Night Shift Work, Chronotype, Sleep Duration, and Prostate Cancer Risk: CAPLIFE Study

 , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
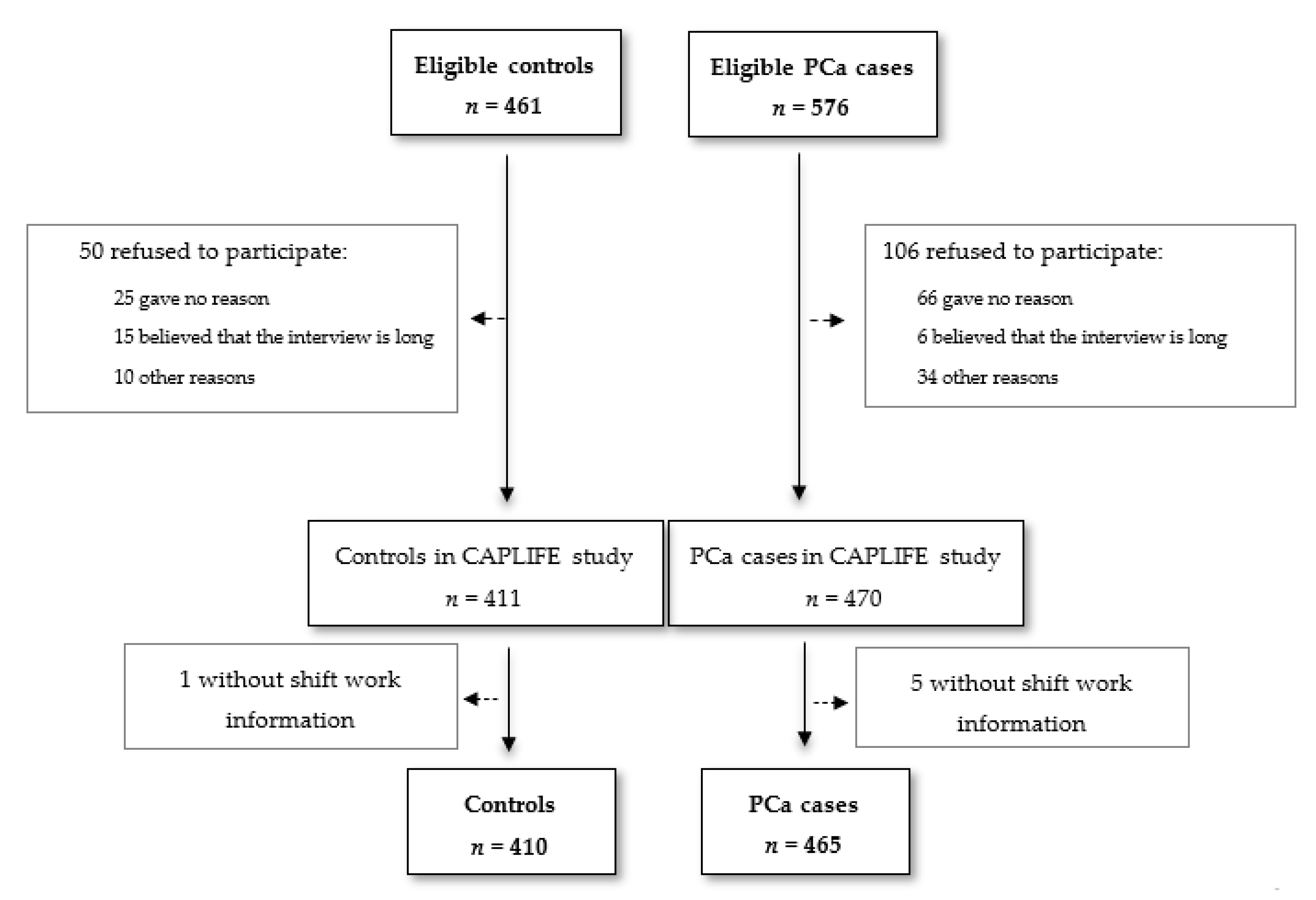
2.1. Study Design and Setting
2.2. Participants
2.3. Data Collection
2.4. Night Shift Work
2.5. Chronotype
2.6. Sleeps Duration
2.7. Measurement of Tumor Aggressiveness
2.8. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Rawla, P. Epidemiology of Prostate Cancer. World J. Oncol. 2019, 10, 63–89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, M.C.S.; Goggins, W.B.; Wang, H.H.X.; Fung, F.D.H.; Leung, C.; Wong, S.Y.S.; Ng, C.F.; Sung, J.J.Y. Global Incidence and Mortality for Prostate Cancer: Analysis of Temporal Patterns and Trends in 36 Countries. Eur. Urol. 2016, 70, 862–874. [Google Scholar] [CrossRef] [Green Version]
- SEOM. Estimaciones de la incidencia del cáncer en España, 2020; Red Española de Registros de Cáncer: Madrid, Spain, 2020; pp. 1–21. [Google Scholar]
- Eeles, R.A.; Olama, A.A.A.; Benlloch, S.; Saunders, E.J.; Leongamornlert, D.A.; Tymrakiewicz, M.; Ghoussaini, M.; Luccarini, C.; Dennis, J.; Jugurnauth-Little, S.; et al. Identification of 23 new prostate cancer susceptibility loci using the iCOGS custom genotyping array. Nat. Genet. 2013, 45, 385–391. [Google Scholar] [CrossRef] [PubMed]
- Tan, S.-H.; Petrovics, G.; Srivastava, S. Prostate Cancer Genomics: Recent Advances and the Prevailing Underrepresentation from Racial and Ethnic Minorities. Int. J. Mol. Sci. 2018, 19, 1255. [Google Scholar] [CrossRef] [Green Version]
- Chen, H.; Yu, H.; Wang, J.; Zhang, Z.; Gao, Z.; Chen, Z.; Lu, Y.; Liu, W.; Jiang, D.; Zheng, S.L.; et al. Systematic enrichment analysis of potentially functional regions for 103 prostate cancer risk-associated loci. Prostate 2015, 75, 1264–1276. [Google Scholar] [CrossRef]
- Cooperberg, M.R.; Chan, J.M. Epidemiology of prostate cancer. World J. Urol. 2017, 35, 849. [Google Scholar] [CrossRef] [Green Version]
- Agents Classified by the IARC Monographs, Volumes 1–125—IARC Monographs on the Identification of Carcinogenic Hazards to Humans. Available online: https://monographs.iarc.fr/agents-classified-by-the-iarc/ (accessed on 2 April 2020).
- Eriksen, K.T.; Halkjaer, J.; Meliker, J.R.; McElroy, J.A.; Sorensen, M.; Tjonneland, A.; Raaschou-Nielsen, O. Dietary cadmium intake and risk of prostate cancer: A Danish prospective cohort study. BMC Cancer 2015, 15, 177. [Google Scholar] [CrossRef] [Green Version]
- Roh, T.; Lynch, C.F.; Weyer, P.; Wang, K.; Kelly, K.M.; Ludewig, G. Low-level arsenic exposure from drinking water is associated with prostate cancer in Iowa. Environ. Res. 2017, 159, 338–343. [Google Scholar] [CrossRef] [PubMed]
- Diallo, A.; Deschasaux, M.; Latino-Martel, P.; Hercberg, S.; Galan, P.; Fassier, P.; Alles, B.; Gueraud, F.; Pierre, F.H.; Touvier, M. Red and processed meat intake and cancer risk: Results from the prospective NutriNet-Sante cohort study. Int. J. Cancer 2018, 142, 230–237. [Google Scholar] [CrossRef] [PubMed]
- Papantoniou, K.; Castano-Vinyals, G.; Espinosa, A.; Aragones, N.; Perez-Gomez, B.; Burgos, J.; Gomez-Acebo, I.; Llorca, J.; Peiro, R.; Jimenez-Moleon, J.J.; et al. Night shift work, chronotype and prostate cancer risk in the MCC-Spain case-control study. Int. J. Cancer 2015, 137, 1147–1157. [Google Scholar] [CrossRef] [PubMed]
- Diet, Nutrition, Physical Activity and Cancer: A Global Perspective. Available online: https://www.wcrf.org/dietandcancer (accessed on 5 May 2020).
- Do you work shifts? (Working time) visualisation: European Map by: Age, All, Answer: No—European Working Conditions Survey—Data visualisation EWCS2016. Available online: https://www.eurofound.europa.eu/data/european-working-conditions-survey (accessed on 2 April 2020).
- Careers for night owls and early birds: Career Outlook: U.S. Bureau of Labor Statistics. Available online: https://www.bls.gov/careeroutlook/2015/article/night-owls-and-early-birds.htm (accessed on 6 April 2020).
- Vetter, C. Circadian disruption: What do we actually mean? Eur. J. Neurosci. 2018, 51, 531–550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vitale, J.A.; Lombardi, G.; Weydahl, A.; Banfi, G. Biological rhythms, chronodisruption and chrono-enhancement: The role of physical activity as synchronizer in correcting steroids circadian rhythm in metabolic dysfunctions and cancer. Chronobiol. Int. 2018, 35, 1185–1197. [Google Scholar] [CrossRef] [PubMed]
- Shostak, A. Circadian Clock, Cell Division, and Cancer: From Molecules to Organism. Int. J. Mol. Sci. 2017, 18, 873. [Google Scholar] [CrossRef]
- Hunter, C.M.; Figueiro, M.G. Measuring Light at Night and Melatonin Levels in Shift Workers: A Review of the Literature. Biol. Res. Nurs. 2017, 19, 365–374. [Google Scholar] [CrossRef]
- IARC Monographs Vol 124 Group. Carcinogenicity of night shift work. Lancet Oncol. 2019, 20, 1058–1059. [Google Scholar] [CrossRef]
- IARC International Agency for Research on Cancer. Painting, Firefighting, and Shiftwork; International Agency for Research on Cancer: Lyon, France, 2010; ISBN 9789283212980. [Google Scholar]
- Stevens, R.G.; Hansen, J.; Costa, G.; Haus, E.; Kauppinen, T.; Aronson, K.J.; Castano-Vinyals, G.; Davis, S.; Frings-Dresen, M.H.W.; Fritschi, L.; et al. Considerations of circadian impact for defining “shift work” in cancer studies: IARC Working Group Report. Occup. Environ. Med. 2011, 68, 154–162. [Google Scholar] [CrossRef]
- Tse, L.A.; Lee, P.M.Y.; Ho, W.M.; Lam, A.T.; Lee, M.K.; Ng, S.S.M.; He, Y.; Leung, K.S.; Hartle, J.C.; Hu, H.; et al. Bisphenol A and other environmental risk factors for prostate cancer in Hong Kong. Environ. Int. 2017, 107, 1–7. [Google Scholar] [CrossRef]
- Behrens, T.; Rabstein, S.; Wichert, K.; Erbel, R.; Eisele, L.; Arendt, M.; Dragano, N.; Brüning, T.; Jöckel, K.H. Shift work and the incidence of prostate cancer: A 10-year follow-up of a German population-based cohort study. Scand. J. Work. Environ. Heal. 2017, 43, 560–568. [Google Scholar] [CrossRef] [Green Version]
- Åkerstedt, T.; Narusyte, J.; Svedberg, P.; Kecklund, G.; Alexanderson, K. Night work and prostate cancer in men: A Swedish prospective cohort study. BMJ Open 2017, 7, e015751. [Google Scholar] [CrossRef]
- Dickerman, B.A.; Markt, S.C.; Koskenvuo, M.; Hublin, C.; Pukkala, E.; Mucci, L.A.; Kaprio, J. Sleep disruption, chronotype, shift work, and prostate cancer risk and mortality: A 30-year prospective cohort study of Finnish twins. Cancer Causes Control 2016, 27, 1361–1370. [Google Scholar] [CrossRef] [PubMed]
- Barul, C.; Richard, H.; Parent, M.-E. Night-Shift Work and Risk of Prostate Cancer: Results From a Canadian Case-Control Study, the Prostate Cancer and Environment Study. Am. J. Epidemiol. 2019, 188, 1801–1811. [Google Scholar] [CrossRef] [PubMed]
- Wendeu-Foyet, M.G.; Bayon, V.; Cénée, S.; Trétarre, B.; Rébillard, X.; Cancel-Tassin, G.; Cussenot, O.; Lamy, P.-J.; Faraut, B.; Ben Khedher, S.; et al. Night work and prostate cancer risk: Results from the EPICAP Study. Occup. Environ. Med. 2018, 75, 573–581. [Google Scholar] [CrossRef] [PubMed]
- Erren, T.C.; Morfeld, P.; Groß, J.V.; Wild, U.; Lewis, P. IARC 2019: “Night shift work” is probably carcinogenic: What about disturbed chronobiology in all walks of life? J. Occup. Med. Toxicol. 2019, 14, 29. [Google Scholar] [CrossRef]
- Vanttola, P.; Puttonen, S.; Karhula, K.; Oksanen, T.; Härmä, M. Employees with shift work disorder experience excessive sleepiness also on non-work days: A cross-sectional survey linked to working hours register in Finnish hospitals. Ind. Health 2020, 58, 366–374. [Google Scholar] [CrossRef] [Green Version]
- Brum, M.C.B.; Dantas Filho, F.F.; Schnorr, C.C.; Bertoletti, O.A.; Bottega, G.B.; Da Costa Rodrigues, T. Night shift work, short sleep and obesity. Diabetol. Metab. Syndr. 2020, 12, 13. [Google Scholar] [CrossRef] [Green Version]
- Cao, J.; Eshak, E.S.; Liu, K.; Muraki, I.; Cui, R.; Iso, H.; Tamakoshi, A. Sleep duration and risk of breast cancer: The JACC Study. Breast Cancer Res. Treat. 2019, 174, 219–225. [Google Scholar] [CrossRef]
- Shen, J.; Chrisman, M.; Wu, X.; Chow, W.-H.; Zhao, H. Sleep duration and risk of cancer in the Mexican American Mano-a-Mano Cohort. Sleep Heal. 2019, 5, 78–83. [Google Scholar] [CrossRef]
- Fritschi, L.; Glass, D.C.; Heyworth, J.S.; Aronson, K.; Girschik, J.; Boyle, T.; Grundy, A.; Erren, T.C. Hypotheses for mechanisms linking shiftwork and cancer. Med. Hypotheses 2011, 77, 430–436. [Google Scholar] [CrossRef]
- Markt, S.C.; Grotta, A.; Nyren, O.; Adami, H.-O.; Mucci, L.A.; Valdimarsdottir, U.A.; Stattin, P.; Bellocco, R.; Lagerros, Y.T. Insufficient Sleep and Risk of Prostate Cancer in a Large Swedish Cohort. Sleep 2015, 38, 1405–1410. [Google Scholar] [CrossRef]
- Horne, J.A.; Östberg, O. Individual differences in human circadian rhythms. Biol. Psychol. 1977, 5, 179–190. [Google Scholar] [CrossRef]
- Bonaconsa, M.; Malpeli, G.; Montaruli, A.; Carandente, F.; Grassi-Zucconi, G.; Bentivoglio, M. Differential modulation of clock gene expression in the suprachiasmatic nucleus, liver and heart of aged mice. Exp. Gerontol. 2014, 55, 70–79. [Google Scholar] [CrossRef] [PubMed]
- Adan, A.; Archer, S.N.; Hidalgo, M.P.; Di Milia, L.; Natale, V.; Randler, C. Circadian typology: A comprehensive review. Chronobiol. Int. 2012, 29, 1153–1175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hurley, S.; Goldberg, D.; Von Behren, J.; Clague DeHart, J.; Wang, S.; Reynolds, P. Chronotype and postmenopausal breast cancer risk among women in the California Teachers Study. Chronobiol. Int. 2019, 36, 1504–1514. [Google Scholar] [CrossRef] [PubMed]
- Morfeld, P.; Erren, T.C. Shift work, chronotype, and cancer risk-letter. Cancer Epidemiol. Biomark. Prev. 2019, 28, 1404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Razavi, P.; Devore, E.E.; Bajaj, A.; Lockley, S.W.; Figueiro, M.G.; Ricchiuti, V.; Gauderman, W.J.; Hankinson, S.E.; Willett, W.C.; Schernhammer, E.S. Shift Work, Chronotype, and Melatonin Rhythm in Nurses. Cancer Epidemiol. Biomark. Prev. 2019, 28, 1177–1186. [Google Scholar] [CrossRef]
- Olmedo-Requena, R.; Lozano-Lorca, M.; Salcedo-Bellido, I.; Jimenez-Pacheco, A.; Vazquez-Alonso, F.; Garcia-Caballos, M.; Sanchez, M.-J.; Jimenez-Moleon, J.-J. Compliance with the 2018 World Cancer Research Fund/American Institute for Cancer Research Cancer Prevention Recommendations and Prostate Cancer. Nutrients 2020, 12, 768. [Google Scholar]
- Versión ICD-10: 2016. Available online: https://icd.who.int/browse10/2016/en (accessed on 20 January 2020).
- Román Viñas, B.; Ribas Barba, L.; Ngo, J.; Serra Majem, L. Validación en población catalana del cuestionario internacional de actividad física. Gac. Sanit. 2013, 27, 254–257. [Google Scholar] [CrossRef] [Green Version]
- Real Decreto Legislativo 2/2015, de 23 de octubre, por el que se aprueba el texto refundido de la Ley del Estatuto de los Trabajadores Núm Disposición 11430 del BOE núm. 255 de 2015. Available online: https://www.boe.es/buscar/pdf/2015/BOE-A-2015-11430-consolidado.pdf (accessed on 28 July 2020).
- Roenneberg, T.; Wirz-Justice, A.; Merrow, M. Life between clocks: Daily temporal patterns of human chronotypes. J. Biol. Rhythms 2003, 18, 80–90. [Google Scholar] [CrossRef] [Green Version]
- Roenneberg, T.; Kuehnle, T.; Juda, M.; Kantermann, T.; Allebrandt, K.; Gordijn, M.; Merrow, M. Epidemiology of the human circadian clock. Sleep Med. Rev. 2007, 11, 429–438. [Google Scholar] [CrossRef] [Green Version]
- Pilz, L.K.; Carissimi, A.; Oliveira, M.A.B.; Francisco, A.P.; Fabris, R.C.; Medeiros, M.S.; Scop, M.; Frey, B.N.; Adan, A.; Hidalgo, M.P. Rhythmicity of Mood Symptoms in Individuals at Risk for Psychiatric Disorders. Sci. Rep. 2018, 8, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Papantoniou, K.; Castano-Vinyals, G.; Espinosa, A.; Aragones, N.; Perez-Gomez, B.; Ardanaz, E.; Altzibar, J.M.; Sanchez, V.M.; Gomez-Acebo, I.; Llorca, J.; et al. Breast cancer risk and night shift work in a case-control study in a Spanish population. Eur. J. Epidemiol. 2016, 31, 867–878. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papantoniou, K.; Castaño-Vinyals, G.; Espinosa, A.; Turner, M.C.; Alonso-Aguado, M.H.; Martin, V.; Aragonés, N.; Pérez-Gómez, B.; Pozo, B.M.; Gómez-Acebo, I.; et al. Shift work and colorectal cancer risk in the MCC-Spain case–control study. Scand. J. Work. Environ. Health 2017, 43, 250–259. [Google Scholar] [CrossRef] [Green Version]
- Hirshkowitz, M.; Whiton, K.; Albert, S.M.; Alessi, C.; Bruni, O.; DonCarlos, L.; Hazen, N.; Herman, J.; Katz, E.S.; Kheirandish-Gozal, L.; et al. National sleep foundation’s sleep time duration recommendations: Methodology and results summary. Sleep Health 2015, 1, 40–43. [Google Scholar] [CrossRef] [PubMed]
- Epstein, J.I.; Egevad, L.; Amin, M.B.; Delahunt, B.; Srigley, J.R.; Humphrey, P.A. The 2014 International Society of Urological Pathology (ISUP) Consensus Conference on Gleason Grading of Prostatic Carcinoma: Definition of Grading Patterns and Proposal for a New Grading System. Am. J. Surg. Pathol. 2016, 40, 244–252. [Google Scholar] [CrossRef] [PubMed]
- Neuzillet, Y.; Raynaud, J.-P.; Dreyfus, J.-F.; Radulescu, C.; Rouanne, M.; Schneider, M.; Krish, S.; Roupret, M.; Drouin, S.J.; Comperat, E.; et al. Aggressiveness of Localized Prostate Cancer: The Key Value of Testosterone Deficiency Evaluated by Both Total and Bioavailable Testosterone: AndroCan Study Results. Horm. Cancer 2019, 10, 36–44. [Google Scholar] [CrossRef]
- Kogevinas, M.; Espinosa, A.; Papantoniou, K.; Aragonés, N.; Pérez-Gómez, B.; Burgos, J.; Gómez-Acebo, I.; Llorca, J.; Peiró, R.; Jimenez-Moleón, J.J.; et al. Prostate cancer risk decreases following cessation of night shift work. Int. J. Cancer 2019, 145, 2597–2599. [Google Scholar] [CrossRef]
- Martin, J.S.; Laberge, L.; Sasseville, A.; Berube, M.; Alain, S.; Houle, J.; Hebert, M. Day and night shift schedules are associated with lower sleep quality in Evening-types. Chronobiol. Int. 2015, 32, 627–636. [Google Scholar] [CrossRef]
- Schuster, M.; Oberlinner, C.; Claus, M. Shift-specific associations between age, chronotype and sleep duration. Chronobiol. Int. 2019, 36, 784–795. [Google Scholar] [CrossRef]
- Ritonja, J.; Tranmer, J.; Aronson, K.J. The relationship between night work, chronotype, and cardiometabolic risk factors in female hospital employees. Chronobiol. Int. 2019, 36, 616–628. [Google Scholar] [CrossRef]
- Markt, S.C.; Flynn-Evans, E.E.; Valdimarsdottir, U.A.; Sigurdardottir, L.G.; Tamimi, R.M.; Batista, J.L.; Haneuse, S.; Lockley, S.W.; Stampfer, M.; Wilson, K.M.; et al. Sleep Duration and Disruption and Prostate Cancer Risk: A 23-Year Prospective Study. Cancer Epidemiol. Biomark. Prev. 2016, 25, 302–308. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Controls | PCa Cases | ||||||
|---|---|---|---|---|---|---|---|
| Never Night Shift N = 344 | Ever Night Shift N = 66 | Total N = 410 | Never Night Shift N=368 | Ever Night Shift N = 97 | Total N = 465 | P-Value a | |
| Age (Years), Mean (SD) | 66.5 (7.7) | 63.2 (8.4) | 65.6 (7.9) | 67.4 (7.5) | 68.4 (7.6) | 67.7 (7.5) | 0.001 |
| P-Value b | 0.002 | 0.244 | |||||
| Age (Years), N (%) | 0.039 | ||||||
| 40–54 | 28 (8.1) | 14 (21.2) | 42 (10.2) | 24 (6.5) | 4 (4.1) | 28 (6.0) | |
| 55–69 | 182 (52.9) | 41 (62.1) | 223 (54.4) | 198 (53.8) | 50 (51.6) | 248 (53.3) | |
| 70–80 | 134 (39.0) | 11 (16.7) | 145 (35.4) | 146 (39.7) | 43 (44.3) | 189 (40.7) | |
| P-Value b | <0.001 | 0.544 | |||||
| Education, N (%) | 0.357 | ||||||
| Primary | 100 (29.1) | 19 (28.8) | 119 (29.0) | 108 (29.3) | 36 (37.1) | 144 (31.0) | |
| Secondary | 178 (51.7) | 26 (39.4) | 204 (49.8) | 189 (51.4) | 51 (52.6) | 240 (51.6) | |
| University | 66 (19.2) | 21 (31.8) | 87 (21.2) | 71 (19.3) | 10 (10.3) | 81 (17.4) | |
| P-Value b | 0.053 | 0.079 | |||||
| BMI, Mean (SD) | 28.4 (3.9) | 28.9 (4.6) | 28.5 (4.0) | 28.2 (4.1) | 28.0 (3.6) | 28.2 (4.0) | 0.252 |
| P-Value b | 0.400 | 0.598 | |||||
| BMI, N (%) | 0.569 | ||||||
| Normal weight (<25 Kg/m2) | 65 (18.9) | 8 (12.1) | 73 (17.8) | 75 (20.4) | 21 (21.6) | 96 (20.6) | |
| Overweight (25–29.9 Kg/m2) | 179 (52.0) | 38 (57.6) | 217 (52.9) | 184 (50.0) | 54 (55.7) | 238 (51.2) | |
| Obesity (≥30 Kg/m2) | 100 (29.1) | 20 (30.3) | 120 (29.3) | 109 (29.6) | 22 (22.7) | 131 (28.2) | |
| P-Value b | 0.411 | 0.396 | |||||
| Smoking Status, N (%) | 0.781 | ||||||
| Never | 89 (25.9) | 19 (28.8) | 108 (26.3) | 95 (25.8) | 23 (23.7) | 118 (25.4) | |
| Former | 189 (54.9) | 36 (54.5) | 225 (54.9) | 195 (53.0) | 56 (57.7) | 251 (54.0) | |
| Current | 66 (19.2) | 11 (16.7) | 77 (18.8) | 78 (21.2) | 18 (18.6) | 96 (20.6) | |
| P-Value b | 0.832 | 0.700 | |||||
| Physical Activity (MET-Hour/Week), Mean (SD) | 29.4 (29.7) | 35.4 (49.6) | 30.3 (33.7) | 27.9 (32.6) | 32.3 (30.9) | 28.8 (32.3) | 0.489 |
| P-Value b | 0.186 | 0.234 | |||||
| Physical Activity, N (%) | 0.171 | ||||||
| Low | 119 (34.6) | 19 (28.8) | 138 (33.7) | 152 (41.3) | 32 (33.0) | 184 (39.6) | |
| Moderate | 177 (51.4) | 36 (54.5) | 213 (52.0) | 176 (47.8) | 49 (50.5) | 225 (48.4) | |
| High | 48 (14.0) | 11 (16.7) | 59 (14.3) | 40 (10.9) | 16 (16.5) | 56 (12.0) | |
| P-Value b | 0.625 | 0.176 | |||||
| First-Degree Family History of PCa c, N (%) | 0.771 | ||||||
| No | 324 (94.2) | 64 (97.0) | 388 (94.6) | 348 (94.6) | 89 (91.8) | 437 (94.0) | |
| Yes | 20 (5.8) | 2 (3.0) | 22 (5.4) | 19 (5.1) | 8 (8.2) | 27 (5.8) | |
| Unknown | 1 (0.3) | 1 (0.2) | |||||
| P-Value b | 0.358 | 0.251 | |||||
| Aggressiveness *, N (%) | |||||||
| ISUP 1 | 207 (56.3) | 66 (68.0) | 273 (58.7) | ||||
| ISUP 2 | 71 (19.3) | 13 (13.4) | 84 (18.1) | ||||
| ISUP 3 | 30 (8.2) | 7 (7.2) | 37 (8.0) | ||||
| ISUP 4 | 41 (11.1) | 6 (6.2) | 47 (10.1) | ||||
| ISUP 5 | 18 (4.9) | 5 (5.2) | 23 (4.9) | ||||
| P-Value b | 0.263 | ||||||
| Controls N = 410 | PCa Cases N = 465 | P-Value a | aOR b (95% CI) | |
|---|---|---|---|---|
| n (%) | n (%) | |||
| Shift Work | ||||
| Never night shift | 344 (83.9) | 368 (79.1) | 0.071 | 1 |
| Ever night shift | 66 (16.1) | 97 (20.9) | 1.47 (1.02–2.11) | |
| Types of NightShift | ||||
| Never night shift | 0.073 | 1 | ||
| Permanent night shift | 34 (8.3) | 39 (8.4) | 1.21 (0.73–1.98) | |
| Rotating night shift | 32 (7.8) | 58 (12.5) | 1.73 (1.09–2.75) | |
| Chronotype c | ||||
| Morning | 247 (60.2) | 283 (60.8) | 0.622 | 1 |
| Neither | 125 (30.5) | 130 (28.0) | 0.94 (0.69–1.28) | |
| Evening | 34 (8.3) | 45 (9.7) | 1.18 (0.72–1.93) | |
| Missing | 4 (1.0) | 7 (1.5) | ||
| Sleep Duration c | ||||
| Recommended | 217 (52.9) | 234 (50.3) | 0.784 | 1 |
| May be appropriated | 124 (30.2) | 146 (31.4) | 1.11 (0.81–1.50) | |
| Not recommended | 65 (15.9) | 78 (16.8) | 1.18 (0.80–1.74) | |
| Missing | 4 (1.0) | 7 (1.5) |
| Ever Night Shift | Permanent Night Shift | Rotating Night Shift | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Controls N = 66 | PCa Cases N = 97 | aOR a (95% CI) | Controls N = 34 | PCa Cases N = 39 | aOR a (95% CI) | Controls N = 32 | PCa Cases N = 58 | aOR a (95% CI) | |
| N (%) | N (%) | N (%) | N (%) | N (%) | N (%) | ||||
| Lifetime Cumulative Duration of Night Shifts (Years) | |||||||||
| Never night shift | 1 | 1 | 1 | ||||||
| Tercile 1: ≤7 | 23 (5.6) | 29 (6.2) | 1.33 (0.75–2.38) | 18 (4.3) | 16 (3.4) | 0.97 (0.48–1.95) | 5 (1.2) | 13 (2.8) | 2.57 (0.90–7.34) |
| Tercile 2: >7–≤26 | 22 (5.4) | 40 (8.6) | 1.93 (1.11–3.36) | 8 (2.0) | 11 (2.4) | 1.58 (0.61–4.06) | 14 (3.4) | 29 (6.2) | 2.08 (1.08–4.04) |
| Tercile 3: >26 | 21 (5.1) | 28 (6.0) | 1.18 (0.65–2.14) | 8 (2.0) | 12 (2.6) | 1.37 (0.54–3.47) | 13 (3.2) | 16 (3.5) | 1.08 (0.51–2.29) |
| Intensity of Night Shift(Night Shifts/Year) | |||||||||
| Never night shift | 1 | 1 | 1 | ||||||
| Tercile 1: ≤74 | 22 (5.4) | 20 (4.3) | 0.88 (0.46–1.65) | 4 (1.0) | 18 (4.4) | 20 (4.3) | 1.05 (0.54–2.03) | ||
| Tercile 2: >74–≤250 | 23 (5.6) | 47 (10.1) | 2.06 (1.21–3.49) | 10 (2.4) | 12 (2.6) | 1.26 (0.52–3.05) | 13 (3.2) | 35 (7.5) | 2.60 (1.34–5.02) |
| Tercile 3: >250 | 20 (4.9) | 27 (5.9) | 1.40 (0.76–2.58) | 20 (4.9) | 27 (5.8) | 1.40 (0.76–2.58) | |||
| Unknown b,* | 1 (0.2) | 3 (0.6) | 1 (0.2) | 3 (0.6) | |||||
| Morning Chronotype | Neither Chronotype | Evening Chronotype | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Controls N = 247 | PCa Cases N = 283 | aOR a (95% CI) | Controls N = 125 | PCa Cases N = 130 | aOR a (95% CI) | Controls N = 34 | PCa Cases N = 45 | aOR a (95% CI) | P-Interaction | |
| Shift Work | ||||||||||
| Never night shift | 208 (84.2) | 232 (82.0) | 1 | 109 (87.2) | 106 (81.5) | 1 | 27 (79.4) | 29 (64.4) | 1 | 0.280 |
| Ever night shift | 39 (15.8) | 51 (18.0) | 1.25 (0.78–2.00) | 16 (12.8) | 24 (18.5) | 1.71 (0.83–3.51) | 7 (20.6) | 16 (35.6) | 3.14 (0.91–10.76) | |
| Types of Night Shift | ||||||||||
| Never night shift | 1 | 1 | 1 | 0.199 | ||||||
| Permanent night shift | 20 (8.1) | 19 (6.7) | 0.99 (0.50–1.94) | 9 (7.2) | 11 (8.5) | 1.64 (0.61–4.40) | 4 (11.8) | 9 (20.0) | 3.53 (0.76–16.34) | |
| Rotating night shift | 19 (7.7) | 32 (11.3) | 1.50 (0.82–2.75) | 7 (5.6) | 13 (10.0) | 1.77 (0.66–4.73) | 3 (8.8) | 7 (15.6) | 2.72 (0.54–13.62) | |
| Lifetime Cumulative Duration of Night Shift (Years) | ||||||||||
| Never night shift | 1 | 1 | 1 | 0.107 | ||||||
| Tercile 1: ≤7 | 11 (4.5) | 15 (5.3) | 1.40 (0.62–3.19) | 9 (7.2) | 11 (8.5) | 1.56 (0.58–4.21) | 3 (8.8) | 3 (6.7) | 1.26 (0.19–8.47) | |
| Tercile 2: >7–≤26 | 12 (4.8) | 22 (7.7) | 1.78 (0.85–3.76) | 4 (3.2) | 9 (6.9) | 2.51 (0.72–8.75) | 4 (11.8) | 7 (15.6) | 2.58 (0.54–12.37) | |
| Tercile 3: >26 | 16 (6.5) | 14 (5.0) | 0.78 (0.37–1.66) | 3 (2.4) | 5 (3.1) | 1.14 (0.24–5.39) | 6 (13.3) | |||
| Intensity of NightShift(Nights Shifts/Year) | ||||||||||
| Never night work | 1 | 1 | 1 | 0.450 | ||||||
| Tercile 1: ≤74 | 16 (6.5) | 11 (3.9) | 0.61 (0.27–1.37) | 4 (3.2) | 5 (3.9) | 1.17 (0.29–4.66) | 1 (3.0) | 3 (6.7) | 3.54 (0.26–48.22) | |
| Tercile 2: >74–≤250 | 12 (4.8) | 28 (9.9) | 2.22 (1.09–4.55) | 6 (4.8) | 11 (8.5) | 2.13 (0.72–6.30) | 3 (8.8) | 6 (13.3) | 2.87 (0.55–14.84) | |
| Tercile 3: >250 | 11 (4.5) | 12 (4.2) | 1.14 (0.48–2.71) | 6 (4.8) | 8 (6.2) | 1.69 (0.52–5.49) | 3 (8.8) | 7 (15.6) | 3.29 (0.62–17.50) | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lozano-Lorca, M.; Olmedo-Requena, R.; Vega-Galindo, M.-V.; Vázquez-Alonso, F.; Jiménez-Pacheco, A.; Salcedo-Bellido, I.; Sánchez, M.-J.; Jiménez-Moleón, J.-J. Night Shift Work, Chronotype, Sleep Duration, and Prostate Cancer Risk: CAPLIFE Study. Int. J. Environ. Res. Public Health 2020, 17, 6300. https://doi.org/10.3390/ijerph17176300
Lozano-Lorca M, Olmedo-Requena R, Vega-Galindo M-V, Vázquez-Alonso F, Jiménez-Pacheco A, Salcedo-Bellido I, Sánchez M-J, Jiménez-Moleón J-J. Night Shift Work, Chronotype, Sleep Duration, and Prostate Cancer Risk: CAPLIFE Study. International Journal of Environmental Research and Public Health. 2020; 17(17):6300. https://doi.org/10.3390/ijerph17176300
Chicago/Turabian StyleLozano-Lorca, Macarena, Rocío Olmedo-Requena, María-Victoria Vega-Galindo, Fernando Vázquez-Alonso, Antonio Jiménez-Pacheco, Inmaculada Salcedo-Bellido, María-José Sánchez, and José-Juan Jiménez-Moleón. 2020. "Night Shift Work, Chronotype, Sleep Duration, and Prostate Cancer Risk: CAPLIFE Study" International Journal of Environmental Research and Public Health 17, no. 17: 6300. https://doi.org/10.3390/ijerph17176300