
Unclear Insomnia Concept in Randomized Controlled Trials and Systematic Reviews: A Meta-Epidemiological Study

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Types of Studies Included
2.3. Search Methods
2.4. Study Selection and Data Extraction
2.5. Statistical Analysis
2.6. Differences between the Protocol and the Article
2.7. Ethics
3. Results
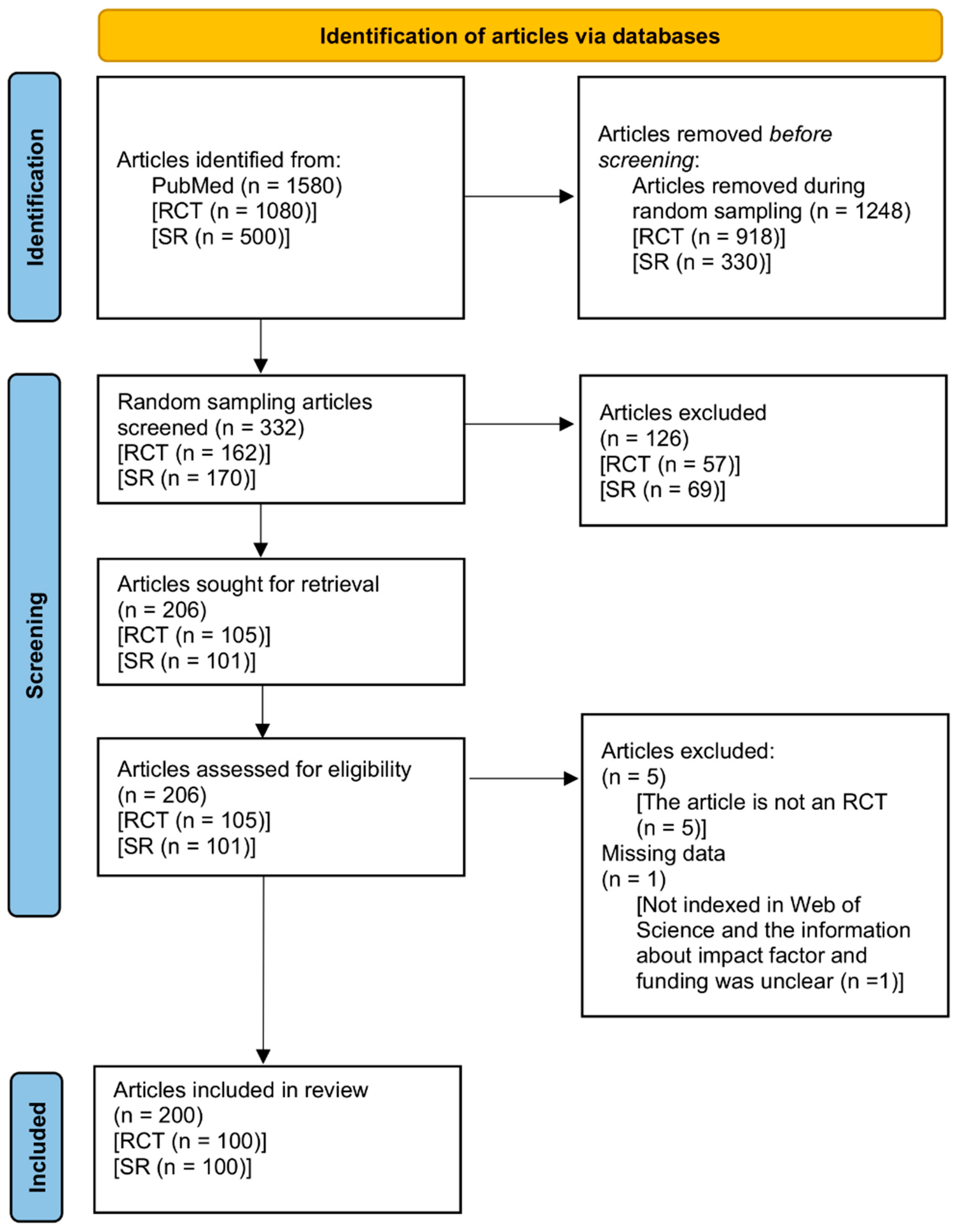
3.1. Selection Process
3.2. Proportions and Trends of RCT and SR Abstracts in Which Insomnia Concept Was Unclear
3.3. The Percentage of Unclear Insomnia Concept of RCT and SR Abstracts If We Consider What Was Stated in the Full Text
3.4. Characteristics of RCT and SR Abstracts with Unclear Insomnia Concept, and the Relationship between the Characteristics and Unclear Definitions in Abstracts
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Glasziou, P.; Meats, E.; Heneghan, C.; Shepperd, S. What is missing from descriptions of treatment in trials and reviews? BMJ 2008, 336, 1472–1474. [Google Scholar] [CrossRef] [PubMed]
- Chalmers, I.; Glasziou, P. Avoidable waste in the production and reporting of research evidence. Lancet 2009, 374, 86–89. [Google Scholar] [CrossRef]
- Hua, F.; Sun, Q.; Zhao, T.; Chen, X.; He, H. Reporting quality of randomised controlled trial abstracts presented at the SLEEP Annual Meetings: A cross-sectional study. BMJ Open 2019, 9, e029270. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; Shamseer, L.; Altman, D.G.; Tetzlaff, J.; Sampson, M.; Tricco, A.C.; Catala-Lopez, F.; Li, L.; Reid, E.K.; Sarkis-Onofre, R.; et al. Epidemiology and Reporting Characteristics of Systematic Reviews of Biomedical Research: A Cross-Sectional Study. PLoS Med. 2016, 13, e1002028. [Google Scholar] [CrossRef] [PubMed]
- Ho, F.Y.; Choi, W.T.; Yeung, W.F.; Lam, H.K.; Lau, W.Y.; Chung, K.F. The efficacy of integrated cognitive behavioral therapy (CBT) and acupressure versus CBT for insomnia: A three-arm pilot randomized controlled trial. Sleep Med. 2021, 87, 158–167. [Google Scholar] [CrossRef] [PubMed]
- Yardley, J.; Karppa, M.; Inoue, Y.; Pinner, K.; Perdomo, C.; Ishikawa, K.; Filippov, G.; Kubota, N.; Moline, M. Long-term effectiveness and safety of lemborexant in adults with insomnia disorder: Results from a phase 3 randomized clinical trial. Sleep Med. 2021, 80, 333–342. [Google Scholar] [CrossRef] [PubMed]
- Morin, C.M.; Drake, C.L.; Harvey, A.G.; Krystal, A.D.; Manber, R.; Riemann, D.; Spiegelhalder, K. Insomnia disorder. Nat. Rev. Dis. Primers 2015, 1, 15026. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition: DSM-5; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- American Academy of Sleep Medicine. International Classification of Sleep Disorders, 3rd ed.; American Academy of Sleep Medicine: Darien, IL, USA, 2014. [Google Scholar]
- World Health Organization. ICD-10: International Statistical Classification of Diseases and Related Health Problems: Tenth Revision, 2nd ed.; World Health Organization: Geneva, Switzerland, 2004. [Google Scholar]
- Chung, K.F.; Yeung, W.F.; Ho, F.Y.; Yung, K.P.; Yu, Y.M.; Kwok, C.W. Cross-cultural and comparative epidemiology of insomnia: The Diagnostic and statistical manual (DSM), International classification of diseases (ICD) and International classification of sleep disorders (ICSD). Sleep Med. 2015, 16, 477–482. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Qin, Z.; So, T.H.; Chen, H.; Lam, W.L.; Yam, L.L.; Yan Chan, P.; Lao, L.; Zhang, Z.J. Electroacupuncture Plus Auricular Acupressure for Chemotherapy-Associated Insomnia in Breast Cancer Patients: A Pilot Randomized Controlled Trial. Integr. Cancer Ther. 2021, 20, 15347354211019103. [Google Scholar] [CrossRef] [PubMed]
- Vestergaard, C.L.; Vedaa, O.; Simpson, M.R.; Faaland, P.; Vethe, D.; Kjorstad, K.; Langsrud, K.; Ritterband, L.M.; Sivertsen, B.; Stiles, T.C.; et al. The effect of sleep-wake intraindividual variability in digital cognitive behavioral therapy for insomnia: A mediation analysis of a large-scale RCT. Sleep 2021, 44, zsab118. [Google Scholar] [CrossRef] [PubMed]
- Liou, K.T.; Garland, S.N.; Li, Q.S.; Sadeghi, K.; Green, J.; Autuori, I.; Orlow, I.; Mao, J.J. Effects of acupuncture versus cognitive behavioral therapy on brain-derived neurotrophic factor in cancer survivors with insomnia: An exploratory analysis. Acupunct Med. 2021, 39, 637–645. [Google Scholar] [CrossRef] [PubMed]
- Xiao, K.; Gillissie, E.S.; Lui, L.M.W.; Ceban, F.; Teopiz, K.M.; Gill, H.; Cao, B.; Ho, R.; Rosenblat, J.D.; McIntyre, R.S. Immune Response to Vaccination in Adults with Mental Disorders: A Systematic Review. J. Affect. Disord. 2022. [Google Scholar] [CrossRef] [PubMed]
- Evans, K.; Rennick-Egglestone, S.; Cox, S.; Kuipers, Y.; Spiby, H. Remotely Delivered Interventions to Support Women With Symptoms of Anxiety in Pregnancy: Mixed Methods Systematic Review and Meta-analysis. J. Med. Internet Res. 2022, 24, e28093. [Google Scholar] [CrossRef] [PubMed]
- Sharafkhaneh, A.; Salari, N.; Khazaie, S.; Ghasemi, H.; Darvishi, N.; Hosseinian-Far, A.; Mohammadi, M.; Khazaie, H. Telemedicine and insomnia: A comprehensive systematic review and meta-analysis. Sleep Med. 2022, 90, 117–130. [Google Scholar] [CrossRef] [PubMed]
- Chutiyami, M.; Cheong, A.M.Y.; Salihu, D.; Bello, U.M.; Ndwiga, D.; Maharaj, R.; Naidoo, K.; Kolo, M.A.; Jacob, P.; Chhina, N.; et al. COVID-19 Pandemic and Overall Mental Health of Healthcare Professionals Globally: A Meta-Review of Systematic Reviews. Front. Psychiatry 2021, 12, 804525. [Google Scholar] [CrossRef] [PubMed]
- Banno, M.; Tsujimoto, Y.; Kohmura; Dohi, E.; Taito, S.; Someko, H.; Kataoka, Y. Unclear insomnia types in randomized controlled trials and systematic reviews: The protocol for a meta-epidemiological study. protocols.io 2022. [Google Scholar] [CrossRef]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef]
- Rombey, T.; Lochner, V.; Puljak, L.; Konsgen, N.; Mathes, T.; Pieper, D. Epidemiology and reporting characteristics of non-Cochrane updates of systematic reviews: A cross-sectional study. Res. Synth Methods 2020, 11, 471–483. [Google Scholar] [CrossRef] [PubMed]
- Banno, M.; Tsujimoto, Y.; Kataoka, Y. The majority of reporting guidelines are not developed with the Delphi method: A systematic review of reporting guidelines. J. Clin. Epidemiol. 2020, 124, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Bigna, J.J.; Um, L.N.; Nansseu, J.R. A comparison of quality of abstracts of systematic reviews including meta-analysis of randomized controlled trials in high-impact general medicine journals before and after the publication of PRISMA extension for abstracts: A systematic review and meta-analysis. Syst. Rev. 2016, 5, 174. [Google Scholar] [CrossRef] [Green Version]
- Firth, D. Bias reduction of maximum likelihood estimates. Biometrika 1993, 80, 27–38. [Google Scholar] [CrossRef]
- Heinze, G.; Schemper, M. A solution to the problem of separation in logistic regression. Stat. Med. 2002, 21, 2409–2419. [Google Scholar] [CrossRef] [PubMed]
- Rubin, M. Do p Values Lose Their Meaning in Exploratory Analyses? It Depends How You Define the Familywise Error Rate. Rev. Gen. Psychol. 2017, 21, 269–275. [Google Scholar] [CrossRef]
- StataCorp. Stata Statistical Software: Release 15; StataCorp LLC: College Station, TX, USA, 2017. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Category | Subcategory | RCT n = 88 | SR n = 94 |
|---|---|---|---|
| Intended insomnia concept | Unclear insomnia concept | 24 (27) | 54 (57) |
| Insomnia disorder | 5 (6) | 12 (13) | |
| Insomnia symptoms | 43 (49) | 23 (24) | |
| Both insomnia disorder and insomnia symptoms | 16 (18) | 5 (5) |
| Category | Subcategory | RCTs | SRs | ||
|---|---|---|---|---|---|
| Unclear Insomnia Concept n = 88 | Clear Insomnia Concept n = 12 | Unclear Insomnia Concept n = 94 | Clear Insomnia Concept n = 6 | ||
| Impact Factor | 0 to 4 | 58 (66) | 10 (83) | 46 (49) | 4 (67) |
| 5 to 9 | 17 (19) | 1 (8) | 35 (37) | 1 (17) | |
| 10 or more | 8 (9) | 1 (8) | 4 (4) | 1 (17) | |
| No value | 5 (6) | 0 (0) | 9 (10) | 0 (0) | |
| Word counts in abstracts | median 270 (IQR 244 to 311) | median 288 (IQR 272 to 298) | median 279 (IQR 237 to 387) | median 246 (IQR 241 to 257) | |
| Word limitations in abstracts | Less than 300 | 64 (73) | 9 (75) | 39 (41) | 4 (67) |
| 300 or more | 20 (23) | 2 (17) | 43 (46) | 1 (17) | |
| Unclear | 4 (5) | 1 (8) | 12 (13) | 1 (17) | |
| Funding | None | 12 (14) | 1 (8) | 53 (56) | 3 (50) |
| Industry | 29 (33) | 5 (42) | 3 (3) | 0 (0) | |
| Non-industry | 47 (53) | 6 (50) | 38 (40) | 3 (50) | |
| Compliance with reporting guidelines | No compliance | 77 (88) | 12 (100) | 46 (49) | 3 (50) |
| Compliance | 11 (13) | 0 (0) | 48 (51) | 3 (50) | |
| Registrations or protocols | No registrations/protocols | 21 (24) | 4 (33) | 63 (67) | 6 (100) |
| Registrations/protocols | 67 (76) | 8 (67) | 31 (33) | 0 (0) | |
| Journal names that included sleep | Non-sleep journal | 68 (77) | 9 (75) | 90 (96) | 5 (83) |
| Sleep journal | 20 (23) | 3 (25) | 4 (4) | 1 (17) | |
| Category | Subcategory | RCTs (n = 100) | SRs (n = 100) | ||
|---|---|---|---|---|---|
| Crude OR (95% CI) | AOR (95% CI) | Crude OR (95% CI) | AOR (95% CI) | ||
| Impact factor | 0 to 4 | Ref | Ref | Ref | Ref |
| 5 to 9 | 2.09 (0.35, 12.57) | 1.97 (0.33, 11.81) | 2.29 (0.34, 15.29) | 1.69 (0.23, 12.55) | |
| 10 or more | 1.02 (0.16, 6.51) | 1.43 (0.14, 14.26) | 0.29 (0.04, 2.34) | 0.50 (0.05, 4.99) | |
| No value | 1.97 (0.10, 38.43) | 4.09 (0.11, 149.78) | 1.84 (0.09, 37.08) | 4.22 (0.15, 121.40) | |
| Word counts in abstracts | 1.00 (0.99, 1.01) | 1.00 (0.99, 1.01) | 1.00 (0.99, 1.01) | 1.00 (1.00, 1.01) | |
| Word limitations in abstracts | Less than 300 | Ref | Ref | Ref | Ref |
| 300 or more | 1.21 (0.28, 5.30) | 1.44 (0.28, 7.42) | 3.30 (0.50, 22.03) | 2.18 (0.28, 16.92) | |
| Unclear | 0.44 (0.06, 3.17) | 0.31 (0.03, 3.44) | 0.95 (0.13, 6.70) | 0.63 (0.07, 5.44) | |
| Funding | None | Ref | Ref | Ref | Ref |
| Industry | 0.64 (0.09, 4.40) | 0.71 (0.10, 5.33) | 0.46 (0.02, 10.73) | 0.77 (0.03, 22.63) | |
| Non-industry | 0.88 (0.13, 5.76) | 0.79 (0.11, 5.90) | 0.72 (0.15, 3.35) | 0.79 (0.17, 3.64) | |
| Compliance with reporting guidelines | No compliance | Ref | Ref | Ref | Ref |
| Compliance | 3.71 (0.21, 67.00) | 3.05 (0.16, 57.19) | 1.04 (0.22, 4.84) | 0.87 (0.19, 4.02) | |
| Registrations or protocols | No registrations/protocols | Ref | Ref | Ref | Ref |
| Registrations/protocols | 1.66 (0.48, 5.75) | 1.60 (0.40, 6.35) | 6.45 (0.35, 118.14) | 6.40 (0.36, 114.28) | |
| Journal names that included sleep | Non-sleep journal | Ref | Ref | Ref | Ref |
| Sleep journal | 0.81 (0.22, 3.04) | 0.77 (0.18, 3.30) | 0.18 (0.02, 1.40) | 0.38 (0.03, 4.42) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Banno, M.; Tsujimoto, Y.; Kohmura, K.; Dohi, E.; Taito, S.; Someko, H.; Kataoka, Y. Unclear Insomnia Concept in Randomized Controlled Trials and Systematic Reviews: A Meta-Epidemiological Study. Int. J. Environ. Res. Public Health 2022, 19, 12261. https://doi.org/10.3390/ijerph191912261
Banno M, Tsujimoto Y, Kohmura K, Dohi E, Taito S, Someko H, Kataoka Y. Unclear Insomnia Concept in Randomized Controlled Trials and Systematic Reviews: A Meta-Epidemiological Study. International Journal of Environmental Research and Public Health. 2022; 19(19):12261. https://doi.org/10.3390/ijerph191912261
Chicago/Turabian StyleBanno, Masahiro, Yasushi Tsujimoto, Kunihiro Kohmura, Eisuke Dohi, Shunsuke Taito, Hidehiro Someko, and Yuki Kataoka. 2022. "Unclear Insomnia Concept in Randomized Controlled Trials and Systematic Reviews: A Meta-Epidemiological Study" International Journal of Environmental Research and Public Health 19, no. 19: 12261. https://doi.org/10.3390/ijerph191912261