; Campbell, J.M. The effects of curcuminoids on musculoskeletal pain: A systematic review. JBI Database Syst. Rev. Implement Rep. 2017, 15, 486–516. [Google Scholar] [CrossRef]
- Harty, P.S.; Cottet, M.L.; Malloy, J.K.; Kerksick, C.M. Nutritional and Supplementation Strategies to Prevent and Attenuate Exercise-Induced Muscle Damage: A Brief Review. Sports Med. Open 2019, 5, 1. [Google Scholar] [CrossRef] [PubMed]
- Hewlings, S.; Kalman, D. Curcumin: A review of its’ effects on human health. Foods 2017, 6, 92. [Google Scholar] [CrossRef] [PubMed]
- Alamdari, N.; O’Neal, P.; Hasselgren, P.-O. Curcumin and muscle wasting—A new role for an old drug? Nutrition 2009, 25, 125–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Derosa, G.; Maffioli, P.; Simental-Mendia, L.E.; Bo, S.; Sahebkar, A. Effect of curcumin on circulating interleukin-6 concentrations: A systematic review and meta-analysis of randomized controlled trials. Pharmacol. Res. 2016, 111, 394–404. [Google Scholar] [CrossRef] [PubMed]
- Noorafshan, A.; Ashkani-Esfahani, S. A review of therapeutic effects of curcumin. Curr. Pharm. Des. 2013, 19, 2032–2046. [Google Scholar] [PubMed]
- Hatcher, H.; Planalp, R.; Cho, J.; Torti, F.; Torti, S. Curcumin: From ancient medicine to current clinical trials. Cell Mol. Life Sci. 2008, 65, 1631–1652. [Google Scholar] [CrossRef]
- Kahkhaie, K.R.; Mirhosseini, A.; Aliabadi, A.; Mohammadi, A.; Haftcheshmeh, S.M.; Sathyapalan, T.; Sahebkar, A. Curcumin: A modulator of inflammatory signaling pathways in the immune system. Inflammopharmacology 2019, 27, 885–900. [Google Scholar] [CrossRef]
- Sahebkar, A.; Cicero, A.F.; Simental-Mendia, L.E.; Aggarwal, B.B.; Gupta, S.C. Curcumin downregulates human tumor necrosis factor-α levels: A systematic review and meta-analysis ofrandomized controlled trials. Pharmacol. Res. 2016, 107, 234–242. [Google Scholar] [CrossRef]
- Dunsmore, K.E.; Chen, P.G.; Wong, H.R. Curcumin, a medicinal herbal compound capable of inducing the heat shock response. Cri. Care Med. 2001, 29, 2199–2204. [Google Scholar] [CrossRef]
- Thitimuta, S.; Pithayanukul, P.; Nithitanakool, S.; Bavovada, R.; Leanpolchareanchai, J.; Saparpakorn, P. Camellia sinensis l. Extract and its potential beneficial effects in antioxidant, anti-inflammatory, anti-hepatotoxic, and anti-tyrosinase activities. Molecules 2017, 22, 401. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakhostin-Roohi, B.; Nasirvand Moradlou, A.; Mahmoodi Hamidabad, S.; Ghanivand, B. The effect of curcumin supplementation on selected markers of delayed onset muscle soreness (DOMS). Ann. Appl. Sport Sci. 2016, 4, 25–31. [Google Scholar] [CrossRef] [Green Version]
- Tanabe, Y.; Chino, K.; Sagayama, H.; Lee, H.J.; Ozawa, H.; Maeda, S.; Takahashi, H. Effective Timing of Curcumin Ingestion to Attenuate Eccentric Exercise-Induced Muscle Soreness in Men. J. Nutr. Sci. Vitaminol. 2019, 65, 82–89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kopec, T.J. Performance Recovery Following Exercise Induced Muscle Damage (EIMD) through an Exhaustive Bout of Exercise. Ph.D. Thesis, University of Alabama, Tuscaloosa, AL, USA, 2016. [Google Scholar]
- Hutton, B.; Catalá-López, F.; Moher, D. La extensión de la declaración PRISMA para revisiones sistemáticas que incorporan metaanálisis en red: PRISMA-NMA. Med. Clin. 2016, 147, 262–266. [Google Scholar] [CrossRef] [PubMed]
- Nicol, L.M.; Rowlands, D.S.; Fazakerly, R.; Kellett, J. Curcumin supplementation likely attenuates delayed onset muscle soreness (DOMS). Eur. J. Appl. Physiol. 2015, 115, 1769–1777. [Google Scholar] [CrossRef] [PubMed]
- Law, M.; Stewart, D.; Pollock, N.; Letts, L.; Bosch, J.; Westmorland, M. Guidelines for Critical Review Form—Quantitative Studies 1998; McMaster University: Hamilton, ON, Canada, 2008. [Google Scholar]
- McFarlin, B.K.; Venable, A.S.; Henning, A.L.; Sampson, J.N.B.; Pennel, K.; Vingren, J.L.; Hill, D.W. Reduced inflammatory and muscle damage biomarkers following oral supplementation with bioavailable curcumin. BBA Clin. 2016, 5, 72–78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delecroix, B.; Abaïdia, A.E.; Leduc, C.; Dawson, B.; Dupont, G. Curcumin and piperine supplementation and recovery following exercise induced muscle damage: A randomized controlled trial. J. Sport Sci. Med. 2017, 16, 147–153. [Google Scholar]
- Basham, S.A.; Waldman, H.S.; Krings, B.M.; Lamberth, J.; Smith, J.W.; McAllister, M.J. Effect of Curcumin Supplementation on Exercise-Induced Oxidative Stress, Inflammation, Muscle Damage, and Muscle Soreness. J. Diet Suppl. 2019, 1, 1–14. [Google Scholar] [CrossRef]
- Authority EFS. Refined exposure assessment for curcumin (E 100). EFSA J. 2014, 12, 3876. [Google Scholar] [CrossRef]
- Krishnakumar, I.; Kumar, D.; Ninan, E.; Kuttan, R.; Maliakel, B. Enhanced absorption and pharmacokinetics of fresh turmeric (Curcuma longa L) derived curcuminoids in comparison with the standard curcumin from dried rhizomes. J. Funct. Foods 2015, 17, 55–65. [Google Scholar] [CrossRef]
- Oliver, J.M.; Stoner, L.; Rowlands, D.S.; Caldwell, A.R.; Sanders, E.; Kreutzer, A.; Jäger, R. Novel form of curcumin improves endothelial function in young, healthy individuals: A double-blind placebo controlled study. J. Nutr. Metab. 2016, 1, E1089653. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tabrizi, R.; Vakili, S.; Akbari, M.; Mirhosseini, N.; Lankarani, K.B.; Rahimi, M.; Asemi, Z. The effects of curcumin-containing supplements on biomarkers of inflammation and oxidative stress: A systematic review and meta-analysis of randomized controlled trials. Phytother. Res. 2019, 33, 253–262. [Google Scholar] [CrossRef] [PubMed]
- Daily, J.W.; Yang, M.; Park, S. Efficacy of turmeric extracts and curcumin for alleviating the symptoms of joint arthritis: A systematic review and meta-analysis of randomized clinical trials. J. Med. Food 2016, 19, 717–729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shen, L.; Liu, C.-C.; An, C.-Y.; Ji, H.-F. How does curcumin work with poor bioavailability? Clues from experimental and theoretical studies. Sci. Rep. 2018, 6, 20872. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.H.; Kim, H.Y.; Back, S.Y.; Han, H.-K. Piperine-mediated drug interactions and formulation strategy for piperine: Recent advances and future perspectives. Expert Opin. Drug Metab. Toxicol. 2018, 14, 43–57. [Google Scholar] [CrossRef]
- Proske, U.; Morgan, D.L. Muscle damage from eccentric exercise: Mechanism, mechanical signs, adaptation and clinical applications. J. Physiol. 2001, 537, 333–345. [Google Scholar] [CrossRef]
- Järvinen, T.A.; Järvinen, M.; Kalimo, H. Regeneration of injured skeletal muscle after the injury. Muscles Ligaments Tendons 2013, 3, 337–345. [Google Scholar] [CrossRef] [Green Version]
- Kirkpatrick, D.R.; McEntire, D.M.; Smith, T.A.; Dueck, N.P.; Kerfeld, M.J.; Hambsch, Z.J.; Agrawal, D.K. Transmission pathways and mediators as the basis for clinical pharmacology of pain. Expert Rev. Clin. Pharmacol. 2016, 9, 1363–1387. [Google Scholar] [CrossRef]
- Nosaka, K. Effects of amino acid supplementation on muscle soreness and damage. Int. J. Sport Nutr. Exerc. Metab. 2006, 16, 620–635. [Google Scholar] [CrossRef] [Green Version]
- Cook, C.J.; Beaven, C.M. Individual perception of recovery is related to subsequent sprint performance. Br. J. Sports Med. 2013, 47, 705–709. [Google Scholar] [CrossRef]
- Wainstein, G.E. Patogénesis de la artrosis. Rev. Med. Clin. Las. Condes. 2014, 25, 723–727. [Google Scholar]
- Córdova, A.; Mielgo-Ayuso, J.; Fernandez-Lazaro, C.I.; Caballero-García, A.; Roche, E.; Fernández-Lázaro, D. Effect of Iron Supplementation on the Modulation of Iron Metabolism, Muscle Damage Biomarkers and Cortisol in Professional Cyclists. Nutrients 2019, 11, 500. [Google Scholar]
- Moriyuki, K.; Sekiguchi, F.; Matsubara, K.; Nishikawa, H.; Kawabata, A. Curcumin inhibits the proteinase-activated receptor-2–triggered prostaglandin E2 production by suppressing cyclooxygenase-2 upregulation and Akt-dependent activation of nuclear factor-κB in human lung epithelial cells. J. Pharmacol. Sci. 2010, 114, 225–229. [Google Scholar] [CrossRef] [PubMed]
- Engel, F.A.; Holmberg, H.-C.; Sperlich, B. Is there evidence that runners can benefit from wearing compression clothing? Sports Med. 2016, 46, 1939–1952. [Google Scholar] [CrossRef]
- Georganas, C.; Liu, H.; Perlman, H.; Hoffmann, A.; Thimmapaya, B.; Pope, R.M. Regulation of IL-6 and IL-8 expression in rheumatoid arthritis synovial fibroblasts: The dominant role for NF-κB but not C/EBPβ or c-Jun. J. Immunol. 2000, 165, 7199–7206. [Google Scholar] [CrossRef] [Green Version]
- Dongari-Bagtzoglou, A.I.; Ebersole, J.L. Increased presence of interleukin-6 (IL-6) and IL-8 secreting fibroblast subpopulations in adult periodontitis. J. Periodontol. 1998, 69, 899–910. [Google Scholar] [CrossRef]
- Ranchordas, M.K.; Rogerson, D.; Soltani, H.; Costello, J.T. Antioxidants for preventing and reducing muscle soreness after exercise. Cochrane Database Syst. Rev. 2014, 12, CD009789. [Google Scholar]
- Miranda, C.; Ela, M.; Hernández Lantigua, I.; Llópiz Janer, N. Enzimas que participan como barreras fisiológicas para eliminar los radicales libres: II. Catalasa. Rev. Cubana Invest. Biomed. 1996, 15, 5–11. [Google Scholar]
- Trivedi, M.K.; Mondal, S.C.; Gangwar, M.; Jana, S. Immunomodulatory potential of nanocurcumin-based formulation. Inflammopharmacology 2017, 25, 609–619. [Google Scholar] [CrossRef]
- Patil, U.K.; Singh, A.; Charkraborty, A.K. Role of piperine as a bioavaility enhacer. Inter. J. Recent Advan. Pharma. Resear. 2011, 4, 16–23. [Google Scholar]
- Owens, D.J.; Twist, C.; Cobley, J.N.; Howatson, G.; Close, G.L. Exercise-induced muscle damage: What is it, what causes it and what are the nutritional solutions? Eur. J. Sport Sci. 2019, 19, 71–78. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| References | Drobnic et al., 2014 [5] | Sciberras et al., 2015 [4] | Nicol et al., 2015 [28] | Tanabe et al., 2015 [2] | McFarlin et al., 2016 [30] | Nakhostin-Roohi et al., 2016 [24] | Delecroix et al., 2017 [31] | Tanabe et al., 2018 [1] | Tanabe et al., 2019 [25] | Jäger et al., 2019 [10] | Basham et al., 2019 [32] | TI | |
| ITEMS | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 10 |
| 2 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 10 | |
| 3 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 10 | |
| 4 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 10 | |
| 5 | 0 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 4 | |
| 6 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 7 | |
| 7 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 10 | |
| 8 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 10 | |
| 9 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 10 | |
| 10 | 1 | 1 | 0 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 7 | |
| 11 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 10 | |
| 12 | 1 | 0 | 0 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 3 | |
| 13 | 0 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 6 | |
| 14 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 10 | |
| 15 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 1 | 0 | 7 | |
| 16 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 6 | |
| TS | 13 | 14 | 12 | 14 | 14 | 13 | 12 | 15 | 14 | 15 | 14 | ||
| % | 81.3 | 87.5 | 75 | 87.5 | 87.5 | 81.3 | 75 | 93.8 | 87.5 | 93.8 | 87.5 | ||
| MQ | VG | VG | G | VG | VG | VG | G | E | VG | E | VG | ||
| Level of Participants | Elite Athletes | 1 Study [31] |
| Moderately Active | 5 Studies [4,5,10,28,32] | |
| No Regular Training before the Study | 5 Studies [1,2,24,25,30] | |
| Type of Administration of Curcumin | Commercially available curcumin supplement | 10 studies [1,2,4,5,10,24,25,30,31,32] |
| Curcumin capsule made for the study | 1 study [28] | |
| Dosage Used | 150 mg/day | 1 study [24] |
| 180 mg/day (2 doses of 90 mg/day) | 2 studies [1,25] | |
| 300 mg /day (2 doses of 150 mg/day) | 1 study [2] | |
| 400 mg/day | 1 study [30] | |
| 400 mg /day (2 doses of 200 mg/day) | 1 study [5] | |
| 500 mg / day | 1 study [4] | |
| 5 g/day (2 doses of 2.5 g/day) | 1 study [28] | |
| 6 g of curcumin + 60 mg of piperine/day (3 doses of 2 g of curcumin + 20 mg of piperine/day) | 1 study [31] | |
| 600 mg/day (3 doses of 200 mg of curcumin) | 1 study [10] | |
| 1500 mg/day (3 doses of 500 mg of curcumin) | 1 study [32] | |
| Moment of Supplementation | Before Exercise | 1 study [4] |
| Before and After Exercise | 9 studies [1,2,5,10,25,28,30,31,32] | |
| After Exercise | 1 study [24] | |
| Duration of Treatment | 1 day | 2 studies [2,24] |
| 4 days | 3 studies [4,5,31] | |
| 6 days | 2 studies [28,30] | |
| 7 days | 2 studies [1,25] | |
| 56 days | 1 study [10] | |
| 28 days | 1 study [32] |
| A. Summary of Studies Included in This Systematic Review. | |||||
| Author/s—Year | Study Design | Population | Intervention | Analyzed Results | Main Conclusions |
| Drobnic et al., 2014 [5] | Randomized controlled trial single-blind | 20 moderately active men (38.1 ± 11.1 years and 32.7 ± 12.3 years) | 200 mg curcumin capsules (Phytosome Meriva) twice a day 48 h before exercise and for 24 h after | Evidence of muscle injury by MRI | ↓ RT and LT posterior and medial |
| CRP, hsCRP, ERS, MCP-1, FRAP, CAT, GPx, CK | † CRP, hsCRP, ERS, MCP-1, FRAP, CAT, GPx, CK | ||||
| IL-8 | ↓ IL-8 | ||||
| Intensity of pain | † Intensity of pain | ||||
| Sciberras et al., 2015 [4] | Double-blind randomized cross-over. Subjects performed three trials in total (supplement/placebo and control) | 11 male recreational athletes (35.5 ± 5.7 years) | 500 mg of curcumin in capsules (Meriva Curcumin) 72 h before and immediately before exercise | RPE | † RPE |
| Cortisol, PCR, Hto, Hb, | † Cortisol, PCR, Hto, Hb, | ||||
| WBC, Neutrophils, IL-6, | WBC, Neutrophils, IL-6, | ||||
| IL1-RA, IL-10 | IL1-RA, IL-10 | ||||
| Questionnaire DALDA | ↑ “better than usual” | ||||
| Nicol et al., 2015 [28] | Double-blind crossover randomized controlled trial | 17 moderately active men (33.8 ± 5.4 years) | 2.5 g of curcumin in capsules, 48 h before the exercise and for 72 h after | Muscle pain—VAS | ↓ Muscle pain: squatting jump (1.5−1.1; ± 1.2); Stretch butt (−1.0a-1.9; ± 0.9); Sitting on one leg (−1.4a−1.7; 90% CL ± 1.0) |
| Jump height to one leg | ↑ Jump 1 leg (15%; 90% CL ± 1 2%) | ||||
| CK | ↓ CK 24 and 48 h before (−22%; 90% CL ± 22%), (−29%; ± 21%) | ||||
| IL-6 | ↑ IL-6 at 0-h (31%; ± 29%) and 48 h (32%; ± 29%) ↓ 24 h post-exercise (−20%; ± 18%) | ||||
| TNF-α | † TNF-α | ||||
| Tanabe et al., 2015 [2] | Single-blind crossover randomized controlled trial | 14 young men without regular resistance training (23.5 ± 2.3 years) | 150 mg curcumin capsules (Theracurcumin Theravalues) twice a day 1 h before exercise and 12 h later | MVC Torque | ↓ MVC Torque |
| ROM | † ROM | ||||
| Upper arm circumference | † Upper arm circumference | ||||
| Muscle pain—VAS | †VAS | ||||
| CK | ↓ CK (maximum activity) | ||||
| IL-6 | † IL-6 | ||||
| TNF-α | † TNF-α | ||||
| B. Summary of Studies Included in This Systematic Review (Continued) | |||||
| Author/s—Year | Study Design | Population | Intervention | Analyzed Results | Main Conclusions |
| McFarlin et al., 2016 [30] | Randomized controlled trial double blind | 28 men and women without regular resistance training (20 ± 1 ages and 19 ± 2 ages) | 400mg curcumin capsules (Long-life) 48h before exercise and for 72h after | Subjective quadriceps pain | † Subjective quadriceps pain |
| ADL | †ADL | ||||
| CK | ↓CK | ||||
| TNF-α | ↓TNF-α | ||||
| IL-6 | †IL-6 | ||||
| IL-8 | ↓IL-8 | ||||
| IL-10 | †IL-10 | ||||
| Nakhostin-Roohi et al., 2016 [24] | Controlled test randomized crossed double-blind | 10 young men without regular training with weights (25.0 ± 1.6 years) | 150 mg of curcumin gin capsules (Theravalues) Immediately after exercise | Muscle pain—VAS | ↓ VAS 48–72 h |
| TAC | ↑ TAC | ||||
| CK | ↓ CK | ||||
| ALT | ↓ ALT | ||||
| AST | ↓ AST | ||||
| Delecroix et al., 2017 [31] | A randomized, balanced cross-over | 10 rugby players elite level (20.7 ± 1.4 years) | 2 g curcumin + 20 mg of piperine in capsules (MGD Nature) 3 times/day48h before exercise and for 48 h after exercise | 6-s power sprint | < Group reduction EXP: (−1.77 ± 7.25%; 1277 ± 153 W). CON Group (−13.6 ± 13.0%; 1130 ± 241 W) |
| CMJ | ↑ CMJ (ES = −0.56; CI 90% = 0.81−0.32) | ||||
| CK | † CK 24, 48, 72 h post-exercise | ||||
| Muscle pain—Hooper scale | † Muscle pain—Hooper scale | ||||
| Subjective quadriceps pain | † Subjective quadriceps pain | ||||
| Tanabe et al., 2018 [1] | Double-blind crossover randomized controlled trial | Exp1: 10 men (28.5 ± 3.4 years) Exp2: 10 men (29.0 ± 3.9 years) Both untrained 3-7 days prior to assay | 90mg curcumin capsules (Theracurcumin Theravalues) 2 times/day Exp1: 7 days before exercise Exp2: 7 days after exercise | MVC Torque | Exp1:† Exp2:↑ MVC Torque |
| ROM | Exp1:† Exp2:↑ ROM | ||||
| Muscle pain -VAS | Exp1:† Exp2: ↓ VAS | ||||
| T2 | Exp1:† Exp2: † T2 | ||||
| CK | Exp1:† Exp2:↓ CK | ||||
| TNF- α | Exp1:† Exp2: † TNF- α | ||||
| IL-8 | Exp1: ↓ Exp2: † IL-8 | ||||
| d-ROMs | Exp1:† Exp2: † d-ROMs | ||||
| BAP | Exp1:† Exp2: † BAP | ||||
| Tanabe et al., 2019 [25] | Single-Blind Parallel Randomized Trial | 24 young men without intense training during the study period PRE (28.8 ± 3.6 years) POST (29.8 ± 3.4 years) CON (28.0 ± 3.2 years) | 90 mg curcumin capsules (Theracurcumin Theravalues) twice a day PRE: 7 days before exercise POST: 4 days after exercise CON: 4 days after exercise | MVC Torque | PRE: † POST: † MVC Torque |
| ROM | PRE: † POST: ↑ ROM | ||||
| Muscle pain—VAS | PRE: † POST: ↓ VAS | ||||
| CK | PRE: † POST: † CK | ||||
| C. Summary of Studies Included in This Systematic Review (Continued) | |||||
| Author/s—Year | Study Design | Population | Intervention | Analyzed Results | Main Conclusions |
| Jäger et al., 2019 [10] | Randomized controlled trial double-blind | 63 men (31) and women (32) (21 ± 2 years) physically active meeting ACSM guidelines | G1: Placebo (PLB) G2: 50 mg curcumin in capsules (CurcuWIN®)G3: 200 mg curcumin in capsules (CurcuWIN®)3 times/day (breakfast/lunch/dinner) | Subjective muscle pain anterior, posterior, and total scale 100 mm Maximum extension torque and isokinetic flexion Extension power and isokinetic flexion Isometric torque Measurements: 1 h, 24 h, 48 h, and 72 h post-exercise | ↑ Subjective muscle pain (anterior, posterior) G 1, 2, and 3 † Subjective (total) muscle pain G3 1 h and 24 h post-exercise † Maximum bending torque G2 † Bending power G2 |
| Basham et al., 2019 [32] | Randomized controlled trial double-blind | 20 men elite level (21.7 ± 2.9 years) physically active compliance with ACSM guidelines | 1.5 g curcumin/69 mg curcuminoids 500 mg capsule (CurcuFresh, NOW FoodsUSA) twice a day (2 breakfast/1 dinner) | Oxidative stress Inflammation Muscle damage Muscle pain | ↓ CK (p < 0.0001) ↓ VAS (p = 0.012) &TAC &MDA &TNF-α |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernández-Lázaro, D.; Mielgo-Ayuso, J.; Seco Calvo, J.; Córdova Martínez, A.; Caballero García, A.; Fernandez-Lazaro, C.I. Modulation of Exercise-Induced Muscle Damage, Inflammation, and Oxidative Markers by Curcumin Supplementation in a Physically Active Population: A Systematic Review. Nutrients 2020, 12, 501. https://doi.org/10.3390/nu12020501
Fernández-Lázaro D, Mielgo-Ayuso J, Seco Calvo J, Córdova Martínez A, Caballero García A, Fernandez-Lazaro CI. Modulation of Exercise-Induced Muscle Damage, Inflammation, and Oxidative Markers by Curcumin Supplementation in a Physically Active Population: A Systematic Review. Nutrients. 2020; 12(2):501. https://doi.org/10.3390/nu12020501
Chicago/Turabian StyleFernández-Lázaro, Diego, Juan Mielgo-Ayuso, Jesús Seco Calvo, Alfredo Córdova Martínez, Alberto Caballero García, and Cesar I. Fernandez-Lazaro. 2020. "Modulation of Exercise-Induced Muscle Damage, Inflammation, and Oxidative Markers by Curcumin Supplementation in a Physically Active Population: A Systematic Review" Nutrients 12, no. 2: 501. https://doi.org/10.3390/nu12020501