 Danielle Toccalino1,2*
Danielle Toccalino1,2* Amy Moore3
Amy Moore3 Elizabeth Cripps3
Elizabeth Cripps3 Sophia Chuon Gutierrez4
Sophia Chuon Gutierrez4 Angela Colantonio2,5,6,7,8
Angela Colantonio2,5,6,7,8 Christine M. Wickens1,8,9,10,11
Christine M. Wickens1,8,9,10,11 Vincy Chan1,2,5,7
Vincy Chan1,2,5,7 Emily Nalder5,6,7
Emily Nalder5,6,7 Halina (Lin) Haag2,3
Halina (Lin) Haag2,3- 1Institute of Health Policy, Management and Evaluation, University of Toronto, Toronto, ON, Canada
- 2Acquired Brain Injury Research Lab, University of Toronto, Toronto, ON, Canada
- 3Lyle S. Hallman Faculty of Social Work, Wilfrid Laurier University, Waterloo, ON, Canada
- 4Faculty of Kinesiology and Physical Education, University of Toronto, Toronto, ON, Canada
- 5KITE-Toronto Rehabilitation Institute, University Health Network, Toronto, ON, Canada
- 6Department of Occupational Science and Occupational Therapy, Temerty Faculty of Medicine, University of Toronto, Toronto, ON, Canada
- 7Rehabilitation Sciences Institute, Temerty Faculty of Medicine, University of Toronto, Toronto, ON, Canada
- 8Dalla Lana School of Public Health, University of Toronto, Toronto, ON, Canada
- 9Institute for Mental Health Policy Research, Centre for Addiction and Mental Health, Toronto, ON, Canada
- 10Campbell Family Mental Health Research Institute, Centre for Addiction and Mental Health, Toronto, ON, Canada
- 11Department of Pharmacology and Toxicology, University of Toronto, Toronto, ON, Canada
Rationale: Intimate partner violence (IPV) is the most commonly occurring form of violence against women. The most common site of injury in IPV is the head, face, and neck, resulting in possible brain injury (BI). Independently, mental health (MH) concerns are highly prevalent among both IPV survivors and individuals with BI; however, no systematic review exists on the combined experience of BI and MH in IPV.
Objective: The aim of this review was to describe the identification of and relationships between BI, MH, and IPV in the literature and the implications for health policy and practice.
Methods: A search strategy including text words and subject headings related to BI, IPV, and MH was developed for MEDLINE and translated to EMBASE, PsycINFO, CINAHL, Cochrane, Scopus, and Web of Science. Two reviewers independently assessed articles for inclusion. Articles discussing MH, BI, and IPV in relation to one another were included in the review.
Results: Twenty-eight articles were identified for inclusion. Methods for identifying IPV, BI, and MH were highly variable across studies. Fourteen studies reported significantly higher MH scores in IPV survivors with BI than in those without BI. Articles predominantly focused on cis gender women in heterosexual relationships and the impact of race and ethnicity were largely overlooked. Healthcare access was explored by eight articles, though none discussed the implications of co-occurring BI and MH.
Conclusion: Brain injury and MH are highly prevalent among IPV survivors; however, little research discusses the implication for healthcare. Future research should explore healthcare-related needs and experiences to inform policy and practice and better represent the diversity of IPV survivors.
1. Introduction
Recent estimates suggest 44% of women and 36% of men will experience intimate partner violence (IPV) in their lifetime, more than half of whom will experience physical violence (1). Intimate partner violence has been defined as physical, psychological, or sexual violence committed by an intimate partner or ex-partner and can result in significant emotional and bodily harm (2). Individuals of all genders and sexual orientations experience IPV; however, most research has focused on women survivors of IPV. Women experience higher rates and more severe forms of IPV than men, including higher rates of strangulation (1), and IPV is the most commonly experienced form of violence women experience (3, 4). For the purposes of this review, we also include individuals working in sex work or prostitution under the umbrella of IPV. An estimated 45–81% of sex workers experience violence from their clients and many also experience violence from another intimate partner (5, 6).
The COVID-19 pandemic has exacerbated IPV globally, significantly increasing both rates of IPV and the level of violence per encounter (7–11). Physical violence in IPV most commonly results in injury to the head, face, and neck (12), leaving survivors at high risk of traumatic brain injury (TBI). TBI is “an injury to the brain producing an alteration in brain function, or other evidence of brain pathology, caused by an external force” (13). Strangulation, also commonly experienced during IPV (1, 14), can result in hypoxic-ischemic brain injury due to a lack of blood circulation and consequently oxygen and nutrients to the brain (15, 16). Both hypoxic-ischemic and traumatic brain injuries have been included in this review under the umbrella of brain injury (BI), as the context of IPV similarly informs treatment and recovery challenges for both injuries (17–19).
Brain injuries from any cause can have significant long-term cognitive, psychiatric, physical, and social consequences (20–23). Previous research indicates a high prevalence of BI among IPV survivors (14, 24), suggesting a significant need for more attention to IPV-related BI. However, lack of awareness, gaps in screening, and unique challenges in healthcare access often leave BI overlooked in IPV survivors, hindering identification and support (14, 17). Identification of IPV-related BI is further challenged by the high correlation between symptoms and sequelae of BI and symptoms of mental health (MH) concerns that are also commonly experienced by survivors (25–31). A recent Lancet Psychiatry Commission report focused on the intersection of IPV and MH noted the elevated risk of MH concerns among IPV survivors and the heightened risk of IPV among individuals, specifically women, with MH concerns (32). However, the report made no mention of head injury or BI of any kind, which is suggestive of the work still to be done in recognizing the triple intersection of IPV, MH concerns, and BI. The correlation between BI symptoms and MH concerns makes differential diagnosis difficult and further complicates the provision of and access to adequate and appropriate healthcare (25, 33). The interaction between BI and MH concerns can impact care and treatment for the BI, MH concern, or both. For example, a BI can amplify the symptoms of post-traumatic stress disorder (PTSD), anxiety, or depression, making these MH concerns more difficult to treat if the underlying BI goes unaddressed (27, 33). Furthermore, treatment for MH concerns may be more effective when accommodations are made for potential difficulties with emotion regulation, impulse control, pain, and cognitive limitations that can accompany BI (30).
Despite the high rates of both BI and MH concerns among survivors of IPV and the high rates of MH concerns among individuals with BI, the literature investigating the co-occurrence and combined experience of BI and MH concerns among survivors of IPV (triple intersection) is limited, and there has not yet, to our knowledge, been a comprehensive review investigating the intersection of BI and MH concerns among IPV survivors. An investigation into the triple intersection is needed as most of the research currently informing BI guidelines is based on predominantly male samples injured through other mechanisms (e.g., sports, military service).
This scoping review was developed to explore what is known in the literature about MH concerns and BI among survivors of IPV. Specifically, it aimed to summarize and synthesize the existing literature through the following objectives: (1) describe how IPV, BI, and MH concerns are identified in the literature and (2) describe the relationships between IPV, BI, and MH concerns. BI is often overlooked in IPV survivors with significant health implications, and MH concerns further complicate healthcare provision and access. Therefore, a third objective was to identify the implications for healthcare and health systems to inform policy and practice.
2. Methods
This scoping review looked at MH concerns and BI among survivors of IPV as reported in the published literature since the inception of the searched databases. The review was designed following the framework first developed by Arksey and O'Malley (34) and further developed by JBI, formerly the Joanna Briggs Institute (35, 36). Reporting was guided by the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) Checklist (37). The search strategy and eligibility criteria were informed by a previous scoping review investigating BI among survivors of IPV (14). Search terms for MH concerns were informed by a previous systematic review investigating MH and BI (38, 39) and by the literature exploring MH implications of both BI and IPV (14, 25–28, 40–43).
2.1. Search strategy
MEDLINE, EMBASE, PsycINFO, CINAHL, Cochrane, Scopus, and Web of Science were searched for relevant articles using a search strategy including text words and subject headings (e.g., MeSH, Emtree) related to BI, IPV, and MH. The search was initially run in October 2020 and revised and updated in January 2022 using concepts broadly characterized as follows:
1. Brain injury: Traumatic brain injury, concussion, head injury, post-concussion syndrome, strangulation, choking, face injury, and neck injury.
2. Intimate partner violence: Domestic violence, spousal abuse, spouse abuse, intimate partner violence, interpersonal violence, battered women, intimate violence, and sex work.
3. Mental health: Post-traumatic stress disorder, anxiety, depression, bipolar and related disorders, mood disorders, obsessive-compulsive disorder, phobias, substance use disorder, drug abuse, and alcohol abuse.
Sex workers are often excluded from IPV; however, there are many similarities in the violent encounters experienced by sex workers and IPV survivors. As such, previous reviews have chosen to include both IPV and sex work terms in their search (14), which we mirror in this review. For the complete search strategy, refer to Appendix A.
Searches were not limited by language, year of publication, or geographic location. Returned records were managed in EndNote and Covidence (44). A manual search of the reference lists of each article meeting the full-text inclusion criteria as well as any identified review articles discussing BI, MH concerns, and IPV was conducted to identify additional literature not captured in the original search.
2.2. Eligibility criteria: Title and abstract screen
Following the removal of duplicates, two reviewers (DT and either AM, SCG, or EC) independently assessed all identified titles and abstracts for eligibility. This screen focused on identifying primary research studies, including theses or dissertations, and review articles addressing BI among IPV survivors, MH concerns among IPV survivors, or IPV among individuals with BI. This broad approach was taken based on previous experience with reviews on BI suggesting that all relevant subgroups (in this case, IPV, MH, and BI) are not always included in the abstract, though relevant data may be presented in the body of the article. Articles were excluded if they focused on the perpetrator, on populations younger than 18 years of age, or on violence outside of the context of an intimate partner relationship. Conference abstracts, protocols, books or book reviews, and animal studies were also excluded. Covidence software was used for screening and to monitor agreement between the reviewers' assessments (87–94% agreement between pairs). Differences were resolved through discussion and consensus; articles were moved to the full-text screen if consensus could not be reached.
2.3. Eligibility criteria: Full-text screen
Full texts were again reviewed independently by two reviewers (DT and either AM, SCG, or EC). For inclusion in the review, studies needed to specifically discuss MH concerns and BI in survivors of IPV, be written in English, and be available through the University of Toronto Library system. Exclusion criteria used for the abstract and title screen continued to apply. In addition, articles were excluded if they were commentaries or if they did not discuss MH, BI, and IPV in relation to one another (e.g., discussing MH and BI separately). As with the title and abstract screen, Covidence software was used to conduct the screening and monitor agreement between the reviewers' assessments (80–96% agreement between pairs). All differences in screening were resolved through discussion and consensus.
2.4. Data extraction and synthesis
Study details (i.e., location, design, population, sample size, data source, definitions for IPV, BI, and MH) and key findings (prevalence of IPV, BI, and MH; healthcare use; relationships between IPV, BI, and MH) were extracted from included studies as reported. Data were extracted by one reviewer and peer-reviewed by a second (DT and AM or EC) then synthesized using narrative synthesis (45).
3. Results
Searching the seven databases returned 753 results and 563 unique records following duplicate removal. From this body of literature, a total of 28 articles reporting on 27 studies (including three theses) were included. For a comprehensive breakdown of the article review process, please refer to Figure 1.
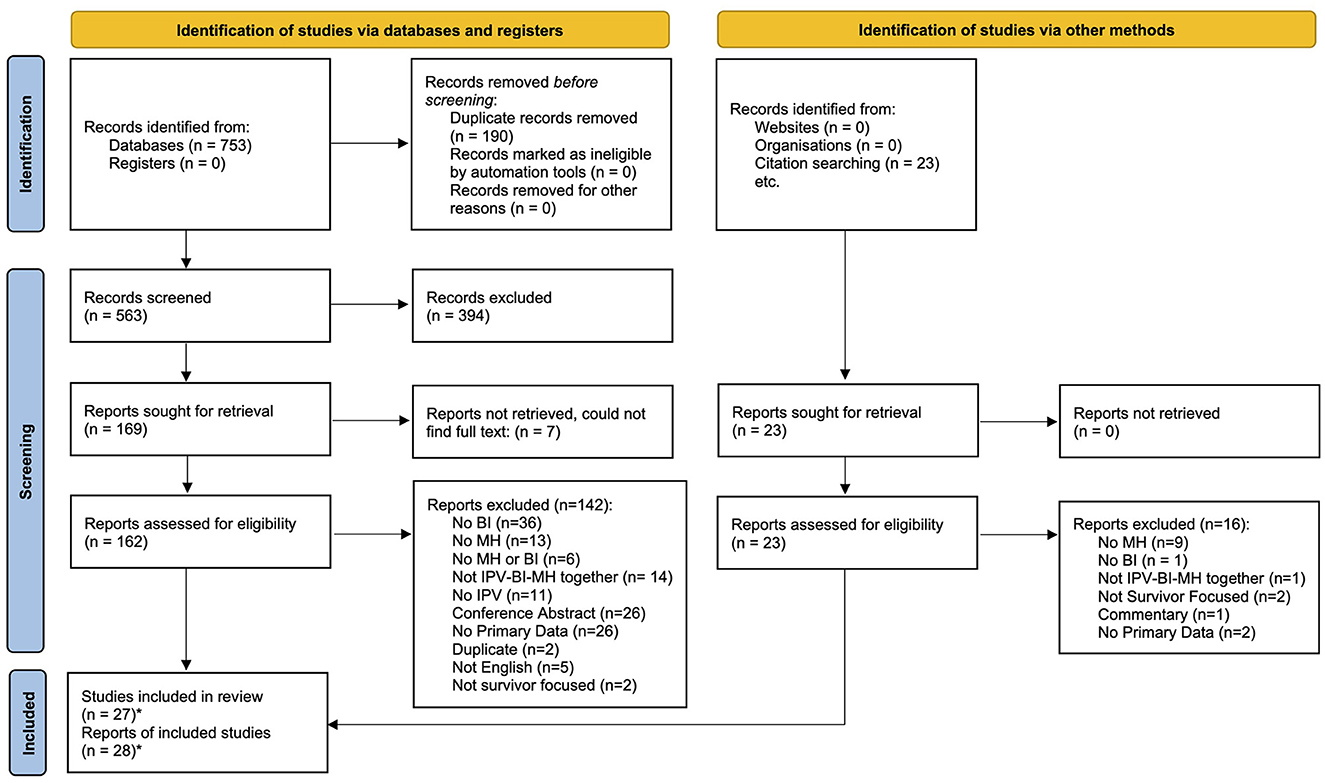
Figure 1. PRISMA 2020 flow diagram for new systematic reviews which included searches of databases, registers and other sources. *Two of the included articles reported on the same study, resulting in 28 total articles being included reporting on the findings from 27 studies. From Page et al. (46).
3.1. Article characteristics and study populations
Articles were predominantly published in the last 5 years (61%, n = 17) and based on data from the United States (US; 82%, n = 23). Study populations consisted almost exclusively of women or female survivors, with a few noted exceptions. Three studies included male survivors in their sample, accounting for 3–10% of the study populations (47–49). Gabbe et al. (50) found 27% of major trauma patients presenting with TBI caused by IPV-related violence were male. While both male and female survivors were included in these studies, sex- or gender-specific findings were not reported, though small sample sizes were likely prohibitive of that reporting. Four studies specifically reported on the sex or gender of the perpetrator, all specifying males or men as perpetrators (51–54). One additional study noted the study population as heterosexual women (55).
Two studies specifically explored the experiences of Black or African American women (56, 57), and one study focused on the experiences of Chinese women (58). The remainder of the studies had variable reporting on race or ethnicity. Four articles reported on the percentage of participants that were non-white (ranging from 4 to 62% stratified by BI status) (27, 59, 60) or from a visible minority (13%) (61). Five articles reported on the number of participants who were Black/African American or white with the remainder in a mixed race or other categories (40, 52, 55, 62, 63). Nine articles reported on all groups represented in the sample (10, 43, 47, 49, 51, 54, 64–66), and seven articles did not report race or ethnicity at all (48, 50, 53, 67–70). Among studies where race or ethnicity was not an inclusion criterion, white (n = 14 studies, 8–75%), African American/Black (n = 13, 13–90%), and Latina/Hispanic (n = 6, 1–16%) were the most commonly reported groups. Some studies controlled for sociodemographic factors (including race or ethnicity) in their analyses; however, none reported race- or ethnicity-specific findings.
Though the search terms were broadened to include sex work, none of the included studies focused on or included individuals who participate in sex work or prostitution. However, the inclusion of strangulation in our search terms was mirrored to a large extent in the literature. Although most articles referred to TBI, 15 of the 28 included articles (54%) included strangulation in their definition of TBI. In addition, five articles focused specifically on strangulation (51, 54, 55, 66, 69). One of these articles, reporting on findings from a broader study investigating BI (43), specifically looked at strangulation-related alterations in consciousness (66); however, three of the remaining four articles reported high rates of loss of consciousness or dizziness among their study participants, indicative of a potential BI (51, 54, 69). For article summaries, refer to Table 1.

Table 1. Summary of included articles.
3.1.1. Identifying intimate partner violence (IPV)
Experience of IPV was an inclusion criterion for almost all included studies, with one exception: Gabbe et al. (50) looked at rates of IPV among violence-related TBI, reporting an annual incidence of 0.11/100,000. Most studies identified survivors of IPV either through recruitment sites (e.g., women's shelters; 37%, n = 11) or via self-report of abusive relationships (24%, n = 7) with recruitment through a variety of sites. The remainder identified IPV using screening tools, with the most common being the Conflict Tactics Scale (CTS, n = 6) (43, 56, 58, 60, 65, 71). Additional tools included the Humiliate/Afraid/Rape/Kick tool (HARK tool, n = 2) (27, 59) and the Women's Experiences of Battering (n = 2) (55, 61).
While most studies included individuals who had experienced IPV at any point in their lifetime, there were several studies that required IPV within a certain timeframe. Four studies assessed for IPV within the last year (27, 51, 58, 60), Mittal et al. (55) required IPV within the last 3 months, and Saleem et al. (49) required an incident of physical IPV within the past 60 days. Two studies required participants to have presented to the recruitment site (emergency department and family advocacy center) with IPV-related injuries (48, 58).
3.1.2. Assessing for brain injury (BI)
Identification of BI varied greatly across studies. In most instances, studies assessed for possible or probable BI by asking about instances of hits to the head, face, or neck followed by a period of altered or loss of consciousness, or by asking about instances of strangulation or choking. More than half of the included studies (n = 15) assessed for BI using screening tools or diagnostic interviews, with the Boston Assessment of TBI (62, 63, 67), Brain Injury Severity Assessment (61, 66, 68), and Veterans Affairs TBI screening tool (27, 59, 60) the most commonly used in three studies each. Gabbe et al. (50) used diagnostic codes to identify TBI in a health administrative dataset and Brown et al. (47) identified survivors with electrophysiological similarity to TBI via EEG. Three of the five studies focusing on strangulation simply asked if or how frequently survivors had been choked and/or strangled (51, 54, 55). The remainder of the studies assessed for BI using self-report that was not further specified. Some studies specifically excluded individuals with more severe BI (58, 66) or BI that was not IPV related (43, 49, 57, 66) and a subset of studies reported on BI from other causes in addition to IPV-BI (61, 62, 64, 66, 67).
As previously noted, most articles discussed BI broadly, including both TBI and strangulation (n = 15). Some focused on TBI specifically (n = 8), and others focused on strangulation (n = 5). Table 1 shows included articles stratified by these categories. Several studies in each category had BI as an inclusion criterion (40, 48, 50, 51, 53, 59, 69). Among studies where BI was not an inclusion criterion, the prevalence of strangulation ranged from 13 (56) to 93% (49), the prevalence of BI ranged from 19 (60) to 100% (68), and the prevalence of TBI ranged from 21 (64) to 69% (47). There was also a noted relationship between BI and IPV scores or experiences. Mittal et al. (55) reported significantly higher scores on two IPV scales among women who were strangled compared to women who were not, and Wong et al. (58) reported a significant association between past-year psychological (but not physical or sexual) abuse and IPV-related mild TBI.
3.1.3. Assessing for mental health (MH) concerns
Of the 28 included articles, most either investigated anxiety, depression, and PTSD together (40, 43, 47, 57, 59, 61, 64, 66, 68) or MH as a broad concept (i.e., type of MH was not specified) (10, 48, 50, 51, 58, 69). Among the 17 articles measuring PTSD, the most commonly used measures were the Clinician administered PTSD scale (CAPS, n = 7) (43, 61–63, 66–68) and the Post-traumatic Stress Disorder Checklist (PCL, n = 5) (27, 59, 60, 62, 63), with two studies using the PCL to screen for PTSD and the CAPS to diagnose (62, 63). Assessment of both depression and anxiety was much more varied. Four of the 15 studies measuring depression used the Center of Epidemiologic Studies Depression Scale (55, 56, 59, 60). Three studies used the Beck Depression Inventory and Beck Anxiety Inventory to measure depression and anxiety, respectively (61, 64, 68), and two studies reported on anxiety and depression based on the HELPS tool, reporting “problems because of a hit to the head or due to strangulation” (49, 70). Though included in our search terms, only three studies reported substance use (49, 52, 61). Full reporting on measures used can be found in Table 1.
3.2. Experiences of BI and MH concerns in survivors of IPV
All studies in this review specifically discussed MH, BI, and IPV in relation to one another, allowing us to explore the intersectional impact of MH concerns and BI among IPV survivors. All but three of the 28 included articles reported on MH concerns among survivors of IPV with BI. Those three looked at rates of IPV among individuals with BI, reporting on MH prevalence within that subset (50); and rates of BI among survivors of IPV with positive screen and diagnosis of PTSD, respectively (62, 63).
Prevalence of MH among individuals who had experienced IPV and BI was reported in 13 studies, with depression ranging from 25 to 86% across nine studies (40, 49, 52, 54, 57, 61, 64, 68, 70), anxiety ranging from 32 to 100% across eight studies (40, 49, 54, 57, 61, 64, 68, 70), and PTSD ranging from 29 to 100% across six studies (27, 40, 61, 64, 65). Two studies reported the prevalence of MH as a broader category, ranging from 32 to 41% (48, 50). Finally, two studies reported the prevalence of substance use ranging from 28 to 33% (49, 61).
Relationships between BI and MH concerns among IPV survivors were also explored in 14 studies. Studies reported statistically significant differences in PTSD scores (27, 56, 57, 60, 64–67), depression scores (55, 60, 66), anxiety scores (57), or composite mental health scores (56, 58) among IPV survivors with BI compared to those without. Two studies compared MH scores with BI severity scores rather than grouping survivors with and without BI, both reporting significant positive associations between BI and MH scores (43, 47). Furthermore, the presence of BI was noted to negatively impact outcomes in PTSD treatment (63), and persistent BI symptoms were associated with lingering insomnia, depression, and physical health concerns (59). McFadgion (65) also reported that IPV survivors who experienced post-traumatic stress symptoms were more likely to experience a blow to the head from physical abuse. Two qualitative studies exploring experiences of BI among survivors of IPV noted MH concerns were often exacerbated following physical abuse (51) and negatively impacted by the COVID-19 pandemic (10). It was further noted that survivors often continued to experience MH concerns even after leaving the abusive relationship (51).
3.3. Healthcare use and access
Many studies identified implications for health and healthcare among IPV survivors with BI and MH; however, less than half investigated healthcare use or access. Seven studies used healthcare settings for some or all their participant recruitment (50, 54–56, 58, 60, 69), two of which also reported healthcare seeking (54, 69). An additional five studies reported the number of survivors who sought healthcare because of IPV (40, 51, 52, 64, 70). One article specifically compared health service use among IPV survivors with and without BI, reporting significantly higher Veterans Affairs healthcare use among women veteran IPV survivors with BI than those without (60). Studies reported 18–62% of survivors received care for an IPV-related injury at some point following the abuse (40, 51, 52, 54, 64, 69, 70). A qualitative exploration of care seeking identified fear of the abuser and a reluctance to discuss the experience of IPV as barriers (51).
4. Discussion
This review identified 28 trail-blazing articles discussing BI and MH concerns among survivors of IPV. Studies focused on cis gender women in relationships with men and were predominantly conducted in the US. Overall, the prevalence of BI (strangulation, TBI, or both) among IPV survivors ranged from 13 to 93%, which is in line with previous estimations (14). The prevalence of MH concerns among IPV-BI survivors, which has not previously been assessed in a review, ranged from 25 to 100%. Studies used a wide range of methods for identifying IPV, MH, and BI, including via recruitment settings, single self-report questions, validated questionnaires, and medical diagnoses. These differences are likely to contribute to the large ranges in prevalence seen across studies.
Many studies reported significant differences in MH scores between IPV survivors with BI compared to those without or significant correlations between BI and MH scores. Though only explored in two studies, BI was shown to negatively impact PTSD treatment outcomes and both physical and mental health. The prevalence of healthcare seeking was explored in a subset of studies, ranging from 18 to 62% among studies that did not recruit solely from healthcare sites. One of those studies reported higher care use among IPV survivors with BI than those without (60). Fear of the abuser and a reluctance to discuss the experience were noted as barriers to accessing care (51).
This review highlights the small but growing pool of foundational work on the intersection of MH concerns and BI among IPV survivors, underscoring the high prevalence of co-occurring MH and BI among IPV survivors and identifying opportunities for future exploration, including the investigation into the healthcare-related impacts of this intersection on survivors and the health system. The high rate of BI among survivors combined with the higher severity of MH associated with BI indicates this is a significant intersection for investigation not only for healthcare systems but also for community care systems and society at large. As much is still unknown about this intersection, four broad categories in need of further investigation are highlighted below.
4.1. Identification
Defining and screening for BI among IPV survivors is an ongoing debate in the IPV-BI literature (14, 48, 72). While loss of consciousness is a strong indicator of BI, more subtle alterations of consciousness (e.g., feeling dazed, confused, seeing stars) are also indicative of BI (56) but may not be captured depending on the way questions are worded and the survivor's memory of the incident. Given that almost all the included studies relied on survivor self-report, and the measures used varied from asking about specific injuries resulting in loss of consciousness to any injury resulting in the alteration of consciousness, it is likely that even when using BI screening measures, BIs are missed among IPV survivors. Several studies reported on BI both as identified via screening tools and as identified through questions about hits to the head with alterations in or loss of consciousness. In some cases, the prevalence using the latter method was double that of the former.
It is worth noting that the identification of IPV, particularly in healthcare settings, poses its own challenges. In addition to the challenges with IPV survivors not wanting or being able to seek treatment noted in the included literature, there are also challenges with the identification and disclosure of IPV when survivors do seek care. Medical professionals may be reluctant to broach the topic for reasons including lack of training or resources to do so or a belief that IPV is beyond their scope of practice. This, combined with a survivor's reluctance to disclose, can impede identification of IPV, impacting professionals' ability to adequately support survivors.
4.2. Sex and gender
The studies included in this review focused predominantly on cis gender women in relationships with men. However, there were inconsistencies throughout the included studies in referring to survivors as women, which aligns with the social construct of gender, and as females, which aligns with physiological sex. Similar inconsistencies were found in the reporting of partner sex and/or gender. As the experience of BI is influenced by both sex and gender (73–75), and IPV impacts individuals across the gender spectrum, there is an opportunity in this growing field to explore experiences of BI and MH concerns across IPV survivors of all genders and sexes.
4.3. Healthcare seeking
Included articles that explored healthcare predominantly focused on whether or not women sought medical help, rather than survivors' self-perceived health needs or how comorbid conditions shaped their care-seeking. The experience of care seeking, whether through medical or community routes, and perceived care needs is an opportunity for exploration. Several articles provided recommendations for healthcare providers in their discussions; the field would benefit from an investigation of how survivors experienced healthcare or other services that could further develop those recommendations. This call is echoed in the literature, identifying the triple intersection as needing more focus particularly because MH that is comorbid with BI, both in IPV survivors and the broader population, requires different considerations for care and treatment than MH alone, and vice versa (31, 76–78).
An additional consideration in the discussion of care-seeking is the healthcare and social context in which the study was conducted. Only five of the included articles were conducted outside of the US (10, 50, 58, 61, 68). While there are many aspects of the lived experience of BI, IPV, and MH that are universal, context also plays a role. Financial accessibility of healthcare has implications for care-seeking. More research in diverse contexts with different healthcare systems, including systems with universal healthcare, would support a more complete understanding of survivor needs and experiences. The one study reporting on healthcare use among IPV survivors with BI found increased Veterans Affairs healthcare use, which is funded for US veterans (60). Further investigation of the experiences of IPV-related BI and MH in contexts outside of the US will be critical for shaping the response to this “parallel pandemic” of COVID-19 and IPV, particularly when it comes to healthcare or service access and use. For example, in April 2020, the Government of Canada acknowledged IPV as a critical problem, exacerbated by COVID-19, and invested $207.5 million to support organizations addressing homelessness and women experiencing gender-based violence (79). Given the system-wide barriers and challenges identified with respect to the IPV-BI intersection overall (80), more research in this area could help target future investments to the areas with the greatest impact.
4.4. Intersectional representation
Throughout the literature included in this study, the intersection of other aspects of identity, such as race, ethnicity, ability, or immigration status, and the impacts of MH and BI among IPV survivors remains largely unexplored. Three studies focused on the experiences of specific ethnic groups (56–58) and one case report discussed the experiences of two refugees identifying as IPV survivors with BI (53); however, only one of the cases explored the triple intersection. A more thorough look into the impact of intersecting identities is needed as there are increased risks and differing care needs for these groups. For example, Indigenous women are at particularly high risk for IPV, reporting 2.5 times higher rates of violence and a higher rate of resultant injury (81), yet preliminary work in the IPV-BI intersection working with Indigenous groups in Canada (82) suggests that resources developed for urban settler populations are ineffective for many First Nations and Inuit communities for myriad reasons. A collaborative, Indigenous-led approach to developing culturally sensitive community-based resources and interventions is needed to support Indigenous survivors and their communities.
4.5. Strengths and limitations
This scoping review is the first, to the best of our knowledge, exploring the combined experience of IPV, BI, and MH. It provides insight into the prevalence of BI and MH among IPV survivors; identifies the wide variety of methods used to identify BI, MH, and IPV; and synthesizes the relationships between them as currently understood in the literature. The review used a comprehensive and purposefully broad search strategy across five databases that were not limited by date or language, maximizing the published literature captured in the initial search. The two-stage, systematic screening process, as well as the high proportion of agreement among reviewers, further minimized the risk of excluding relevant articles.
We acknowledge several limitations to this review. While the search was not limited by language, we were not able to review full-text articles in languages other than English, resulting in the exclusion of five articles at the full-text stage (3% of articles reviewed). In addition, any unpublished literature, reports, or briefs that may be present in gray literature were not captured in our search. Including gray literature has the noted benefit of providing a more comprehensive overview of available evidence on a subject; but, its inclusion poses a significant challenge in the increased human resources required to find, manage, and review these records (83). Unfortunately, due to resource limitations, a systematic search of the gray literature was not possible. Finally, we recognize that the findings presented are limited by the included literature, which predominantly used small (N < 50) convenience samples. It can be challenging to engage IPV survivors in research for a variety of reasons including willingness to disclose and safety concerns. Furthermore, many of the studies recruited through shelters and related domestic violence support centers, which impacts the type of individuals captured in the research.
4.6. Latest contributions
The literature focusing on the triple intersection is growing rapidly, as indicated by the majority of the included articles being published in the last 5 years. In the time between running our last database search and the publication of this review, we are aware of the publication of three additional articles reporting on the triple intersection. Chiou et al. (84) investigated depression severity in a subsample of IPV-BI survivors explored in another article included in this review (70), finding 64% of their participants endorsing moderate to severe depression based on the Beck Depression Inventory. Oakley et al. (85) assessed the willingness of IPV survivors to be screened for BI, with 88% of their sample screening positive for probable TBI on the HELPS tool. Among the sample with a positive TBI screen, 89 and 78% reported depression and anxiety, respectively. Finally, Quiroz Molinares et al. (86) explored BI among Colombian women survivors of IPV, finding 31% experienced BI and a significant correlation between BI score and depression when controlling for abuse severity and various socioeconomic factors. The findings from these articles align with those reported in the review.
5. Conclusion
This review highlighted the foundational and growing pool of literature on the triple intersection of IPV, BI, and MH and draws attention to the numerous opportunities for future work, such as increasing our understanding of BI and MH among IPV survivors, better representing the diversity of individuals experiencing IPV, and exploring service-related needs and experiences to inform policy and practice.
Data availability statement
All data analyzed as part of this scoping review is from publicly available published literature.
Author contributions
This study was conceptualized by DT, HLH, AC, and CMW in consultation with EN and VC. DT developed the search strategy, ran the database searches finalized analyses, and drafted the manuscript. DT, AM, EC, and SCG conducted screening and contributed to the analyses. All authors contributed to the manuscript revision, read, and approved the submitted version.
Funding
DT and HLH were supported by a grant from the Ontario Neurotrauma Foundation and the Ontario Women's Health Scholar Award. This research was undertaken, in part, thanks to funding from the Canada Research Chairs Program.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1100549/full#supplementary-material
References
1. Cotter A. Intimate Partner Violence in Canada, 2018: An Overview. Statistics Canada: Canadian Centre for Justice and Community Safety Statistics. St Louis: Canadian Centre for Justice Statistics (2021).
3. Conroy S, Burczycka M, Savage L. Family Violence in Canada: A Statistical Profile, 2018. Ontorio: Canadian Centre for Justice Statistics (2019).
4. World Health Organization. Understanding and Addressing Violence against Women. Geneva: World Health Organization (2012).
5. Baumann RM, Hamilton-Wright S, Riley DL, Brown K, Hunt C, Michalak A, et al. Experiences of violence and head injury among women and transgender women sex workers. Sexual Res Soc Policy. (2019) 16:278–88. doi: 10.1007/s13178-018-0334-0
6. Farley M, Banks ME, Ackerman RJ, Golding JM. Screening for traumatic brain injury in prostituted women. Dignity J Sex Exploit Viol. (2018) 3:5. doi: 10.23860/dignity.2018.03.02.05
7. Campbell AM. An increasing risk of family violence during the COVID-19 pandemic: strengthening community collaborations to save lives. For Sci Int Rep. (2020) 2:100089. doi: 10.1016/j.fsir.2020.100089
8. Matoori S, Khurana B, Balcom MC, Koh D-M, Froehlich JM, Janssen S, et al. Intimate partner violence crisis in the COVID-19 pandemic: how can radiologists make a difference? Eur Radiol. (2020) 30:6933–6. doi: 10.1007/s00330-020-07043-w
9. Valera EM. When pandemics clash: gendered violence-related traumatic brain injuries in women since COVID-19. EClinicalMedicine. (2020) 24:423. doi: 10.1016/j.eclinm.2020.100423
10. Haag HL, Toccalino D, Estrella M, Moore A, Colantonio A. The shadow pandemic: a qualitative exploration of the impacts of COVID-19 on service providers and women survivors of intimate partner violence and brain injury. J Head Trauma Rehabil. (2022) 37:43–52. doi: 10.1097/HTR.0000000000000751
11. Toccalino D, Haag H, Estrella M, Cowle S, Fuselli P, Ellis M, et al. Addressing the shadow pandemic: COVID-19 related impacts, barriers, needs, and priorities to healthcare and support for women survivors of intimate partner violence and brain injury. Arch Phys Med Rehabil. (2022) 103:1466–76. doi: 10.1016/j.apmr.2021.12.012
12. Sheridan DJ, Nash KR. Acute injury patterns of intimate partner violence victims. Trauma Viol Abuse. (2007) 8:281–9. doi: 10.1177/1524838007303504
13. Menon DK, Schwab K, Wright DW, Maas AI. Position statement: definition of traumatic brain injury. Arch Phys Med Rehabil. (2010) 91:1637–40. doi: 10.1016/j.apmr.2010.05.017
14. Haag HL, Jones D, Joseph T, Colantonio A. Battered and brain injured: traumatic brain injury among women survivors of intimate partner violence—a scoping review. Trauma Viol Abuse. (2019) 23:1270–87. doi: 10.1177/1524838019850623
15. Arciniegas DB. Hypoxic-ischemic brain injury: addressing the disconnect between pathophysiology and public policy. NeuroRehabilitation. (2010) 26:1–4. doi: 10.3233/NRE-2010-0530
16. Howard RS, Holmes PA, Koutroumanidis MA. Hypoxic-ischaemic brain injury. Pract Neurol. (2011) 11:4–18. doi: 10.1136/jnnp.2010.235218
17. Campbell JC, Anderson JC, McFadgion A, Gill J, Zink E, Patch M, et al. The effects of intimate partner violence and probable traumatic brain injury on central nervous system symptoms. J Womens Health. (2018) 27:761–7. doi: 10.1089/jwh.2016.6311
18. Cullen NK, Weisz K. Cognitive correlates with functional outcomes after anoxic brain injury: a case-controlled comparison with traumatic brain injury. Brain Injury. (2011) 25:35–43. doi: 10.3109/02699052.2010.531691
19. Colantonio A, Valera EM. Brain injury and intimate partner violence. J Head Trauma Rehabil. (2022) 37:2–4. doi: 10.1097/HTR.0000000000000763
20. Ilie G, Adlaf EM, Mann RE, Boak A, Hamilton H, Asbridge M, et al. The moderating effects of sex and age on the association between traumatic brain injury and harmful psychological correlates among adolescents. PLoS ONE. (2014) 9:e108167. doi: 10.1371/journal.pone.0108167
21. Mansfield E, Stergiou-Kita M, Cassidy JD, Bayley M, Mantis S, Kristman V, et al. Return-to-work challenges following a work-related mild tbi: the injured worker perspective. Brain Injury. (2015) 29:1362–9. doi: 10.3109/02699052.2015.1053524
22. Hwang SW, Colantonio A, Chiu S, Tolomiczenko G, Kiss A, Cowan L, et al. The effect of traumatic brain injury on the health of homeless people. CMAJ Can Med Assoc J. (2008) 17:779–84. doi: 10.1503/cmaj.080341
23. Whiteneck GG, Cuthbert JP, Corrigan JD, Bogner JA. Risk of negative outcomes after traumatic brain injury: a statewide population-based survey. J Head Trauma Rehabil. (2016) 31:E43–54. doi: 10.1097/HTR.0000000000000141
24. Campbell JK, Joseph A-LC, Rothman EF, Valera EM. The prevalence of brain injury among survivors and perpetrators of intimate partner violence and the prevalence of violence victimization and perpetration among people with brain injury: a scoping review. Curr Epidemiol Rep. (2022) 302:1–26. doi: 10.1007/s40471-022-00302-y
25. Beydoun HA, Williams M, Beydoun MA, Eid SM, Zonderman AB. Relationship of physical intimate partner violence with mental health diagnoses in the nationwide emergency department sample. J Womens Health. (2017) 26:141–51. doi: 10.1089/jwh.2016.5840
26. Kwako LE, Glass N, Campbell J, Melvin KC, Barr T, Gill JM. Traumatic brain injury in intimate partner violence: a critical review of outcomes and mechanisms. Trauma Viol Abuse. (2011) 12:115–26. doi: 10.1177/1524838011404251
27. Iverson KM, Dardis CM, Pogoda TK. Traumatic brain injury and ptsd symptoms as a consequence of intimate partner violence. Compreh Psychiatry. (2017) 74:80–7. doi: 10.1016/j.comppsych.2017.01.007
28. St Ivany A, Bullock L, Schminkey D, Wells K, Sharps P, Kools S. Living in fear and prioritizing safety: exploring women's lives after traumatic brain injury from intimate partner violence. Qual Health Res. (2018) 28:1708–18. doi: 10.1177/1049732318786705
29. Schwarzbold M, Diaz A, Martins ET, Rufino A, Amante LN, Thais ME, et al. Psychiatric disorders and traumatic brain injury. Neuropsychiatr Dis Treat. (2008) 4:797–816. doi: 10.2147/NDT.S2653
30. Rosen V, Ayers G. An update on the complexity and importance of accurately diagnosing post-traumatic stress disorder and comorbid traumatic brain injury. Neurosci Insights. (2020) 15:2633105520907895. doi: 10.1177/2633105520907895
31. Davis A. Violence-related mild traumatic brain injury in women: identifying a triad of postinjury disorders. J Trauma Nurs Off J Soc Trauma Nurs. (2014) 21:300–8. doi: 10.1097/JTN.0000000000000086
32. Oram S, Fisher HL, Minnis H, Seedat S, Walby S, Hegarty K, et al. The lancet psychiatry commission on intimate partner violence and mental health: advancing mental health services, research, and policy. Lancet Psychiatry. (2022) 9:487–524. doi: 10.1016/S2215-0366(22)00008-6
33. Kumar RG, Gao S, Juengst SB, Wagner AK, Fabio A. The effects of post-traumatic depression on cognition, pain, fatigue, and headache after moderate-to-severe traumatic brain injury: a thematic review. Brain Injury. (2018) 32:383–94. doi: 10.1080/02699052.2018.1427888
34. Arksey H, O'Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. (2005) 8:19–32. doi: 10.1080/1364557032000119616
35. Peters MD, Godfrey CM, Khalil H, McInerney P, Parker D, Soares CB. Guidance for conducting systematic scoping reviews. Int J Evid Based Healthcare. (2015) 13:141–6. doi: 10.1097/XEB.0000000000000050
36. Peters M, Godfrey C, McInerney P, Munn Z, Tricco A, Khalil H. Chapter 11: scoping reviews (2020 version). In:Aromataris E, Munn Z, , editors. JBI Manual for Evidence Synthesis. Adelaide: Joanna Briggs Institute (2020). doi: 10.46658/JBIRM-20-01
37. Tricco AC, Lillie E, Zarin W, O'Brien KK, Colquhoun H, Levac D, et al. Prisma extension for scoping reviews (prisma-Scr): checklist and explanation. Ann Internal Med. (2018) 169:467–73. doi: 10.7326/M18-0850
38. Chan V, Toccalino D, Colantonio A. Systematic review protocol for facilitators and barriers to integrating health services for traumatic brain injury and mental health or addictions. BMJ Open. (2019) 9:e027534. doi: 10.1136/bmjopen-2018-027534
39. Chan V, Toccalino D, Omar S, Shah R, Colantonio A. A systematic review on integrated care for traumatic brain injury, mental health, and substance use. PLoS ONE. (2022) 17:e0264116. doi: 10.1371/journal.pone.0264116
40. Roberts AR, Kim JH. Exploring the effects of head injuries among battered women: a qualitative study of chronic and severe woman battering. J Soc Serv Res. (2005) 32:33–47. doi: 10.1300/J079v32n01_03
41. Valera E, Kucyi A. Brain injury in women experiencing intimate partner-violence: neural mechanistic evidence of an “invisible” Trauma. Brain Imag Behav. (2017) 11:1664–77. doi: 10.1007/s11682-016-9643-1
42. Hunnicutt G, Lundgren K, Murray C, Olson L. The intersection of intimate partner violence and traumatic brain injury: a call for interdisciplinary research. J Family Viol. (2017) 32:471–80. doi: 10.1007/s10896-016-9854-7
43. Valera EM, Berenbaum H. Brain injury in battered women. J Consult Clin Psychol. (2003) 71:797–804. doi: 10.1037/0022-006X.71.4.797
44. Veritas Health Innovation. Covidence Systematic Review Software. Melbourne: Veritas Health Innovation (2022). Available online at: www.covidence.org (accessed April, 2020).
45. Popay J, Roberts H, Sowden A, Petticrew M, Arai L, Rodgers M, et al. Guidance on the conduct of narrative synthesis in systematic reviews. Prod ESRC Methods Prog. (2006) 1:b92. Available online at: https://www.lancaster.ac.uk/media/lancaster-university/content-assets/documents/fhm/dhr/chir/NSsynthesisguidanceVersion1-April2006.pdf
46. Page MJ, McKenzle JE, Bossuyt PM, Boutron I, Hoffman TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) 372:n71. doi: 10.1136/bmj.n71
47. Brown J, Clark D, Pooley AE. Exploring the use of neurofeedback therapy in mitigating symptoms of traumatic brain injury in survivors of intimate partner violence. J Aggr Maltreat Trauma. (2019) 28:764–83. doi: 10.1080/10926771.2019.1603176
48. Ralston B, Rable J, Larson T, Handmaker H, Lifshitz J. Forensic nursing examination to screen for traumatic brain injury following intimate partner violence. J Aggr Maltreat Trauma. (2019) 28:732–43. doi: 10.1080/10926771.2019.1637988
49. Saleem GT, Champagne M, Haider MN, Leddy JJ, Willer B, Asante I, et al. Prevalence and risk factors for intimate partner physical violence-related acquired brain injury among visitors to justice center in New York. J Head Trauma Rehabil. (2022) 37:E10–E9. doi: 10.1097/HTR.0000000000000750
50. Gabbe BJ, Braaf S, Cameron PA, Berecki-Gisolf J. Epidemiology and 6- and 12-month outcomes of intimate partner violence and other violence-related traumatic brain injury in major Trauma: a population-based trauma registry study. J Head Trauma Rehabil. (2022) 37:E1–9. doi: 10.1097/HTR.0000000000000741
51. Joshi M, Thomas K, Sorenson S. “I didn't know i could turn colors”: health problems and health care experiences of women strangled by an intimate partner. Soc Work Health Care. (2012) 51:798–814. doi: 10.1080/00981389.2012.692352
52. Monahan K, O'Leary KD. Head injury and battered women: an initial inquiry. Health Soc Work. (1999) 24:269–78. doi: 10.1093/hsw/24.4.269
53. Saadi A, Anand P, Kimball SL. Traumatic brain injury and forensic evaluations: three case studies of US asylum-seekers. J For Legal Med. (2021) 79:2139. doi: 10.1016/j.jflm.2021.102139
54. Wilbur L, Higley M, Hatfield J, Surprenant Z, Taliaferro E, Smith DJ, et al. Survey results of women who have been strangled while in an abusive relationship. J Emerg Med. (2001) 21:297–302. doi: 10.1016/S0736-4679(01)00398-5
55. Mittal M, Resch K, Nichols-Hadeed C, Thompson Stone J, Thevenet-Morrison K, Faurot C, et al. Examining associations between strangulation and depressive symptoms in women with intimate partner violence histories. Viol Vict. (2018) 33:1072–87. doi: 10.1891/0886-6708.33.6.1072
56. Cimino AN Yi G, Patch M, Alter Y, Campbell JC, Gundersen KK, et al. The effect of intimate partner violence and probable traumatic brain injury on mental health outcomes for black women. J Aggr Maltreat Trauma. (2019) 28:714–31. doi: 10.1080/10926771.2019.1587657
57. Oden TM. Insult denied: traumatic brain injury in battered African American women. Disser Abst Int Sect B Sci Eng. (2000) 61:1864.
58. Wong JYH, Choi AWM, Wong JKS, Ng ZLH, Cheung KY, Lau CL, et al. Impact of mild traumatic brain injury on physical, mental and cognitive functioning of abused women admitted to emergency units. Health Soc Care Commun. (2020) 06:13218. doi: 10.1111/hsc.13218
59. Iverson KM, Dardis CM, Grillo AR, Galovski TE, Pogoda TK. Associations between traumatic brain injury from intimate partner violence and future psychosocial health risks in women. Compreh Psychiatry. (2019) 92:13–21. doi: 10.1016/j.comppsych.2019.05.001
60. Iverson KM, Pogoda TK. Traumatic brain injury among women veterans: an invisible wound of intimate partner violence. Med Care. (2015) 53:S112–9. doi: 10.1097/MLR.0000000000000263
61. Maldonado-Rodriguez N, Crocker CV, Taylor E, Jones KE, Rothlander K, Smirl J, et al. Characterization of cognitive-motor function in women who have experienced intimate partner violence-related brain injury. J Neurotrauma. (2021) 38:2723–30. doi: 10.1089/neu.2021.0042
62. Fortier CB, Beck BM, Werner KB, Iverson KM, Kim S, Currao A, et al. The boston assessment of traumatic brain injury-lifetime semistructured interview for assessment of tbi and subconcussive injury among female survivors of intimate partner violence: evidence of research utility and validity. J Head Trauma Rehabil. (2021) 37:E175–85. doi: 10.1097/HTR.0000000000000700
63. Galovski TE, Werner KB, Weaver TL, Morris KL, Dondanville KA, Nanney J, et al. Massed cognitive processing therapy for posttraumatic stress disorder in women survivors of intimate partner violence. Psychol Trauma Theory Res Pract Policy. (2021) 14:769–79. doi: 10.1037/tra0001100
64. Marcantonis E. The prevalence of traumatic brain injury in battered women residing in Northern New Jersey Shelters. Dissert Abst Int Sect B Sci Eng. (2004) 64:3532.
65. McFadgion A. Intimate partner violence and probable traumatic brain injury: manifestations in the lives of abused women. Dissert Abst Int Sect A Hum Soc Sci. (2014) 75:3613786.
66. Valera EM, Daugherty JC, Scott OC, Berenbaum H. Strangulation as an acquired brain injury in intimate-partner violence and its relationship to cognitive and psychological functioning: a preliminary study. J Head Trauma Rehabil. (2022) 37:15–23. doi: 10.1097/HTR.0000000000000755
67. Likitlersuang J, Brown EM, Salat DH, Iverson KM, Werner K, McGlinchey RE, et al. Neural correlates of traumatic brain injury in women survivors of intimate partner violence: a structural and functional connectivity neuroimaging study. J Head Trauma Rehabil. (2022) 37:E30–E8. doi: 10.1097/HTR.0000000000000758
68. Smirl JD, Jones KE, Copeland P, Khatra O, Taylor EH, Van Donkelaar P. Characterizing symptoms of traumatic brain injury in survivors of intimate partner violence. Brain Injury. (2019) 33:1529–38. doi: 10.1080/02699052.2019.1658129
69. Smith DJ, Mills T, Taliaferro EH. Frequency and relationship of reported symptomology in victims of intimate partner violence: the effect of multiple strangulation attacks. J Emerg Med. (2001) 21:323–9. doi: 10.1016/S0736-4679(01)00402-4
70. Rajaram SS, Reisher P, Garlinghouse M, Chiou KS, Higgins KD, New-Aaron M, et al. Intimate partner violence and brain injury screening. Viol Against Women. (2021) 27:1548–65. doi: 10.1177/1077801220947164
71. Waite JD. Memory in adult female victims of intimate partner violence. Dissert Abst Int Sect B Sci Eng. (2019) 80:10932401.
72. Goldin Y, Haag HL, Trott CT. Screening for history of traumatic brain injury among women exposed to intimate partner violence. PM&R. (2016) 8:1104–10. doi: 10.1016/j.pmrj.2016.05.006
73. Colantonio A, Harris JE, Ratcliff G, Chase S, Ellis K. Gender differences in self reported long term outcomes following moderate to severe traumatic brain injury. BMC Neurol. (2010) 10:102. doi: 10.1186/1471-2377-10-102
74. Munivenkatappa A, Agrawal A, Shukla D, Kumaraswamy D, Devi B. Traumatic brain injury: does gender influence outcomes? Int J Crit Illness Injury Sci. (2016) 6:70–3. doi: 10.4103/2229-5151.183024
75. Mollayeva T, Mollayeva S, Colantonio A. Traumatic brain injury: sex, gender and intersecting vulnerabilities. Nat Rev Neurol. (2018) 14:711–22. doi: 10.1038/s41582-018-0091-y
76. Iovine-Wong PE, Nichols-Hadeed C, Stone JT, Gamble S, Cross W, Cerulli C, et al. Intimate partner violence, suicide, and their overlapping risk in women veterans: a review of the literature. Milit Med. (2019) 184:E201–E10. doi: 10.1093/milmed/usy355
77. Murray CE, Lundgren K, Olson LN, Hunnicutt G. Practice update: what professionals who are not brain injury specialists need to know about intimate partner violence-related traumatic brain injury. Trauma, Viol Abuse. (2016) 17:298–305. doi: 10.1177/1524838015584364
78. Tanev KS, Pentel KZ, Kredlow MA, Charney ME. Ptsd and tbi co-morbidity: scope, clinical presentation and treatment options. Brain Injury. (2014) 28:261–70. doi: 10.3109/02699052.2013.873821
79. Employment and Social Development Canada. Canada Announces Support to Those Experiencing Homelessness and Women Fleeing Gender-Based Violence During the Coronavirus Disease (COVID-19) Pandemic. Gatineau: Employment and Social Development Canada (2020).
80. Toccalino D, Haag H, Estrella M, Cowle S, Fuselli P, Ellis M, et al. The intersection of intimate partner violence and traumatic brain injury: findings from an emergency summit addressing system-level changes to better support women survivors. J Head Trauma Rehabil. (2022) 37:E20–E9. doi: 10.1097/HTR.0000000000000743
81. Sinha M. Measuring Violence against Women: Statistical Trends. St Louis: Canadian Centre for Justice Statistics (2013).
82. Haag HL, Biscardi M. Pauktuutit Inuit Women of Canada, Smith NN, MacGregor N, Colantonio A. Traumatic brain injury and intimate partner violence: addressing knowledge and service gaps among indigenous populations in Canada. Brain Impair. (2019) 20:197–210. doi: 10.1017/BrImp.2019.16
83. Mahood Q, Van Eerd D, Irvin E. Searching for grey literature for systematic reviews: challenges and benefits. Res Synth Methods. (2014) 5:221–34. doi: 10.1002/jrsm.1106
84. Chiou KS, Feiger JA, Cissne M, Garlinghouse M, Reisher P, Higgins K, et al. Survey of depressive symptomatology in brain injury resulting from intimate partner violence. Brain Inj. (2023) 37:159–69. doi: 10.1080/02699052.2022.2158220
85. Oakley LD, Luebke J, Dosch NC, Snedden TR, Hernadez H, Lemke M, et al. Traumatic brain injury screening and the unmet health needs of shelter-seeking women with head injuries related to intimate partner violence. Women's Health Rep. (2021) 2:586–93. doi: 10.1089/whr.2021.0056
Keywords: intimate partner violence (IPV), brain injury—traumatic, brain injury, strangulation, mental health, health services research
Citation: Toccalino D, Moore A, Cripps E, Gutierrez SC, Colantonio A, Wickens CM, Chan V, Nalder E and Haag HL (2023) Exploring the intersection of brain injury and mental health in survivors of intimate partner violence: A scoping review. Front. Public Health 11:1100549. doi: 10.3389/fpubh.2023.1100549
Received: 16 November 2022; Accepted: 26 January 2023;
Published: 02 March 2023.
Edited by:
Sara Morgan, University of Southampton, United KingdomReviewed by:
Oludoyinmola Omobolade Ojifinni, University of the Witwatersrand, South AfricaKathleen Whiting, Uniformed Services University of the Health Sciences, United States
Copyright © 2023 Toccalino, Moore, Cripps, Gutierrez, Colantonio, Wickens, Chan, Nalder and Haag. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Danielle Toccalino, danielle.toccalino@mail.utoronto.ca