
Utilizing a Human–Computer Interaction Approach to Evaluate the Design of Current Pharmacogenomics Clinical Decision Support

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting
2.2. Participant Recruitment
2.3. Scenario Development
2.4. Simulation Procedure
2.5. Data Collection and Outcome Measures
3. Results
3.1. Participant Characteristics
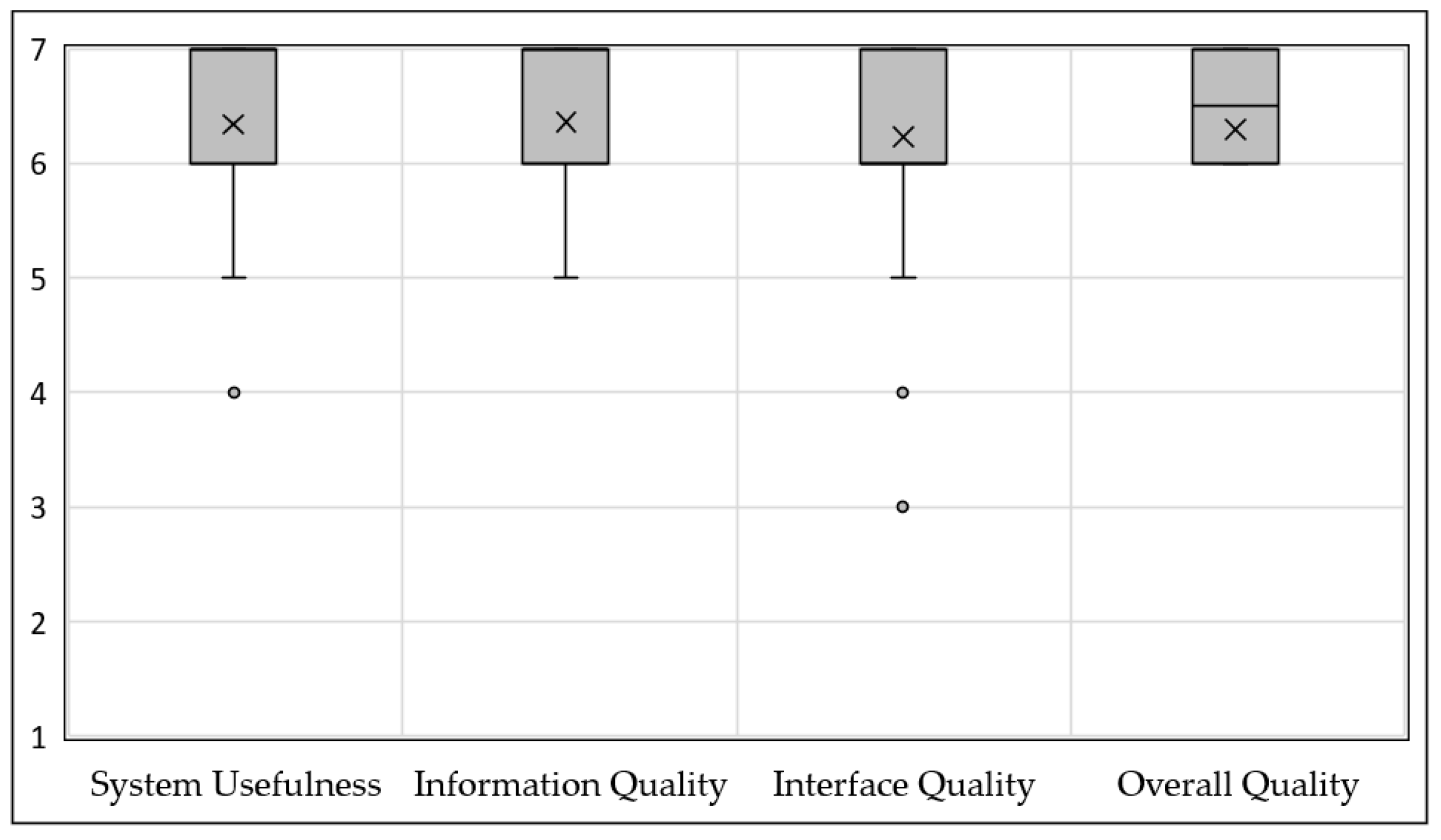
3.2. Satisfaction
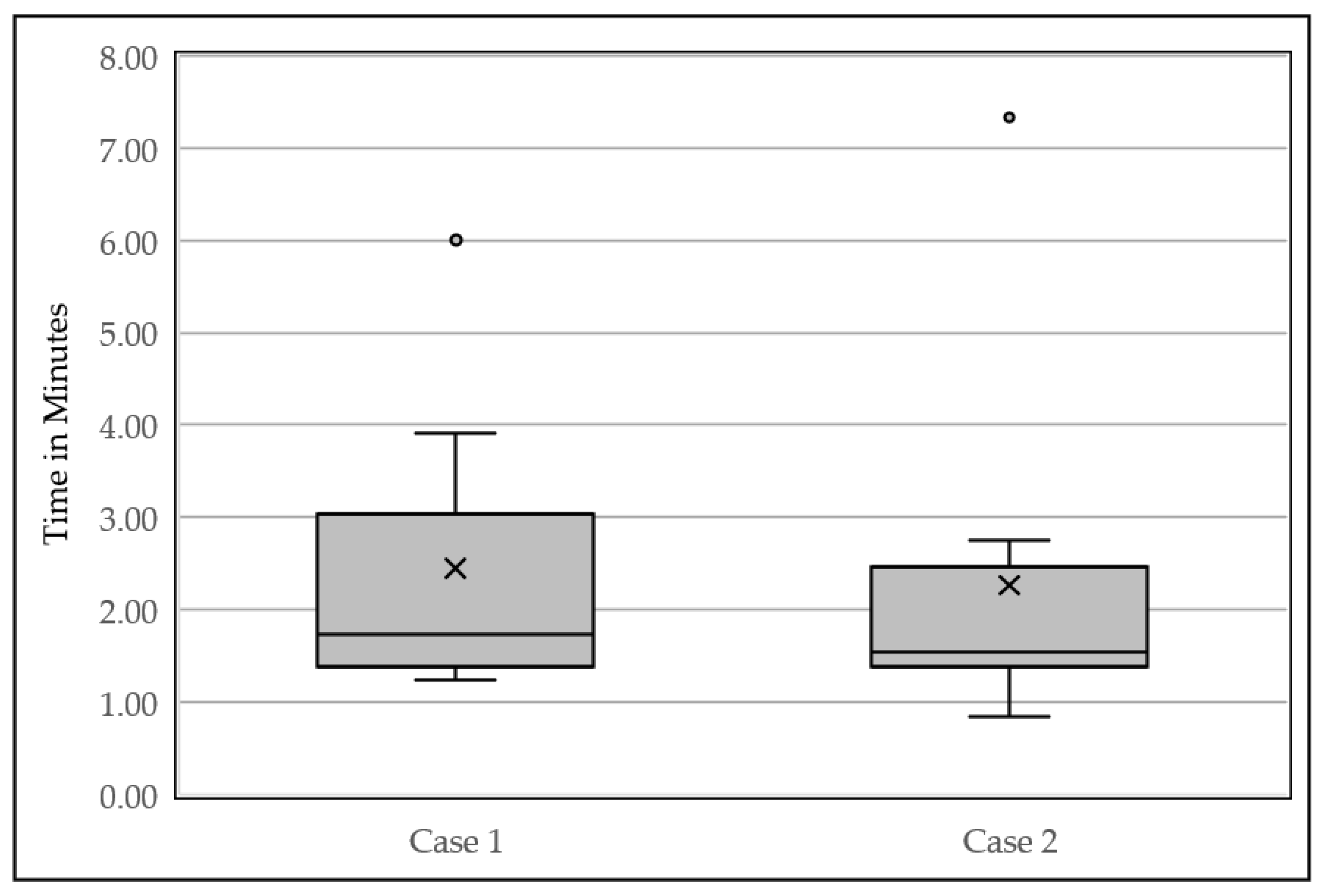
3.3. Efficiency
3.4. Emerging Themes Identified from the Usability Session
3.4.1. Usability
3.4.2. Visibility
3.4.3. Workflow
3.4.4. Content
3.4.5. Understandability
3.4.6. Medical Usefulness
3.4.7. Navigation
4. Discussion
Future Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hicks, J.K.; Dunnenberger, H.M.; Gumpper, K.F.; Haidar, C.E.; Hoffman, J.M. Integrating pharmacogenomics into electronic health records with clinical decision support. Am. J. Health-Syst. Pharm. 2016, 73, 1967–1976. [Google Scholar] [CrossRef] [PubMed]
- Johnson, J.A. Pharmacogenetics: Potential for individualized drug therapy through genetics. Trends Genet. 2003, 19, 660–666. [Google Scholar] [CrossRef]
- van de Velde, S.; Heselmans, A.; Delvaux, N.; Brandt, L.; Marco-Ruiz, L.; Spitaels, D.; Cloetens, H.; Kortteisto, T.; Roshanov, P.; Kunnamo, I.; et al. A systematic review of trials evaluating success factors of interventions with computerised clinical decision support. Implement. Sci. 2018, 13, 114. [Google Scholar] [CrossRef] [PubMed]
- Kilbridge, P.M.; Classen, D.C. The Informatics Opportunities at the Intersection of Patient Safety and Clinical Informatics. J. Am. Med. Inform. Assoc. 2008, 15, 397–407. [Google Scholar] [CrossRef]
- Teich, J.M.; Osheroff, J.A.; Pifer, E.A.; Sittig, D.F.; Jenders, R.A. Clinical Decision Support in Electronic Prescribing: Recommendations and an Action Plan: Report of the Joint Clinical Decision Support Workgroup. J. Am. Med. Inform. Assoc. 2005, 12, 365–376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malsagova, K.A.; Butkova, T.V.; Kopylov, A.T.; Izotov, A.A.; Potoldykova, N.V.; Enikeev, D.V.; Grigoryan, V.; Tarasov, A.; Stepanov, A.A.; Kaysheva, A.L. Pharmacogenetic Testing: A Tool for Personalized Drug Therapy Optimization. Pharmaceutics 2020, 12, 1240. [Google Scholar] [CrossRef] [PubMed]
- Weitzel, K.W.; Aquilante, C.L.; Johnson, S.; Kisor, D.F.; Empey, P.E. Educational strategies to enable expansion of pharmacogenomics-based care. Am. J. Health-Syst. Pharm. 2016, 73, 1986–1998. [Google Scholar] [CrossRef] [PubMed]
- Rohrer Vitek, C.R.; Abul-Husn, N.S.; Connolly, J.J.; Hartzler, A.L.; Kitchner, T.; Peterson, J.F.; Rasmussen, L.V.; Smith, M.E.; Stallings, S.; Williams, M.S.; et al. Healthcare provider education to support integration of pharmacogenomics in practice: The eMERGE Network experience. Pharmacogenomics 2017, 18, 1013–1025. [Google Scholar] [CrossRef] [PubMed]
- Kawamoto, K.; Houlihan, C.A.; Balas, E.A.; Lobach, D.F. Improving clinical practice using clinical decision support systems: A systematic review of trials to identify features critical to success. BMJ Br. Med. J. 2005, 330, 765. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, K.A.; Patel, H.; Haggstrom, D.A.; Zillich, A.J.; Imperiale, T.F.; Russ, A.L. Utilizing a user-centered approach to develop and assess pharmacogenomic clinical decision support for thiopurine methyltransferase. BMC Med. Inform. Decis. Mak. 2019, 19, 194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khelifi, M.; Tarczy-Hornoch, P.; Devine, E.B.; Pratt, W. Design Recommendations for Pharmacogenomics Clinical Decision Support Systems. AMIA Summits Transl. Sci. Proc. 2017, 2017, 237–246. [Google Scholar] [PubMed]
- Wake, D.T.; Smith, D.M.; Kazi, S.; Dunnenberger, H.M. Pharmacogenomic Clinical Decision Support: A Review, How-to Guide, and Future Vision. Clin. Pharmacol. Ther. 2021, 8. [Google Scholar] [CrossRef] [PubMed]
- Kawamoto, K.; Lobach, D.F.; Willard, H.F.; Ginsburg, G.S. A national clinical decision support infrastructure to enable the widespread and consistent practice of genomic and personalized medicine. BMC Med. Inform. Decis. Mak. 2009, 9. [Google Scholar] [CrossRef] [Green Version]
- Siek, K.A. Expanding Human Computer Interaction Methods to Understand User Needs in the Design Process of Personal Health Systems. Yearb. Med. Inform. 2018, 27, 74–78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hochheiser, H.; Valdez, R.S. Human-Computer Interaction, Ethics, and Biomedical Informatics. Yearb. Med. Inform. 2020, 29, 93–98. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.; McCullagh, L.; Press, A.; Kharche, M.; Schachter, A.; Pardo, S. Formative assessment and design of a complex clinical decision support tool for pulmonary embolism. Evid.-Based Med. 2016, 21, 7–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fossum, M.; Ehnfors, M.; Fruhling, A.; Ehrenberg, A. An evaluation of the usability of a computerized decision support system for nursing homes. Appl. Clin. Inform. 2011, 2, 420–436. [Google Scholar] [PubMed] [Green Version]
- Dolin, R.H.; Boxwala, A.; Shalaby, J. A Pharmacogenomics Clinical Decision Support Service Based on FHIR and CDS Hooks. Methods Inf. Med. 2018, 57, e115–e123. [Google Scholar] [CrossRef] [Green Version]
- Richardson, S.; Mishuris, R.; O’Connell, A.; Feldstein, D.; Hess, R.; Smith, P.; McCullagh, L.; McGinn, T.; Mann, D. “Think aloud” and “Near live” usability testing of two complex clinical decision support tools. Int. J. Med. Inform. 2017, 106, 1–8. [Google Scholar] [CrossRef]
- Nielsen, J. Ten Usability Heuristics. 2020. Available online: http://www.nngroup.com/articles/ten-usability-heuristics/ (accessed on 9 November 2021).
- Devine, E.B.; Lee, C.J.; Overby, C.L.; Abernethy, N.; McCune, J.; Smith, J.W.; Tarczy-Hornoch, P. Usability evaluation of pharmacogenomics clinical decision support aids and clinical knowledge resources in a computerized provider order entry system: A mixed methods approach. Int. J. Med. Inform. 2014, 83, 473–483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nielsen, J.; Landauer, T.K. A mathematical model of the finding of usability problems. In Proceedings of the INTERACT ‘93 and CHI ‘93 Conference on Human Factors in Computing Systems, Amsterdam, The Netherlands, 24–29 April 1993; Association for Computing Machinery: New York, NY, USA, 1993. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Coding Category | Definition |
|---|---|
| Usability | Ease of use of the CDS tool, ability to use with minimal effort. This can be both positive and negative (usability errors). |
| Visibility | Ability to quickly recognize key messages and instructions provided by the CDS tool. Colors and symbols are examples of how messages can be easily recognized in the CDS. |
| Workflow | Ability of the CDS tool to fit into the natural order of events in a patient encounter. |
| Content | Medical accuracy or appropriateness of CDS tool text included as orders, patient information, documentation. |
| Understandability | Ability to quickly comprehend meaning of text, instructions, and the purpose of CDS components. |
| Medical Usefulness | Improves clinical decision-making during encounter. |
| Navigation | Ability to move easily through the CDS tool. |
| Characteristics | n = 10 |
|---|---|
| Female Sex (%) | 6 (60) |
| Race (%) | |
| Asian | 2 (20) |
| White | 7 (70) |
| I prefer not to answer | 1 (10) |
| Age (avg ± SD) | 37 ± 10 |
| Degrees/Certification (%) | |
| MD | 9 (90) |
| DO | 1 (10) |
| Other | 0 (0) |
| Years working at UF (%) | |
| Less than 1 year | 1 (10) |
| 1–10 years | 8 (80) |
| 11–20 years | 1 (10) |
| Years using EPIC® EHR (%) | |
| Less than 1 year | 0 (0) |
| 1–10 years | 9 (90) |
| 11–20 years | 1 (10) |
| How often do you encounter PGx BPAs a month (avg)? (%) | |
| Less than once a month | 7 (70) |
| 1–10 times a month | 2 (20) |
| 11–20 times a month | 1 (10) |
| Uncorrectable visual impairments or color blindness (%) | |
| No | 10 (100) |
| Code | Themes | Example | |
|---|---|---|---|
| 1. Usability | Positive |
|
|
|
| ||
| Negative |
|
| |
|
| ||
| Suggestions |
|
| |
|
| ||
| 2. Visibility | Positive |
|
|
|
| ||
|
| ||
| Negative |
|
| |
|
| ||
|
| ||
|
| ||
|
| ||
|
| ||
| Suggestions |
|
| |
|
| ||
|
| ||
| 3. Workflow | Positive |
|
|
| Negative |
|
| |
| Suggestions |
|
| |
|
| ||
|
| ||
| 4. Content | Positive |
|
|
|
| ||
|
| ||
|
| ||
| Negative |
|
| |
|
| ||
|
| ||
|
| ||
|
| ||
|
| ||
| Suggestions |
|
| |
|
| ||
|
| ||
| 5. Understandability | Positive |
|
|
|
| ||
| Negative |
|
| |
|
| ||
|
| ||
|
| ||
|
| ||
| Suggestions |
|
| |
|
| ||
| 6. Medical usefulness | Positive |
|
|
|
| ||
|
| ||
| Negative |
|
| |
| Suggestions |
|
| |
|
| ||
| 7. Navigation | Positive |
|
|
| Negative |
|
| |
|
| ||
|
| ||
| Suggestions |
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Elchynski, A.L.; Desai, N.; D’Silva, D.; Hall, B.; Marks, Y.; Wiisanen, K.; Cicali, E.J.; Cavallari, L.H.; Nguyen, K.A. Utilizing a Human–Computer Interaction Approach to Evaluate the Design of Current Pharmacogenomics Clinical Decision Support. J. Pers. Med. 2021, 11, 1227. https://doi.org/10.3390/jpm11111227
Elchynski AL, Desai N, D’Silva D, Hall B, Marks Y, Wiisanen K, Cicali EJ, Cavallari LH, Nguyen KA. Utilizing a Human–Computer Interaction Approach to Evaluate the Design of Current Pharmacogenomics Clinical Decision Support. Journal of Personalized Medicine. 2021; 11(11):1227. https://doi.org/10.3390/jpm11111227
Chicago/Turabian StyleElchynski, Amanda L., Nina Desai, Danielle D’Silva, Bradley Hall, Yael Marks, Kristin Wiisanen, Emily J. Cicali, Larisa H. Cavallari, and Khoa A. Nguyen. 2021. "Utilizing a Human–Computer Interaction Approach to Evaluate the Design of Current Pharmacogenomics Clinical Decision Support" Journal of Personalized Medicine 11, no. 11: 1227. https://doi.org/10.3390/jpm11111227