Plasma Aromatase Activity Index, Gonadotropins and Estrone Are Associated with Frailty Syndrome in Post-Menopausal Women with Breast Cancer

 and
and 
Abstract
:1. Introduction
- -
- To describe the presence of frailty syndrome and its severity in postmenopausal women with hormone-dependent breast cancer before starting hormonal therapy.
- -
- To determine whether frailty syndrome is associated with alterations in geriatric assessment.
- -
- To ascertain whether frailty syndrome and geriatric assessment are associated with hormonal gonadal alterations in androgens and estrogens, gonadotropins levels, and the aromatase activity index in the blood.
2. Methods
2.1. Design and Study Population
2.2. Assessment of Frailty Syndrome
2.3. Geriatric Assessment
2.4. Measurement of Hormones in Plasma
2.5. Aromatase Activity Index in Plasma
2.6. Statistical Analysis
3. Results
3.1. Sociodemographic and Clinical Data
3.2. Evaluation of Frailty Syndrome
3.3. Evaluation of the Frailty Score and Socio-Demographic and Clinical Variables
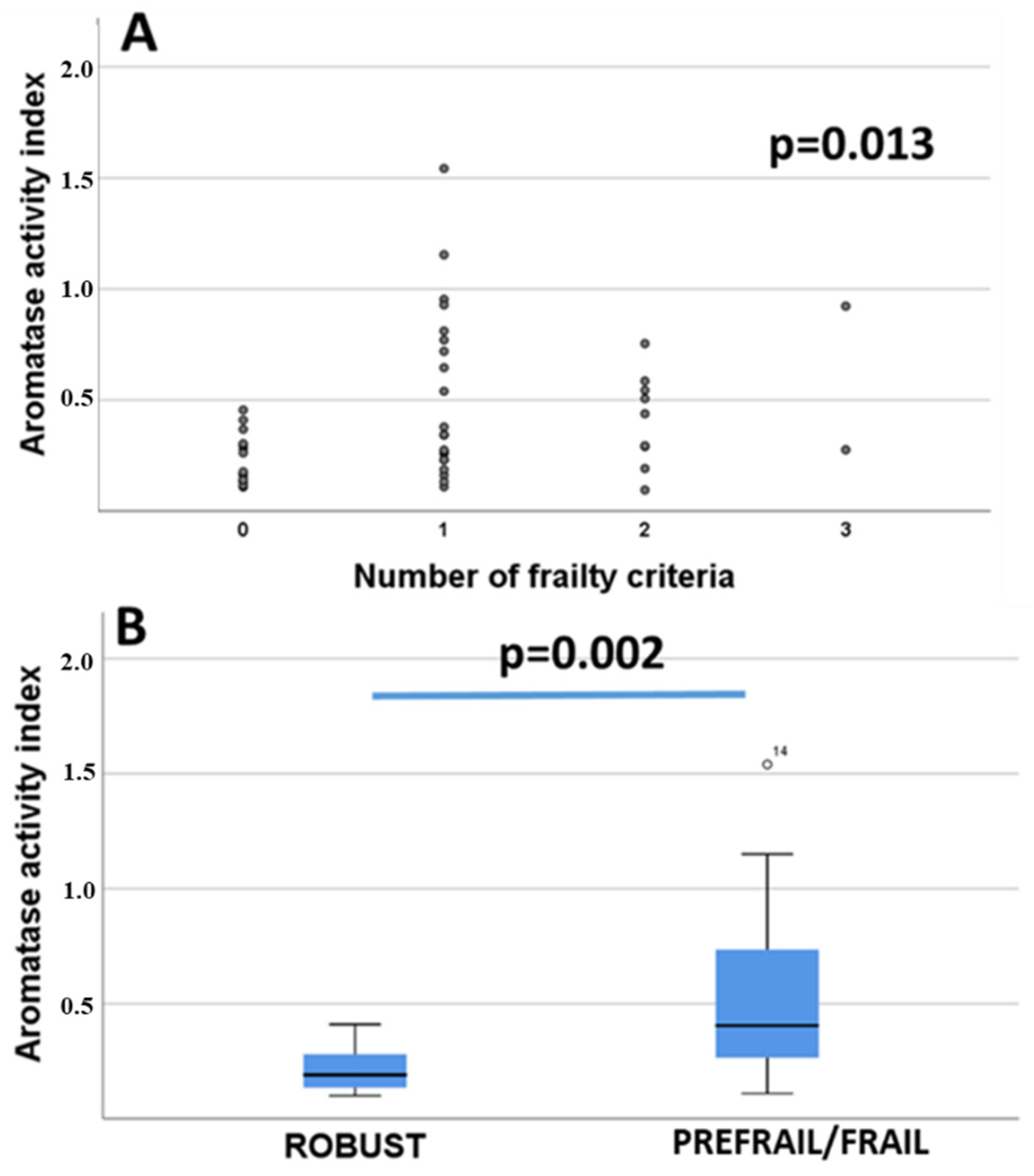
3.4. Frailty Syndrome and the Concentration of Androgens and Estrogens and the Aromatase Activity Index in the Blood
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Li, X.; Oprea-Ilies, G.M.; Krishnamurti, U. New developments in breast cancer and their impact on daily practice in pathology. Arch. Pathol. Lab. Med. 2017, 141, 490–498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mattiuzzi, C.; Lippi, G. Current cancer epidemiology. J. Epidemiol. Glob. Health 2019, 9, 217–222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferrando, J.; Palència, L.; Gotsens, M.; Puig-Barrachina, V.; Marí-Dell’Olmo, M.; Rodríguez-Sanz, M.; Bartoll, X.; Borrell, C. Trends in cancer mortality in Spain: The influence of the financial crisis. Gac. Sanit. 2019, 33, 229–234. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Meng, X.; Chen, Y.; Leng, S.X.; Zhang, H. The biology of aging and cancer: Frailty, inflammation, and immunity. Cancer J. 2017, 23, 201–205. [Google Scholar] [CrossRef] [PubMed]
- Cesari, M.; Calvani, R.; Marzetti, E. Frailty in older persons. Clin. Geriatr. Med. 2017, 33, 293–303. [Google Scholar] [CrossRef] [PubMed]
- Fried, L.P.; Ferrucci, L.; Darer, J.; Williamson, J.D.; Anderson, G. Untangling the concepts of disability, frailty, and comorbidity: Implications for improved targeting and care. J. Gerontol. A Biol. Sci. Med. Sci. 2004, 59, 255–263. [Google Scholar] [CrossRef] [Green Version]
- Wilson, D.; Jackson, T.; Sapey, E.; Lord, J.M. Frailty and sarcopenia: The potential role of an aged immune system. Ageing Res. Rev. 2017, 36, 1–10. [Google Scholar] [CrossRef]
- Wildiers, H.; Heeren, P.; Puts, M.; Topinkova, E.; Janssen-Heijnen, M.L.; Extermann, M.; Falandry, C.; Artz, A.; Brain, E.; Colloca, G.; et al. International Society of Geriatric Oncology consensus on geriatric older patients with cancer. J. Clin. Oncol. 2014, 32, 2595–2603. [Google Scholar] [CrossRef] [Green Version]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef]
- Ruan, H.; Hu, J.; Zhao, J.; Tao, H.; Chi, J.; Niu, X.; Zhang, J.; Wang, Y. Menopause and frailty: A scoping review. Menopause 2020, 27, 1185–1195. [Google Scholar] [CrossRef]
- Walston, J.; Fried, L.P. Frailty and the older man. Med. Clin. N. Am. 1999, 83, 1173–1194. [Google Scholar] [CrossRef]
- Poehlman, E.T.; Toth, M.J.; Fishman, P.S.; Vaitkevicius, P.; Gottlieb, S.S.; Fisher, M.L.; Fonong, T. Sarcopenia in aging humans: The impact of menopause and disease. J. Gerontol. A Biol. Sci. Med. 1995, 50, 73–77. [Google Scholar]
- Wu, I.C.; Lin, X.Z.; Liu, P.F.; Tsai, W.L.; Shiesh, S.C. Low serum testosterone and frailty in older men and women. Maturitas 2010, 67, 348–352. [Google Scholar] [CrossRef] [PubMed]
- Mohr, B.A.; Bhasin, S.; Kupelian, V.; Araujo, A.B.; O’Donnell, A.B.; McKinlay, J.B. Testosterone, sex hormone-binding globulin, and frailty in older men. J. Am. Geriatr. Soc. 2007, 55, 548–555. [Google Scholar] [CrossRef]
- O’Donnell, A.B.; Araujo, A.B.; McKinlay, J.B. The health of normally aging men: The Massachusetts Male Aging Study (1987–2004). Exp. Gerontol. 2004, 39, 975–984. [Google Scholar] [CrossRef]
- Carcaillon, L.; García-García, F.J.; Tresguerres, J.A.F.; Guitiérrez Avila, G.; Kireev, R.; Rodríguez-Mañas, L. Higher levels of endrogenous estradiol are associated with frailty in postmenpausal women from the Toledo study for healthy aging. J. Clin. Endorinol. Metab. 2012, 97, 2898–2906. [Google Scholar] [CrossRef] [Green Version]
- Orentreich, N.; Brind, J.L.; Rizer, R.L.; Vogelman, J.H. Age changes and sex differences in serum dehydroepiandrosterone sulfate concentrations throughout adulthood. J. Clin. Endocrinol. Metab. 1984, 59, 551–555. [Google Scholar] [CrossRef]
- Cappola, A.R.; Xue, Q.L.; Fried, L.P. Multiple hormonal deficiencies in anabolic hormones are found in frail older women: The Women’s Health and Aging studies. J. Gerontol. A Biol. Sci. Med. Sci. 2009, 64, 243–248. [Google Scholar] [CrossRef] [Green Version]
- Leng, S.X.; Cappola, A.R.; Andersen, R.E.; Blackman, M.R.; Koenig, K.; Blair, M.; Walston, J.D. Serum levels of insulin-like growth factor-I (IGF-I) and dehydroepiandrosterone sulfate (DHEA-S), and their relationships with serum interleukin-6, in the geriatric syndrome of frailty. Aging Clin. Exp. Res. 2004, 16, 153–157. [Google Scholar] [CrossRef]
- Cawthon, P.M.; Ensrud, K.E.; Laughlin, G.A.; Cauley, J.A.; Dam, T.T.; Barrett-Connor, E.; Fink, H.A.; Hoffman, A.R.; Lau, E.; Lane, N.E.; et al. Sex hormones and frailty in older men: The osteoporotic fractures in men (MrOS) study. J. Clin. Endocrinol. Metab. 2009, 94, 3806–3815. [Google Scholar] [CrossRef] [Green Version]
- Travison, T.G.; Nguyen, A.H.; Naganathan, V.; Stanaway, F.F.; Blyth, F.M.; Cumming, R.G.; Le Couteur, D.G.; Sambrook, P.N.; Handelsman, D.J. Changes in reproductive hormone concentrations predict the prevalence and progression of the frailty syndrome in older men: The concord health and ageing in men project. J. Clin. Endocrinol. Metab. 2011, 96, 2464–2474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eichholzer, M.; Barbir, A.; Basaria, S.; Dobs, A.S.; Feinleib, M.; Guallar, E.; Menke, A.; Nelson, W.G.; Rifai, N.; Platz, E.A.; et al. Serum sex steroid hormones and frailty in older American men of the Third National Health and Nutrition Examination Survey (NHANES III). Aging Male 2012, 15, 208–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bellieni, A.; Fusco, D.; Sanchez, A.M.; Franceschini, G.; Di Capua, B.; Allocca, E.; Di Stasio, E.; Marazzi, F.; Tagliaferri, L.; Masetti, R.; et al. Different impact of definitions of sarcopenia in defining frailty status in a population of older women with early breast cancer. J. Pers. Med. 2021, 11, 243. [Google Scholar] [CrossRef] [PubMed]
- Horstman, A.M.; Dillon, E.L.; Urban, R.J.; Sheffield-Moore, M. The role of androgens and estrogens on healthy aging and longevity. J. Gerontol. A Biol. Sci. Med. Sci. 2012, 67, 1140–1152. [Google Scholar] [CrossRef] [Green Version]
- Almeida, M.; Laurent, M.R.; Dubois, V.; Claessens, F.; O’Brien, C.A.; Bouillon, R.; Vanderschueren, D.; Manolagas, S.C. Estrogens and androgens in skeletal physiology and pathophysiology. Physiol. Rev. 2017, 97, 135–187. [Google Scholar] [CrossRef]
- Li, J.J.; Shao, Z.M. Endocrine therapy as adjuvant or neoadjuvant therapy for breast cancer: Selecting the best agents, the timing and duration of treatment. Chin. Clin. Oncol. 2016, 5, 40. [Google Scholar] [CrossRef]
- Fernández-Garrido, J.; Navarro-Martínez, R.; Buigues-González, C.; Martínez-Martínez, M.; Ruiz-Ros, V.; Cauli, O. The value of neutrophil and lymphocyte count in frail older women. Exp. Gerontol. 2014, 54, 35–41. [Google Scholar] [CrossRef]
- Orme, J.G.; Reis, J.; Herz, E.J. Factorial and discriminant validity of the Center for Epidemiological Studies Depression (CES-D) scale. J. Clin. Psychol. 1986, 42, 28–33. [Google Scholar] [CrossRef]
- Rubio Castañeda, F.J.; Tomás Aznar, C.; Muro Baquero, C. Medición de la actividad física en personas mayores de 65 años mediante el IPAQ-E: Validez de contenido, fiabilidad y factores asociados [Validity, Reliability and Associated Factors of the International Physical Activity Questionnaire Adapted to Elderly (IPAQ-E)]. Rev. Esp. Salud Publica 2017, 18, 91. [Google Scholar]
- Treacy, D.; Hassett, L. The short physical performance battery. J. Physiother. 2018, 64, 61. [Google Scholar] [CrossRef]
- Graham, J.E.; Ostir, G.V.; Fisher, S.R.; Ottenbacher, K.J. Assessing walking speed in clinical research: A systematic review. J. Eval. Clin. Pract. 2008, 14, 552–562. [Google Scholar] [CrossRef] [PubMed]
- Lobo, A.; Saz, P.; Marcos, G.; Día, J.L.; de la Cámara, C.; Ventura, T.; Morales Asín, F.; Fernando Pascual, L.; Montañés, J.A.; Aznar, S. Revalidación y normalización del Mini-Examen Cognoscitivo (primera versión en castellano del Mini-Mental Status Examination) en la población general geriátrica [Revalidation and standardization of the cognition mini-exam (first Spanish version of the Mini-Mental Status Examination) in the general geriatric population]. Med. Clin. 1999, 112, 767–774, Erratum in Med. Clin. 1999, 113, 197. [Google Scholar]
- Sheikh, J.I.; Yesavage, J.A.; Brooks, J.O., III; Friedman, L.; Gratzinger, P.; Hill, R.D.; Zadeik, A.; Crook, T. Proposed factor structure of the Geriatric Depression Scale. Int. Psychogeriatr. 1991, 3, 23–28. [Google Scholar] [CrossRef]
- Orcos, R.O.; Fort, M.S.; Khajoui, A.K.; Aparicio, S.V.; Del Valle, R.D.D. Validación de la versión española de 5 y 15 ítems de la Escala de Depresión Geriátrica en personas mayores en Atención Primaria [Validation of 5 and 15 items Spanish version of the geriatric depression scale in elderly subjects in primary health care setting]. Rev. Clin. Esp. 2007, 207, 559–562. [Google Scholar]
- González, N.; Bilbao, A.; Forjaz, M.J.; Ayala, A.; Orive, M.; Garcia-Gutierrez, S.; Hayas, C.L.; Quintana, J.M.; OFF (Older Falls Fracture)-IRYSS group. Psychometric characteristics of the Spanish version of the Barthel Index. Aging Clin. Exp. Res. 2018, 30, 489–497. [Google Scholar] [CrossRef] [PubMed]
- Kondrup, J.; Allison, S.P.; Elia, M.; Vellas, B.; Plauth, M.; Educational and Clinical Practice Committee; European Society of Parenteral and Enteral Nutrition (ESPEN). ESPEN guidelines for nutrition screening 2002. Clin. Nutr. 2003, 22, 415–421. [Google Scholar] [CrossRef]
- Winter, J.E.; MacInnis, R.J.; Nowson, C.A. The influence of age on the BMI and all-cause mortality association: A meta-analysis. J. Nutr. Health Aging 2017, 21, 1254–1258. [Google Scholar] [CrossRef]
- Setiati, S.; Istanti, R.; Andayani, R.; Kuswardhani, R.A.; Aryana, I.G.; Putu, I.D.; Apandi, M.; Ichwani, J.; Soewoto, S.; Dinda, R.; et al. Cut-off of anthropometry measurement and nutritional status among elderly outpatient in Indonesia: Multi-centre study. Acta Med. Indones. 2010, 42, 224–230. [Google Scholar]
- Heim, N.; Snijder, M.B.; Heymans, M.W.; Deeg, D.J.; Seidell, J.C.; Visser, M. Optimal cutoff values for high-risk waist circumference in older adults based on related health outcomes. Am. J. Epidemiol. 2011, 174, 479–489. [Google Scholar] [CrossRef]
- Gómez-Benito, J.; Ruiz, C.; Guilera, G. A Spanish version of the Athens Insomnia Scale. Qual. Life Res. 2011, 20, 931–937. [Google Scholar] [CrossRef] [Green Version]
- Soldatos, C.R.; Dikeos, D.G.; Paparrigopoulos, T.J. The diagnostic validity of the Athens Insomnia Scale. J. Psychosom. Res. 2003, 55, 263–267. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Vermeulen, A.; Deslypere, J.P.; Paridaens, R.; Leclercq, G.; Roy, F.; Heuson, J.C. Aromatase, 17 beta-hydroxysteroid dehydrogenase and intratissular sex hormone concentrations in cancerous and normal glandular breast tissue in postmenopausal women. Eur. J. Cancer Clin. Oncol. 1986, 22, 515–525. [Google Scholar] [CrossRef]
- Newton, C.J.; Samuel, D.L.; James, V.H. Aromatase activity and concentrations of cortisol, progesterone and testosterone in breast and abdominal adipose tissue. J. Steroid Biochem. 1986, 24, 1033–1039. [Google Scholar] [CrossRef]
- Kraemer, H.C. Correlation coefficients in medical research: From product moment correlation to the odds ratio. Stat. Methods Med. Res. 2006, 15, 525–545. [Google Scholar] [CrossRef]
- Mukaka, M.M. Statistics corner: A guide to appropriate use of correlation coefficient in medical research. Malawi Med. J. 2012, 24, 69–71. [Google Scholar]
- Early Breast Cancer Trialists’ Collaborative Group (EBCTG); Peto, R.; Davies, C.; Godwin, J.; Gray, R.; Pan, H.C.; Clarke, M.; Cutter, D.; Dardy, S.; McGale, P.; et al. Comparisons between different poly-chemotherapy regimens for early breast cancer: Meta-analyses of long-term outcome among 100,000 women in 123 randomised trials. Lancet 2012, 379, 432–444. [Google Scholar]
- Gianni, L.; Baselga, J.; Eiermann, W.; Porta, V.G.; Semiglazov, V.; Lluch, A.; Zambetti, M.; Sabadell, D.; Raab, G.; Cussac, A.L.; et al. Phase III trial evaluating the addition of paclitaxel to doxorubicin followed by cyclophosphamide, methotrexate, and fluorouracil, as adjuvant or primary systemic therapy: European Cooperative Trial in Operable Breast Cancer. J. Clin. Oncol. 2009, 27, 2474–2481. [Google Scholar] [CrossRef]
- Campos, S. Liposomal anthracyclines: Adjuvant and neoadjuvant therapy for breast cancer. Oncologist 2003, 8, 10–16. [Google Scholar] [CrossRef]
- Jones, S.; Holmes, F.A.; O’Shaughnessy, J.; Blum, J.L.; Vukelja, S.J.; McIntyre, K.J.; Pippen, J.E.; Bordelon, J.H.; Kirby, R.L.; Sandbach, J.; et al. Docetaxel with cyclophosphamide is associated with an overall survival benefit compared with doxorubicin and cyclophosphamide: 7-year follow-up of US Oncology Research Trial 9735. J. Clin. Oncol. 2009, 27, 1177–1183. [Google Scholar] [CrossRef]
- Gianni, L.; Pienkowski, T.; Im, Y.H.; Roman, L.; Tseng, L.M.; Liu, M.C.; Lluch, A.; Staroslawska, E.; de la Haba-Rodriguez, J.; Im, S.A.; et al. Efficacy and safety of neoadjuvant pertuzumab and trastuzumab in women with locally advanced, inflammatory, or early HER2-positive breast cancer (NeoSphere): A randomised multicentre, open-label, phase 2 trial. Lancet Oncol. 2012, 13, 25–32. [Google Scholar] [CrossRef]
- Schneeweiss, A.; Chia, S.; Hickish, T.; Harvey, V.; Eniu, A.; Hegg, R.; Tausch, C.; Seo, J.H.; Tsai, Y.F.; Ratnayake, J.; et al. Pertuzumab plus trastuzumab in combination with standard neoadjuvant anthracycline-containing and anthracycline-free chemotherapy regimens in patients with HER2-positive early breast cancer: A randomized phase II cardiac safety study (TRYPHAENA). Ann. Oncol. 2013, 24, 2278–2284. [Google Scholar] [CrossRef] [PubMed]
- Weiss, C.O. Frailty and chronic diseases in older adults. Clin. Geriatr. Med. 2011, 27, 39–52. [Google Scholar] [CrossRef] [PubMed]
- Cesari, M.; Leeuwenburgh, C.; Lauretani, F.; Onder, G.; Bandinelli, S.; Maraldi, C.; Guralnik, J.M.; Pahor, M.; Ferrucci, L. Frailty syndrome and skeletal muscle: Results from the Invecchiare in Chianti study. Am. J. Clin. Nutr. 2006, 83, 1142–1148. [Google Scholar] [CrossRef] [PubMed]
- Bandeen-Roche, K.; Xue, Q.L.; Ferrucci, L.; Walston, J.; Guralnik, J.M.; Chaves, P.; Zeger, S.L.; Fried, L.P. Phenotype of Frailty: Characterization in the women’s health and aging studies. J. Gerontol. A Biol. Sci. Med. Sci. 2006, 61, 262–266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woods, N.F.; LaCroix, A.Z.; Gray, S.L.; Aragaki, A.; Cochrane, B.B.; Brunner, R.L.; Masaki, K.; Murray, A.; Newman, A.B.; Women’s Health Initiative. Frailty: Emergence and consequences in women aged 65 and older in the Women’s Health Initiative Observational Study. J. Am. Geriatr. Soc. 2005, 53, 1321–1330, Erratum in J. Am. Geriatr. Soc. 2017, 65, 1631–1632. [Google Scholar] [CrossRef] [Green Version]
- Santos-Eggimann, B.; Cuénoud, P.; Spagnoli, J.; Junod, J. Prevalence of frailty in middle-aged and older community-dwelling Europeans living in 10 countries. J. Gerontol. A Biol. Sci. Med. Sci. 2009, 64, 675–681. [Google Scholar] [CrossRef] [Green Version]
- Wang, S.; Yang, T.; Qiang, W.; Shen, A.; Zhao, Z.; Yang, H.; Liu, X. The prevalence of frailty among breast cancer patients: A systematic review and meta-analysis. Support Care Cancer 2022, 30, 2993–3006. [Google Scholar] [CrossRef]
- Kirkhus, L.; Šaltytė Benth, J.; Grønberg, B.H.; Hjermstad, M.J.; Rostoft, S.; Harneshaug, M.; Selbæk, G.; Wyller, T.B.; Jordhøy, M.S. Frailty identified by geriatric assessment is associated with poor functioning, high symptom burden and increased risk of physical decline in older cancer patients: Prospective observational study. Palliat. Med. 2019, 33, 312–322. [Google Scholar] [CrossRef] [Green Version]
- Gilmore, N.; Kadambi, S.; Lei, L.; Loh, K.P.; Mohamed, M.; Magnuson, A.; Cole, S.; Esparaz, B.T.; Giguere, J.K.; Mohile, S.; et al. Associations of inflammation with frailty in patients with breast cancer aged 50 and over receiving chemotherapy. J. Geriatr. Oncol. 2020, 11, 423–430. [Google Scholar] [CrossRef]
- Garcia-Garcia, F.J.; Gutierrez Avila, G.; Alfaro-Acha, A.; Amor Andres, M.S.; De Los Angeles De La Torre Lanza, M.; Escribano Aparicio, M.V.; Humanes Aparicio, S.; Larrion Zugasti, J.L.; Gomez-Serranillo Reus, M.; Rodriguez-Artalejo, F.; et al. The prevalence of frailty syndrome in an older population from Spain. The Toledo Study for Healthy Aging. J. Nutr. Health Aging 2011, 15, 852–856. [Google Scholar] [CrossRef] [PubMed]
- Cordova, M.J.; Giese-Davis, J.; Golant, M.; Kronenwetter, C.; Vickie, C.; Spiegel, D. Breast cancer as trauma: Posttraumatic stress and posttraumatic growth. J. Clin. Psychol. Med. Settings 2007, 14, 308–319. [Google Scholar] [CrossRef]
- Tsaras, K.; Papathanasiou, I.V.; Mitsi, D.; Veneti, A.; Kelesi, M.; Zyga, S.; Fradelos, E.C. Assessment of depression and anxiety in breast cancer patients: Prevalence and associated factors. Asian Pac. J. Cancer Prev. 2018, 19, 1661–1669. [Google Scholar] [PubMed]
- Zhu, J.; Fang, F.; Sjölander, A.; Fall, K.; Adami, H.O.; Valdimarsdóttir, U. First-onset mental disorders after cancer diagnosis and cancer-specific mortality: A nationwide cohort study. Ann. Oncol. 2017, 28, 1964–1969. [Google Scholar] [CrossRef] [PubMed]
- Nicholson, B.D.; Hamilton, W.; O’Sullivan, J.; Aveyard, P.; Hobbs, F.R. Weight loss as a predictor of cancer in primary care: A systematic review and meta-analysis. Br. J. Gen. Pract. 2018, 68, e311–e322. [Google Scholar] [CrossRef]
- Jackson, S.E.; Williams, K.; Steptoe, A.; Wardle, J. The impact of a cancer diagnosis on weight change: Findings from prospective, population-based cohorts in the UK and the US. BMC Cancer 2014, 14, 926. [Google Scholar] [CrossRef] [Green Version]
- Avila-Funes, J.A.; Amieva, H.; Barberger-Gateau, P.; Le Goff, M.; Raoux, N.; Ritchie, K.; Carrière, I.; Tavernier, B.; Tzourio, C.; Gutiérrez-Robledo, L.M.; et al. Cognitive impairment improves the predictive validity of the phenotype of frailty for adverse health outcomes: The Three-City Study. J. Am. Geriatr. Soc. 2009, 57, 453–461. [Google Scholar] [CrossRef]
- Samper-Ternent, R.; Al Snih, S.; Raji, M.A.; Markides, K.S.; Ottenbacher, K.J. Relationship between frailty and cognitive decline in older Mexicans Americans. J. Am. Geriatr. Soc. 2008, 56, 1845–1852. [Google Scholar] [CrossRef]
- Jürschik, P.; Nunin, C.; Botigue, T.; Escobar, M.A.; Lavedan, A.; Viladrosa, M. Prevalence of frailty and factors associated with frailty in the elderly population of Lleida, Spain: The FRALLE survey. Arch. Gerontol. Geriatr. 2012, 55, 625–631. [Google Scholar] [CrossRef]
- Boyle, P.A.; Buchman, A.S.; Wilson, R.S.; Leurgans, S.E.; Bennett, D.A. Association of muscle strength with the risk of Alzheimer disease and the rate of cognitive decline in community-dwelling older persons. Arch. Neurol. 2009, 66, 1339–1344. [Google Scholar] [CrossRef] [Green Version]
- Mitnitski, A.; Fallah, N.; Rockwood, K. A multistate model of cognitive dynamics in relation to frailty in older adults. Ann. Epidemiol. 2011, 21, 507–516. [Google Scholar] [CrossRef] [PubMed]
- Yassuda, M.S.; Lopes, A.; Cachioni, M.; Falcao, D.V.; Batistoni, S.S.; Guimaraes, V.V.; Neri, A.L. Frailty criteria and cognitive performance are related: Data from the FIBRA study in Ermelino Matarazzo, São Paulo, Brazil. J. Nutr. Health Aging 2012, 16, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Swiecicka, A.; Eendebak, R.J.A.H.; Lunt, M.; O’Neill, T.W.; Bartfai, G.; Casanueva, F.F.; Forti, G.; Giwercman, A.; Han, T.S.; Slowikowska-Hilczer, J.; et al. Reproductive hormone levels predict changes in frailty status in community-dwelling older men: European Male Ageing Study Prospective Data. J. Clin. Endocrinol. Metab. 2018, 103, 701–709. [Google Scholar] [CrossRef] [PubMed]
- Huang, G.; Coviello, A.; LaValley, M.P.; Ensrud, K.E.; Cauley, J.A.; Cawthon, P.M.; Fredman, L. Surgical menopause and frailty risk in community-dwelling older women: Study of osteoporotic fractures. J. Am. Geriatr. Soc. 2018, 66, 2172–2177. [Google Scholar] [CrossRef]
- Tajar, A.; O’Connell, M.D.; Mitnitski, A.B.; O’Neill, T.W.; Searle, S.D.; Huhtaniemi, I.T.; Finn, J.D.; Bartfai, G.; Boonen, S.; Casanueva, F.F.; et al. Frailty in relation to variations in hormone levels of the hypothalamic-pituitary-testicular axis in older men: Results from the European male aging study. J. Am. Geriatr. Soc. 2011, 59, 814–821. [Google Scholar] [CrossRef] [PubMed]
- Schaap, L.A.; van Schoor, N.M.; Lips, P.; Visser, M. Associations of sarcopenia definitions, and their components, with the incidence of recurrent falling and fractures: The longitudinal aging study Amsterdam. J. Gerontol. A. Biol. Sci. Med. Sci. 2018, 73, 1199–1204. [Google Scholar] [CrossRef] [PubMed]
- Baumgartner, R.N.; Waters, D.L.; Gallagher, D.; Morley, J.E.; Garry, P.J. Predictors of skeletal muscle mass in elderly men and women. Mech. Ageing Dev. 1999, 107, 123–136. [Google Scholar] [CrossRef]
- Subramanian, A.; Salhab, M.; Mokbel, K. Oestrogen producing enzymes and mammary carcinogenesis: A review. Breast Cancer Res. Treat. 2008, 111, 191–202. [Google Scholar] [CrossRef]
- Reiner, A.P.; Aragaki, A.K.; Gray, S.L.; Wactawski-Wende, J.; Cauley, J.A.; Cochrane, B.B.; Kooperberg, C.L.; Woods, N.F.; LaCroix, A.Z. Inflammation and thrombosis biomarkers and incident frailty in postmenopausal women. Am. J. Med. 2009, 122, 947–954. [Google Scholar] [CrossRef] [Green Version]
- Leng, S.X.; Xue, Q.L.; Tian, J.; Walston, J.D.; Fried, L.P. Inflammation and frailty in older women. J. Am. Geriatr. Soc. 2007, 55, 864–871. [Google Scholar] [CrossRef]
- Gale, C.R.; Baylis, D.; Cooper, C.; Sayer, A.A. Inflammatory markers and incident frailty in men and women: The English Longitudinal Study of Ageing. Age 2013, 35, 2493–2501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Netz, Y.; Ben-Zaken, S.; Zeev, A.; Dunsky, A. Correlates of early-stage frailty-sleep, fitness, oxidative stress, and BMI. Front. Med. 2021, 7, 594710. [Google Scholar] [CrossRef] [PubMed]
- Baptista, G.; Dupuy, A.M.; Jaussent, A.; Durant, R.; Ventura, E.; Sauguet, P.; Picot, M.C.; Jeandel, C.; Cristol, J.P. Low-grade chronic inflammation and superoxide anion production by NADPH oxidase are the main determinants of physical frailty in older adults. Free Radic. Res. 2012, 46, 1108–1114. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Garrido, J.; Ruiz-Ros, V.; Buigues, C.; Navarro-Martinez, R.; Cauli, O. Clinical features of prefrail older individuals and emerging peripheral biomarkers: A systematic review. Arch. Gerontol. Geriatr. 2014, 59, 7–17. [Google Scholar] [CrossRef]
- Morley, J.E.; Vellas, B.; Van Kan, G.A.; Anker, S.D.; Bauer, J.M.; Bernabei, R.; Cesari, M.; Chumlea, W.C.; Doehner, W.; Evans, J.; et al. Frailty consensus: A call to action. J. Am. Med. Dir. Assoc. 2013, 14, 392–397. [Google Scholar] [CrossRef] [Green Version]
- Walston, J.; Robinson, T.N.; Zieman, S.; McFarland, F.; Carpenter, C.R.; Althoff, K.N.; Andrew, M.K.; Blaum, C.S.; Brown, P.J.; Buta, B.; et al. Integrating frailty research into the medical specialties—Report from a U13 conference. J. Am. Geriatr. Soc. 2017, 65, 2134–2139. [Google Scholar] [CrossRef] [Green Version]
- Martinez-Tapia, C.; Laurent, M.; Paillaud, E.; Caillet, P.; Ferrat, E.; Lagrange, J.L.; Rwabihama, J.P.; Allain, M.; Chahwakilian, A.; Boudou-Rouquette, P.; et al. Predicting frailty and geriatric interventions in older cancer patients: Performance of two screening tools for seven frailty definitions-ELCAPA cohort. Cancers 2022, 14, 244. [Google Scholar] [CrossRef]
- Jauhari, Y.; Gannon, M.R.; Dodwell, D.; Horgan, K.; Tsang, C.; Clements, K.; Medina, J.; Tang, S.; Pettengell, R.; Cromwell, D.A. Addressing frailty in patients with breast cancer: A review of the literature. Eur. J. Surg. Oncol. 2020, 46, 24–32. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variables | Frequency % (Categorical Variables) or Mean and Standard Error of the Mean (Range Min-Max) (Discrete Variables) |
|---|---|
| Age (years) | 66.8 ± 1.3 (52–83) |
| Marital status: | |
| Married | 23 (48.9%) |
| Divorced | 7 (14.9%) |
| Separated | 2 (4.3%) |
| Single | 4 (8.5%) |
| Widow | 11 (24.4%) |
| Histology of tumor: | |
| Ductal carcinoma | 46 (97.9%) |
| Lobular carcinoma | 1 (2.1%) |
| Estrogen receptor staining (%) | 93.1 ± 1.6 (40–100) |
| Progesterone receptor staining (%) | 61.3 ± 0.09 (1–3) |
| HER2-positive staining (patients with 3 + staining in HER2: 4 patients) | 2.5 ± 5.2 (0–10) |
| Ki67 mean values (%) | 15.4 ± 2.03 (1–60) |
| Previous chemotherapy | |
| Yes | 8 (17.0%) |
| No | 39 (83.0%) |
| Previous radiotherapy | |
| Yes | 44 (93.6%) |
| No | 3 (6.4%) |
| Charlson comorbidity index | 2.5 ± 0.1 (2–5) |
| Body mass index | 28.9 ± 0.8 (18.7–45) |
| Prevalence (%)/Mean ± SEM | |
|---|---|
| Frailty criterion: Involuntary weight loss | Yes 11 (23.4%) |
| No 36 (76.6%) | |
| Frailty criterion: Weakness | Yes 5 (10.7%) |
| No 42 (89.3%) | |
| Frailty criterion: Low physical activity | Yes 15 (31.9%) |
| No 32 (68.1%) | |
| Frailty criterion: Slow gait speed | Yes 4 (8.5%) |
| No 43 (91.5%) | |
| Frailty criterion: Low muscle strength | Yes 10 (21.3%) |
| No 37 (78.7%) | |
| Cognitive functions | 28.3 ± 0.31 (range 22–30) |
| Activities of daily living (Barthel index) | 97.8 ± 0.5 (range 90–100) |
| Insomnia symptoms (Athens scale) | 2.9 ± 0.4 (range 0–9) |
| Depressive symptoms (Geriatric Depression Scale) | 1.7 ± 0.3 (range 0–9) |
| Nutritional assessment (MNA scale) | 26.9 ± 0.4 (range 20–30) |
| Hormones in Blood | Robust Patients (Mean ± Standard Deviation) | Prefrail/Frail Patients (Mean ± Standard Deviation) | p Values | Effect Size (Cohen’s d) |
|---|---|---|---|---|
| FSH (mUI/mL) | 43.6 ± 5.05 | 186.2 ± 48.2 | 0.013 | −0.628 |
| LH (mUI/mL) | 17.9 ± 2.2 | 79.03 ± 19.7 | 0.014 | −0.658 |
| Progesterone (ng/mL) | 0.07 ± 0.01 | 0.07 ± 0.005 | 0.7 | 0.003 |
| Estrone (pg/mL) | 24.9 ± 2.28 | 34.3 ± 2.5 | 0.02 | −0.72 |
| Estradiol (pg/mL) | 7.33 ± 0.9 | 7.68 ± 1.1 | 0.60 | −0.062 |
| Testosterone (ng/mL) | 0.21 ± 0.02 | 0.30 ± 0.03 | 0.06 | −0.548 |
| Dehydroepiandrosterone (ug/dL) | 103.2 ± 15.5 | 87.2 ± 9.54 | 0.50 | 0.285 |
| Androstenedione (pg/mL) | 123.8 ± 12.9 | 101.2 ± 11.6 | 0.15 | 0.367 |
| Dihydrotestosterone (ng/mL) | 0.151 ± 0.02 | 0.13 ± 0.01 | 0.54 | 0.271 |
| Aromatase activity index | 39.1 ± 4.6 | 31.4 ± 5.4 | 0.03 | 0.278 |
| Variables | p-Value | OR | 95% IC |
|---|---|---|---|
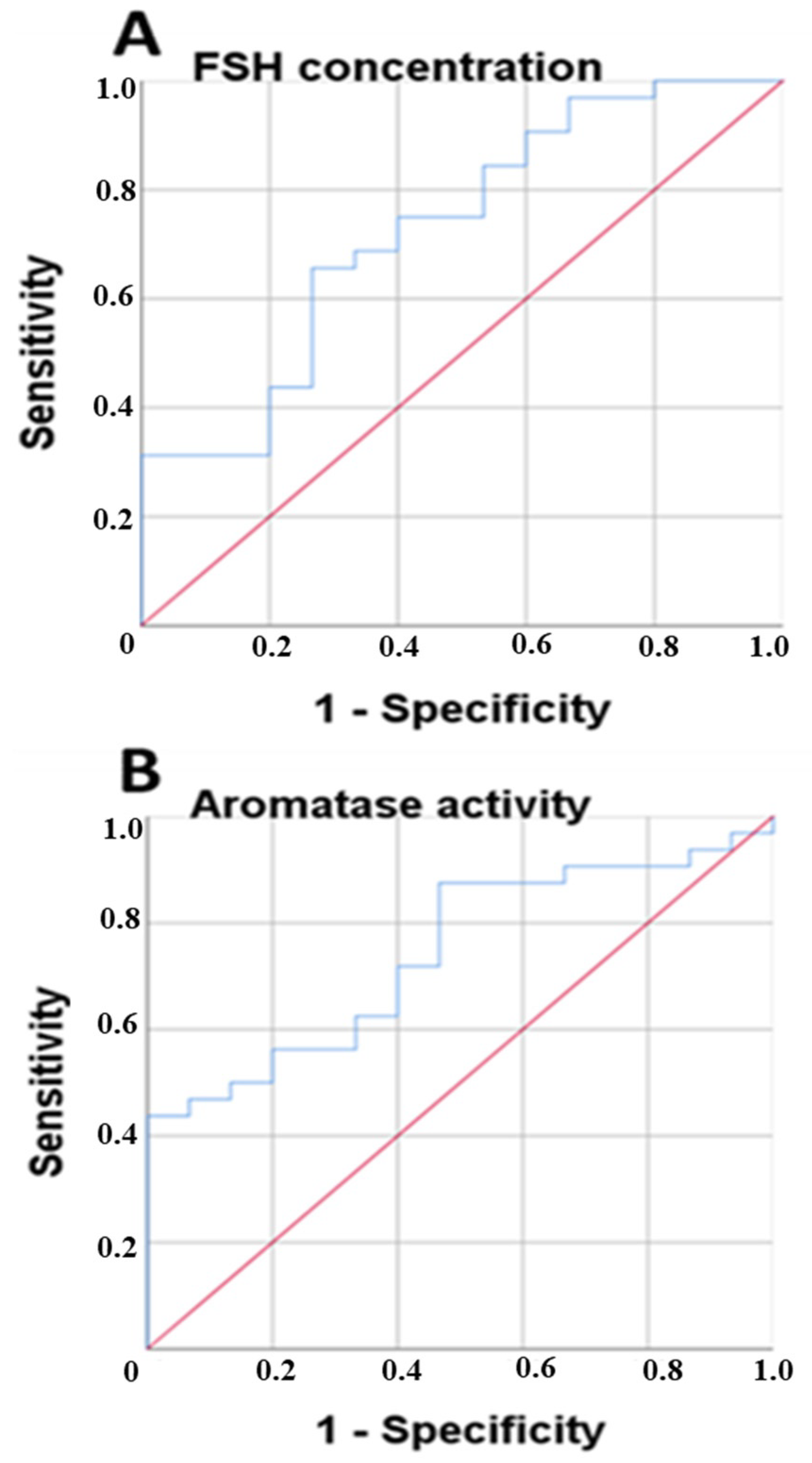
| Aromatase activity index | p = 0.043 | 0.951 | 0.839–0.989 |
| Estrone | p = 0.034 | 1.107 | 1.003–1.222 |
| Androstenedione | p = 0.169 | 0.990 | 0.975–1.004 |
| Age | p = 0.450 | 0.964 | 0.877–1.060 |
| FSH | p = 0.508 | 1.017 | 0.968–1.068 |
| LH | p = 0.657 | 1.019 | 0.938–1.106 |
| Previous chemotherapy treatment | p = 0.913 | 0.867 | 0.067–11.162 |
| Charlson comorbidity index | p = 0.657 | 1.387 | 0.328–5.865 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
García-Sánchez, J.; Mafla-España, M.A.; Tejedor-Cabrera, C.; Avellán-Castillo, O.; Torregrosa, M.D.; Cauli, O. Plasma Aromatase Activity Index, Gonadotropins and Estrone Are Associated with Frailty Syndrome in Post-Menopausal Women with Breast Cancer. Curr. Oncol. 2022, 29, 1744-1760. https://doi.org/10.3390/curroncol29030144
García-Sánchez J, Mafla-España MA, Tejedor-Cabrera C, Avellán-Castillo O, Torregrosa MD, Cauli O. Plasma Aromatase Activity Index, Gonadotropins and Estrone Are Associated with Frailty Syndrome in Post-Menopausal Women with Breast Cancer. Current Oncology. 2022; 29(3):1744-1760. https://doi.org/10.3390/curroncol29030144
Chicago/Turabian StyleGarcía-Sánchez, Javier, Mayra Alejandra Mafla-España, Carlos Tejedor-Cabrera, Olga Avellán-Castillo, María Dolores Torregrosa, and Omar Cauli. 2022. "Plasma Aromatase Activity Index, Gonadotropins and Estrone Are Associated with Frailty Syndrome in Post-Menopausal Women with Breast Cancer" Current Oncology 29, no. 3: 1744-1760. https://doi.org/10.3390/curroncol29030144