 Antoine Citerne
Antoine Citerne Fanny Rancière1,2†
Fanny Rancière1,2† Célina Roda
Célina Roda- 1Health Environmental Risk Assessment (HERA) Team, Centre of Research in Epidemiology and Statistics (CRESS), Inserm, National Research Institute for Agriculture, Food and the Environment (INRAE), Université de Paris, Paris, France
- 2Faculté de Pharmacie de Paris, Université de Paris, Paris, France
- 3Cellule Cohorte, Direction de l'Action Sociale de l'Enfance et de la Santé, Mairie de Paris, Paris, France
Background: Few studies have examined the overall experience of adolescents and their families during COVID-19 lockdowns. This study describes COVID-19-related morbidity in the PARIS birth cohort families during the first lockdown in France and identifies family profiles in terms of morbidity, perception, behaviors, and attitudes.
Methods: Online questionnaires were sent to adolescents of the PARIS birth cohort and their parents. Possible COVID-19 was defined by symptoms using the ECDC definition. Household transmission was estimated by calculating the observed clinical secondary attack rates. Perception, behaviors and attitudes were assessed by levels of stress, degree of satisfaction regarding levels of information about COVID-19, degree of agreement with the lockdown and preventive measures. COVID-19 morbidity in adolescents and parents was compared using chi-squared or Student's t-tests. Within each family, perception, behaviors, and attitudes were compared between adolescents and parents using matched-pairs tests. To identify contrasting family profiles, a K-means cluster analysis was implemented.
Results: Of 1,549 families contacted, 1,051 (68%) participated. Adolescents were less affected by possible COVID-19 than their parents (138.7 vs. 192.7 per 1,00,000 person-days). Household transmission of possible COVID-19 was higher when possible COVID-19 came from adults than from adolescents. Most families implemented preventive measures. Adolescents and parents generally shared the same attitudes, but adolescents were less compliant with restrictive measures. Four family profiles were identified which differed mainly regarding family stress, COVID-19 in the household, and compliance with preventive measures.
Conclusion: Improving information dissemination to parents and adolescents, including dedicated adolescent messages, would increase adherence to preventive measures.
Introduction
After a cluster of pneumonia cases was reported in Wuhan, China, in December 2019, coronavirus disease 2019 (COVID-19), caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), was characterized by the World Health Organization as a pandemic on 03/11/2020 (1). At this time, due to the high demand and shortage of reagents, many national health authorities had to reserve tests for people with severe symptoms of COVID-19 or specific situations. Consequently, very few studies have been able to assess the prevalence or incidence of COVID-19 in general population. One solution was to rely on symptoms of COVID-19 (2, 3), or use SARS-CoV-2 serological tests (4). In France, there were studies in specific populations: in socially deprived neighborhoods (5, 6), suburban households (7) or in day-care centers (8); but few focused on adolescents and their families. Furthermore, the susceptibility of adolescents to SARS-CoV-2 infection seems to be similar to adults to date (9–11) but the role of adolescents in the household transmission of the SARS-CoV-2 during lockdown remains unclear. Some studies showed no difference in SARS-CoV-2 transmission between children and adults in households (12, 13), while others showed a lower household transmission rate from children compared to adults (14, 15).
To slow the spread of COVID-19, several countries successively opted for lockdown measures. In France, a lockdown procedure was implemented between 03/17/2020 and 05/10/2020. This national lockdown included: closing public spaces, businesses, services, and schools; restricting travel (except for necessary food shopping, medical care, legal obligations, and work when telecommuting was not possible) and limiting outside time to the vicinity of homes (individual sports activity, dog hygiene). This unprecedented situation led to a sudden disruption in the daily lives of adolescents and their families. In order to assess the impact of these public health measures, it is important to better understand the perception and compliance with these measures. Studying the behaviors and attitudes of adolescents and their families is essential to a more accurate comprehension of the dynamics of transmission during the lockdown and the impact of these measures on adolescents. To our knowledge, no studies considered the overall experience of adolescents and their families in terms of morbidity, perception, behaviors, and attitudes during this exceptional event.
Our aims were, i) to describe the morbidity related to COVID-19 in the families of the PARIS birth cohort; ii) to identify family profiles in terms of morbidity, perception, behaviors, and attitudes, during the COVID-19 pandemic in France from 03/17/2020 to 05/10/2020.
Methods
Study Design and Participants
This cross-sectional study was carried-out in the PARIS population-based birth cohort which is composed of healthy newborns living in the Paris area recruited between 2003 and 2006 in five Paris hospitals (16). At the end of the first lockdown in France, 1,549 families with an available email address were invited to participate in a specific survey based on both adolescent and parent online self-administered questionnaires. The present study deals with 1,051 families who answered at least one questionnaire (adolescent and/or parents). The response rate was 68%. The French Ethics Committees approved the PARIS cohort follow-up (permission nos. 031153, 051289; ID-RCB, 2009-A00824-53). Parents and adolescents gave their informed consent.
Data Collection
Data from online questionnaires included questions on socio-demographic, family, and home characteristics, reported COVID-19 morbidity, perception, behaviors, and attitudes during the first lockdown (03/17/2020 to 05/10/2020).
Reported COVID-19 Morbidity and Household Transmission
COVID-19 morbidity was assessed for the adolescent, the responding parent, and all relatives in the same household during the lockdown. Families reported symptoms suggestive of COVID-19 since the beginning of the year, date of onset and end of symptoms, potential close contact with a COVID-19-like symptoms case and/or a test-confirmed COVID-19 case in the 14 days prior to symptom onset, doctor-diagnosed COVID-19, test-confirmed COVID-19, medical care, and medications. Possible COVID-19 cases were defined according to the European Centre for Disease Prevention and Control as any person with at least one of the following symptoms: cough, fever, shortness of breath, anosmia, ageusia or dysgeusia (17). Possible COVID-19 cases or test-confirmed COVID-19 cases that occurred during the lockdown period between 03/17/2020 and 05/10/2020 inclusive, were identified within each household. Secondary cases were defined as possible COVID-19 cases that occurred between 2 to 14 days after a primary case from the same household. A household contact of a primary case was defined as a family member or a close relative living in the same household during the full lockdown period who did not develop possible COVID-19 or had test-confirmed COVID-19 before the primary case.
Perception, Behaviors, and Attitudes
Adolescents and parents assessed their levels of stress (overall and SARS-CoV-2-related) from the beginning of the lockdown on a 0-to-10 scale and their degree of satisfaction regarding the level of information received about SARS-CoV-2. Adolescents reported their degree of agreement with lockdown measures while their parents indicated adolescents' tolerance of the lockdown (0-to-10 scale). Concerning changes in family behaviors during the lockdown, we collected adolescents' and parents' information on potential implementation and reinforcement of COVID-19 preventive measures, as well as the frequencies per week of leaving the house for fresh air or shopping and the number of people they had met the previous day. Finally, the parent questionnaire explored the main reason why respondents changed their behavior during the lockdown. Questionnaires were pilot tested.
Statistical Analysis
The main characteristics of responding and non-responding families were compared using chi-squared tests. Family and home characteristics during the lockdown were described. Incidence rates of possible COVID-19 were calculated for adolescents and parents during the lockdown (from 03/17/2020 to 05/10/2020 inclusive). For each participant never having contracted a possible COVID-19 before the start of the lockdown, the time-at-risk was calculated. This was the time from the first day of the lockdown to: i) the day when the first symptoms were reported in possible COVID-19 cases; ii) the last day of the lockdown or the day the questionnaire was filled in (if before the end of the lockdown) when no possible COVID-19 was detected. The 95% confidence intervals (CI) were determined using the quadratic approximation to the Poisson log likelihood for the log-rate parameter. The observed clinical secondary attack rates (SAR) were estimated as the proportion of secondary cases among all household contacts and according to the age of the primary case. Among possible COVID-19 cases, adolescents and parents were compared regarding symptoms, clinical characteristics and medical care using chi-squared, Fisher's exact tests and Student's t-tests. Within each family, perception, behaviors, and attitudes were compared between adolescents and parents using McNemar and Wilcoxon matched-pairs signed-rank tests. To identify contrasting family profiles during the lockdown, a K-means partitioning cluster analysis was implemented on 70 variables related to socio-demographics, family and home characteristics, COVID-19 morbidity, perception, behaviors, and attitudes. Quantitative variables were standardized using Z-scores. The algorithm was performed over 10,000 iterations and repeatedly fitted with 2 to 10 clusters. The optimal classification was chosen based on Calinski-Harabasz criterion and relevance. To compare family profiles and detect the most discriminating variables, chi-squared, Fisher's exact, and Kruskal-Wallis tests were realized with post-hoc Tukey's HSD (honestly significant difference) test. All analyses were performed on Stata/SE, using the complete-case method.
Results
Participants
Of the 1,549 families to whom questionnaires were sent, 866 adolescents (13–17 years old) and 966 parents responded (Supplementary Figure 1). No differences were observed between participating and non-participating families for sex of the adolescent, place of residence at birth, parental socioeconomic status (SES) and presence of older siblings (Supplementary Table 1).
Family and Home Characteristics
Table 1 presents the family and home characteristics during the lockdown. Six percent of the adolescents spent most of the lockdown out of their main residence. The median number of persons in the household was four with a median area of 25 m2/person. At least one parent had an occupation deemed “essential” (e.g., health care, food manufacture and supply) in 29.9% of the families: 40 percent of this group were health professionals.
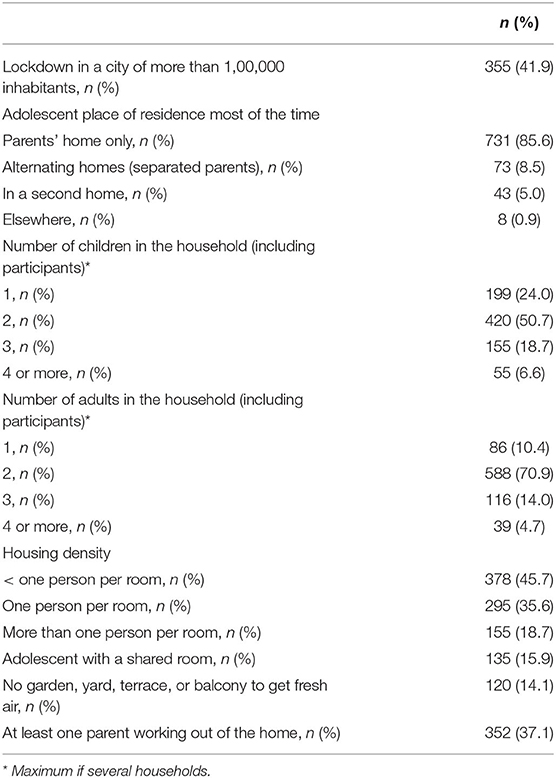
Table 1. Family and home characteristics of the PARIS birth cohort during the lockdown.
Reported COVID-19 Morbidity
From 01/01/2020 to 05/10/2020, there were 159 possible COVID-19 cases in adolescents with no difference detected according to sex, age, body mass index and family SES. During lockdown, possible COVID-19 was developed by 53 adolescents and 78 parents for 38,206 and 40,487 person-days-at-risk (Table 2).
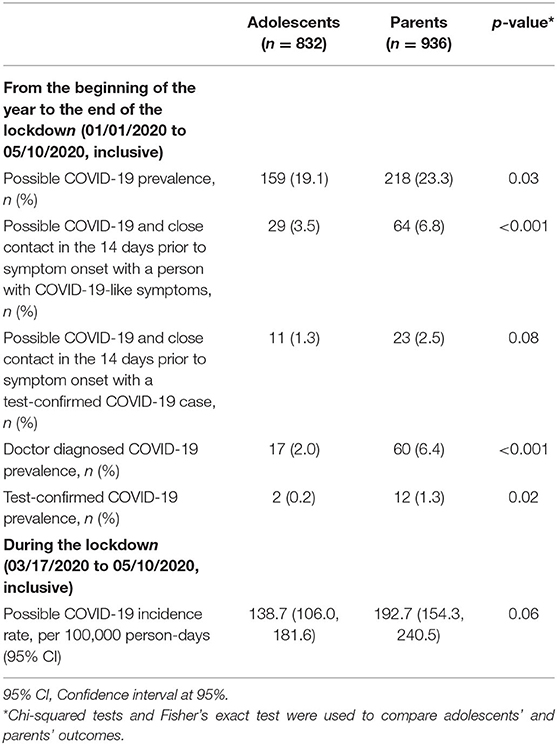
Table 2. Comparison of prevalence and incidence rates of COVID-19 outcomes between adolescents and parents in the PARIS birth cohort.
Concerning possible COVID-19 cases, fewer adolescents suffered from fatigue and more presented rhinitis-like and gastrointestinal symptoms, compared with parents (Table 3). The median recovery time in adolescents and parents with possible COVID-19 was 9 days (first-third quartile: 5–30 days) and 16 days (7–31 days).
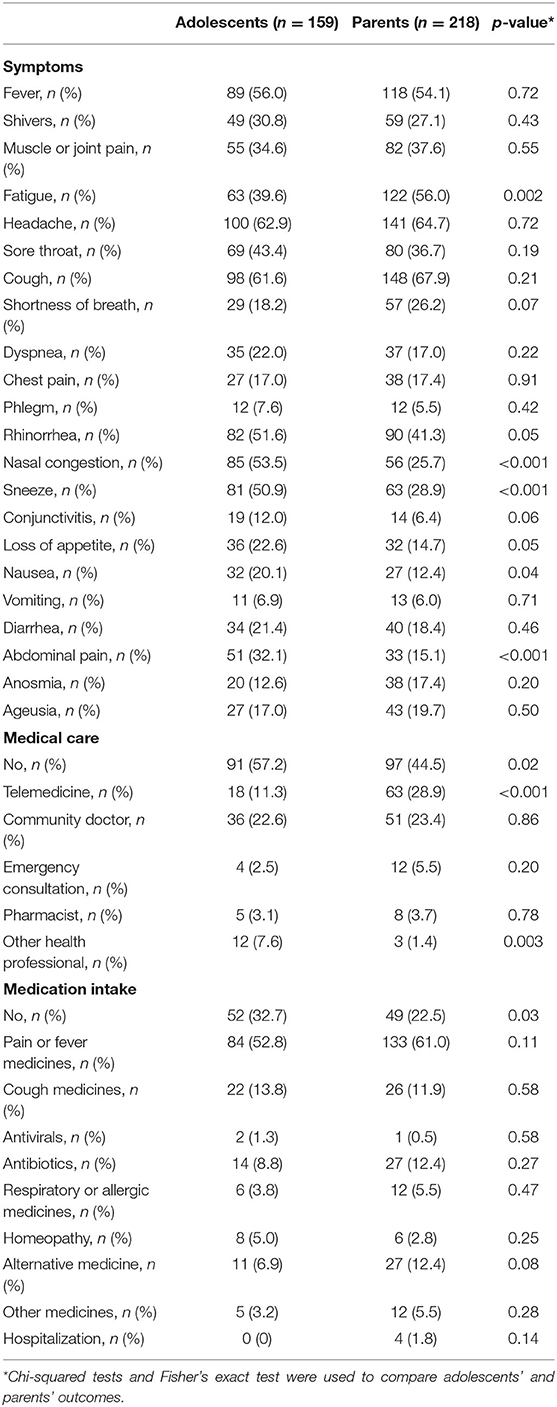
Table 3. Comparison of clinical characteristics and medical care between adolescents and parents with possible COVID-19 in the PARIS birth cohort.
Household Transmission
During the lockdown, 422 possible COVID-19 cases were identified in 291 households. The observed clinical SAR of possible COVID-19 was 6.8% (95% CI: 5.2, 8.6) among 900 household contacts. This was 4.3% (95% CI: 0.5, 14.8) from children, 4.4% (95% CI: 2.2, 7.7) from adolescents and 7.8% (95% CI: 5.8, 10.4) from adults (Supplementary Table 2).
Perception, Behaviors, and Attitudes
Adolescents reported general and SARS-CoV-2-related stress levels lower than their parents (p < 0.001). Both adolescents and parents used the media as the primary information source regarding SARS-CoV-2 (47.3 vs. 61.1%, p < 0.001). Adolescents were more likely to select social networks (11.4 vs. 2.0%, p < 0.001) or their relatives and friends (22.5 vs. 0.8%, p < 0.001) as primary source of information. Adolescents were fewer to be satisfied with their level of information about the SARS-CoV-2 than their parents (60.0 vs. 66.5%, p = 0.006). They tended to be less often satisfied with their level of information when using social networks as their primary source of information (53.1% satisfied using social networks, 61.4% using other sources of information, p = 0.12). Concerning behaviors over the whole lockdown, 96.0% of the adolescents implemented or reinforced at least one preventive measure. The preventive measures most frequently cited by adolescents were cleaning hands (79.8%), avoiding kissing and/or hugging (76.6%), avoiding shaking hands (74.8%) and avoiding going outside (73.7%). Compared with their parents, adolescents generally applied significantly fewer preventive measures (Figure 1).
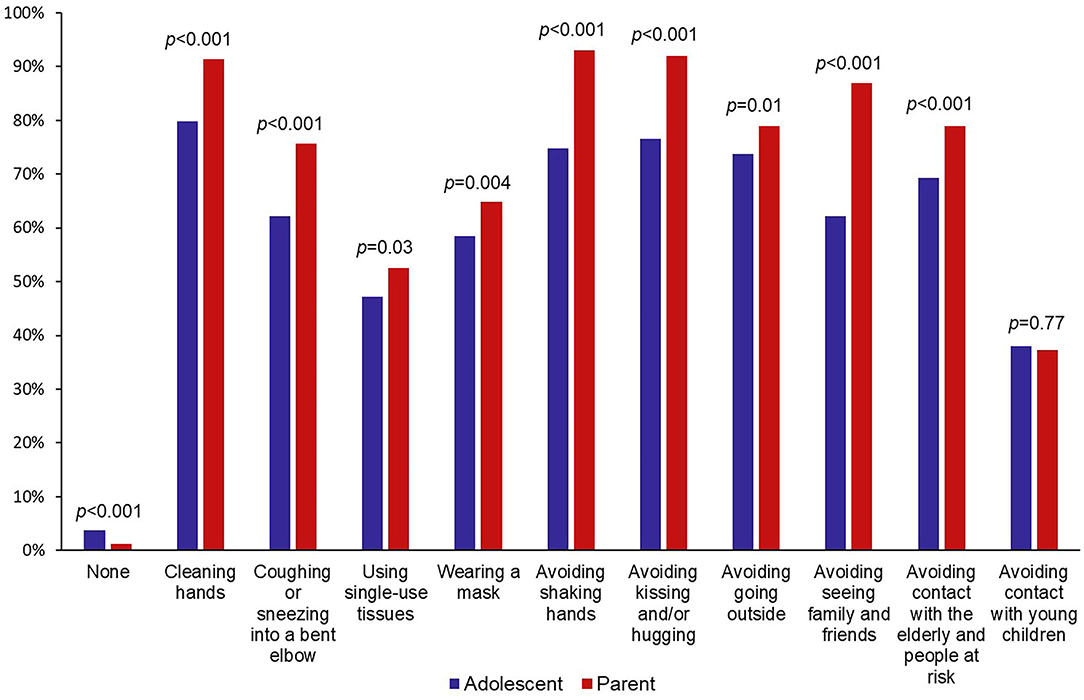
Figure 1. Implementation and reinforcement of COVID-19 preventive measures for adolescents and their parents in the PARIS birth cohort during lockdown.
Family Profiles
A total of 589 families were included in the cluster analysis. Four family profiles were identified. Variables that most distinguished each cluster from another were adolescents' and parents' SARS-CoV-2-related stress levels and overall stress levels, adolescents' tolerance of the lockdown according to the parent, frequency at which the parent left the house for shopping and the number of people the parent had met the previous day (Table 4 and Supplementary Tables 3–7).
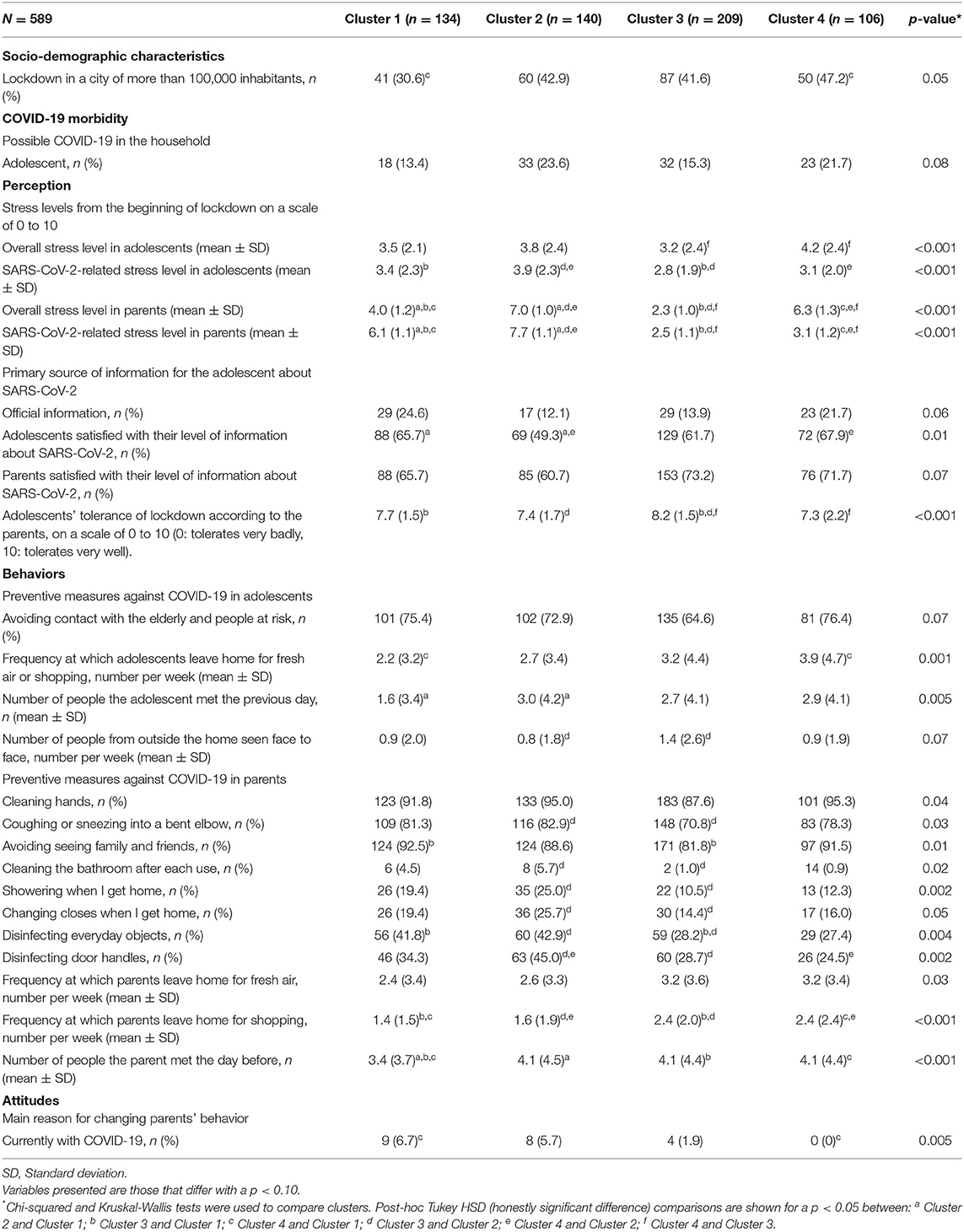
Table 4. Profiles of families from the PARIS birth cohort based on socio-demographic characteristics, COVID-19 morbidity, perception, behaviors, and attitudes during the lockdown.
Cluster 1 (23% of participants) adolescents and parents experienced SARS-CoV-2-related stress, with parents reporting leaving the house for shopping less often than other clusters and meeting fewer people the previous day. Cluster 1 families were less likely to live in a city of more than 1,00,000 inhabitants and were less affected by possible COVID-19 (13.4% of the adolescents).
Cluster 2 (24% of participants) adolescents and parents reported the most SARS-CoV-2-related stress. Parents in Cluster 2 left the house for shopping less often and often applied more extensive preventive measures: cleaning the bathroom after each use, showering, and changing clothes when they arrived home, disinfecting everyday objects and disinfecting door handles. This was the cluster most affected by possible COVID-19 (23.6% of the adolescents).
The largest group was Cluster 3 (35% of participants). Compared to the families from the other clusters, both parents and adolescents showed the least stress and were the least compliant regarding preventive measures. Parents left the house for shopping more frequently. Adolescents saw more people face-to-face and their tolerance of lockdown was the best of all the clusters. The prevalence of possible COVID-19 in Cluster 3 adolescents was 15.3%.
Cluster 4 (18% of participants) adolescents and parents had an overall stress level higher than SARS-CoV-2-related stress level. Families lived more frequently in a city of more than 100,000 inhabitants. Parents were more likely to work outside the home during the lockdown (47.2%) and to leave the house for shopping. Adolescents were less likely to stay at their parents' home for the duration of the lockdown. The prevalence of possible COVID-19 in adolescents in Cluster 4 was 21.7%.
Discussion
Key Results
PARIS adolescents were less affected by possible COVID-19 at the end of the first lockdown than their parents. Household transmission during the lockdown was higher when possible COVID-19 came from adults than when it came from adolescents. Most adolescents and parents implemented prevention measures. Nevertheless, adolescents respected these measures less than their parents. Four family profiles were identified. The main factors differentiating these profiles were stress, particularly parental stress, and compliance with preventive measures. This study showed that compliance with preventive measures was strongly related to family stress and COVID-19 morbidity.
Reported COVID-19 Morbidity
In this study, adolescents were less affected by COVID-19 than their parents. Only the EpiCov study looked at the seroprevalence of SARS-CoV-2 in adolescents in France during the lockdown with a seroprevalence lower in adolescents (3.6%) than in the general population (4.5%) (18). Nevertheless, the prevalence of possible COVID-19 probably led to overestimation of the real prevalence of COVID-19. Our study showed that only 0.2% of the adolescents had test-confirmed COVID-19. This low proportion could be largely explained by the limited access to virological testing during this period. Regarding the clinical manifestations of possible COVID-19 in PARIS teenagers, symptoms were similar to those presented in children studies (19, 20). Adolescents were more likely to develop mild symptoms such as rhinitis-like symptoms and headache. In contrast, parents appeared to develop more severe COVID-19 than adolescents: fatigue symptoms were more frequent, and the duration of symptoms was longer. These results are consistent with previous published findings showing a correlation between age and severity (21, 22). Adolescents suffered from gastrointestinal symptoms more frequently than parents, which has been shown in children (23–25). The household observed clinical SAR of possible COVID-19 (6.8%) was lower than the test-confirmed COVID-19 pooled SAR observed in Thompson et al. (21.1%) and Madewell et al. (16.6%) meta-analysis (26, 27). However, they included few European studies and showed a great heterogeneity of household SAR (0 to 51%) due to different durations of exposure and different testing strategies. The lower SAR observed in our study could be a result of the possible overestimation of primary cases and thus an underestimation of household transmission. However, transmission was lower from adolescents than from adults, which has been previously observed in children but not specifically in adolescents (14, 26, 27). The reasons why adolescents were less affected by COVID-19 than adults could be explained by a greater exposure to SARS-CoV-2 in adults than in adolescents due to the need to go out for shopping or work. Moreover, because the viral load is lower and clearance is faster in the milder COVID-19, this would help explain why transmission from adolescents was lower than from adults (28).
Perception, Behaviors, and Attitudes
PARIS adolescents had a lower stress level than their parents. This may be due to lower exposure of adolescents to pandemic-related stress. During the lockdown, adolescents were educated at home while parents had additional role demands that could cause psychological stress (29). Despite this, adolescents were less satisfied with their level of received information about the SARS-CoV-2 than their parents. Adolescents' use of social networks compared with their parents could explain this lower level of satisfaction. Indeed, adolescents using social networks as their primary source of information were less often satisfied with it. It has been shown that adolescents are often suspicious of health information from the Internet, but still use it (30). This study found that adolescents were less compliant with preventive measures than their parents. Adolescents could have felt less concerned about the pandemic than their parents. However, PARIS families generally complied with preventive measures. These results agree with the EPIDEMIC project based on adults of the French population (31). Overall, adolescents tolerated the lockdown well, which could be due to their living conditions related to high SES.
Family Profiles
Clusters revealed the importance of stress and compliance with lockdown measures in differentiating families. Adolescents generally reported attitudes towards lockdown measures similar to their parents, even if they were less compliant. This could be explained by parental practices and parental coping (32). Furthermore, a probable association between stress, COVID-19, and preventive measures has been pointed out. Cluster 2 reported the higher stress level, was the most affected by COVID-19 and strongly respected preventive measures. Conversely, Cluster 3 reported the lower stress level, was the least affected by COVID-19, and was the least compliant with preventive measures. It has been shown that having had COVID-19 may increase compliance with preventive measures (33). Regarding stress levels, fears of infecting others or oneself may increase compliance with preventive measures (34). In Cluster 1, families were relatively stressed but less affected by COVID-19. They lived less frequently in a large city. Cluster 4 families were stressed but not specifically by SARS-CoV-2. They more often lived in a large city and had one parent working outside the home. The economic or job-related situation of these families may have been an important source of stress.
Strengths and Limitations
It is one of the first studies to consider the complementary views of both adolescents and parents. The use of two simultaneous self-administered questionnaires made it possible to compare morbidity, perception, behaviors and attitudes of adolescents and parents and to collect a large variety of information. The comparison of COVID-19 morbidity between children and adults has been studied, but rarely in adolescents. This study is innovative in comparing perception, behaviors and attitudes between adolescents and their parents. The use of online questionnaires at the end of the lockdown made it possible to cover the entire duration of the lockdown. Finally, the participation rate was satisfactory and remains comparable to other studies (2, 35). The main limitation is the lack of virological confirmation of possible COVID-19 and the risk its misclassification. Moreover, we cannot exclude a recall bias despite the strong awareness, especially via media. Lastly, this study focuses on a specific population. The Parisian families being of a high SES, these findings cannot be generalized to all French families.
Conclusion
COVID-19 morbidity, stress and preventive measures were inter-related within families during the lockdown. Adolescents and their parents presented similar attitudes towards lockdown measures, even if adolescents were less compliant. This study underscores that media and relatives are a key prevention medium to focus on when informing adolescents. Improving information dissemination to adolescents and parents, including dedicated adolescent messages, would increase adherence to preventive measures.
Data Availability Statement
The datasets presented in this article are not readily available because the data analysis is still ongoing. Requests to access the datasets should be directed to the corresponding author (CR, celine.roda@u-paris.fr).
Ethics Statement
The studies involving human participants were reviewed and approved by French Ethic Committee. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
Author Contributions
AC: methodology, validation, formal analyses, writing—original draft, and visualization. FR and CR: conceptualization, methodology, validation, investigation, writing—review and editing, and supervision. IM: conceptualization, methodology, validation, investigation, writing—review and editing, supervision, project administration, and funding acquisition. All authors contributed to the article and approved the submitted version.
Funding
This work was supported by the Paris Municipal Department of Social Action, Childhood, and Health (DASES) and the French National Research Agency (ANR) [16-CE36-0007-01].
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We are grateful to all children and parents of the PARIS (Pollution and Asthma Risk: an Infant Study) birth cohort who participated in this study, and to the administrative staff (Dominique Viguier, Marianne Bijou, and Chimène Yimier) for their involvement in the PARIS cohort follow-up. We thank Agnès Lefranc and Claude Beaubestre for reviewing the questionnaires.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2022.907456/full#supplementary-material
References
1. WHO Timeline - COVID-19. Available online at: https://www.who.int/news/item/27-04-2020-who-timeline---COVID-19. (accessed 10 Feb 2022).
2. Carrat F, Touvier M, Severi G, Meyer L, Jusot F, Lapidus N, et al. Incidence and risk factors of COVID-19-like symptoms in the French general population during the lockdown period: a multi-cohort study. BMC Infect Dis. (2021) 21:169. doi: 10.1186/s12879-021-05864-8
3. Souty C, Guerrisi C, Masse S, Lina B, van der Werf S, Bernard-Stoecklin S, et al. Impact of the lockdown on the burden of COVID-19 in outpatient care in France, spring. (2020) Infect Dis. (2021) 53:376–81. doi: 10.1080/23744235.2021.1880024
4. Warszawski J, Beaumont A-L, Seng R, de Lamballerie X, Rahib D, Lydié N, et al. Prevalence of SARS-Cov-2 antibodies and living conditions: the French national random population-based EPICOV cohort. BMC Infect Dis. (2022) 22:41. doi: 10.1186/s12879-021-06973-0
5. Beaumont A, Durand C, Ledrans M, Schwoebel V, Noel H, Le Strat Y, et al. Seroprevalence of anti-SARS-CoV-2 antibodies after the first wave of the COVID-19 pandemic in a vulnerable population in France: a cross-sectional study. BMJ Open. (2021) 11:e053201. doi: 10.1136/bmjopen-2021-053201
6. Jannot A-S, Countouris H, Van Straaten A, Burgun A, Katsahian S, Rance B, et al. Low-income neighbourhood was a key determinant of severe COVID-19 incidence during the first wave of the epidemic in Paris. J Epidemiol Community Health. (2021) 75:1143–6. doi: 10.1136/jech-2020-216068
7. Gégout Petit A, Jeulin H, Legrand K, Jay N, Bochnakian A, Vallois P, et al. Seroprevalence of SARS-CoV-2, symptom profiles and sero-neutralization in a suburban area, France. Viruses. (2021) 13:1076. doi: 10.3390/v13061076
8. Lachassinne E, de Pontual L, Caseris M, Lorrot M, Guilluy C, Naud A, et al. SARS-CoV-2 transmission among children and staff in daycare centres during a nationwide lockdown in France: a cross-sectional, multicentre, seroprevalence study. Lancet Child Adolesc Health. (2021) 5:256–64. doi: 10.1016/S2352-4642(21)00024-9
9. Viner RM, Mytton OT, Bonell C, Melendez-Torres GJ, Ward J, Hudson L, et al. Susceptibility to SARS-COV-2 infection among children and adolescents compared with adults: a systematic review and meta-analysis. JAMA Pediatr. (2021) 175:143–56. doi: 10.1001/jamapediatrics.2020.4573
10. Irfan O, Li J, Tang K, Wang Z, Bhutta ZA. Risk of infection and transmission of SARS-CoV-2 among children and adolescents in households, communities and educational settings: a systematic review and meta-analysis. J Glob Health. (2021) 11:05013. doi: 10.7189/jogh.11.05013
11. Misra P, Kant S, Guleria R, Rai SK, Aiims WUS study team of. Serological prevalence of SARS-CoV-2 antibody among children and young age. (between age 2–17 years) group in India: an interim result from a large multi-centric population-based seroepidemiological study. MedRxiv. (2021) 06:15. doi: 10.1101/2021.06.15.21258880
12. Madewell ZJ, Yang Y, Longini IM, Halloran ME, Dean NE. Factors associated with household transmission of SARS-CoV-2: an updated systematic review and meta-analysis. JAMA Netw Open. (2021) 4:e2122240. doi: 10.1001/jamanetworkopen.2021.22240
13. Viner R, Waddington C, Mytton O, Booy R, Cruz J, Ward J, et al. Transmission of SARS-CoV-2 by children and young people in households and schools: a meta-analysis of population-based and contact-tracing studies. J Infect. (2021) 84:361–82. doi: 10.1016/j.jinf.2021.12.026
14. Galow L, Haag L, Kahre E, Blankenburg J, Dalpke AH, Lück C, et al. Lower household transmission rates of SARS-CoV-2 from children compared to adults. J Infect. (2021) 83:e34–6. doi: 10.1016/j.jinf.2021.04.022
15. Jing Q-L, Liu M-J, Zhang Z-B, Fang L-Q, Yuan J, Zhang A-R, et al. Household secondary attack rate of COVID-19 and associated determinants in Guangzhou, China: a retrospective cohort study. Lancet Infect Dis. (2020) 20:1141–50. doi: 10.1016/S1473-3099(20)30471-0
16. Clarisse B, Nikasinovic L, Poinsard R, Just J, Momas I. The Paris prospective birth cohort study: which design and who participates? Eur J Epidemiol. (2007) 22:203–10. doi: 10.1007/s10654-007-9109-2
17. ECDC. Case Definition for Coronavirus Disease. (2019). (COVID-19), as of 3 December. (2020) European Centre for Disease Prevention and Control. (2020) Available online at: https://www.ecdc.europa.eu/en/covid-19/surveillance/case-definition. (accessed Feb 10, 2022).
18. Warszawski J, Bajos N, Meyer L, de Lamballerie X, Seng R, Beaumont A-L, et al. En mai. (2020) 4, 5% de la Populationen France Métropolitaine a Développédes Anticorps Contre le SARS-CoV-2. Premiers Résultats de L'enquête Nationale EpiCov. Direction de la Recherche, Des études, de L'évaluation et des Statistiques. (DREES). (2020) Available online at: https://www.epicov.fr/wp-content/uploads/2020/10/Warszawski-et-al-2020-Se%CC%81ropre%CC%81valence.pdf. (accessed Feb 10, 2022).
19. Chung E, Chow EJ, Wilcox NC, Burstein R, Brandstetter E, Han PD, et al. Comparison of symptoms and RNA levels in children and adults with SARS-CoV-2 infection in the community setting. JAMA Pediatr. (2021) 175:e212025. doi: 10.1001/jamapediatrics.2021.2025
20. de Souza TH, Nadal JA, Nogueira RJN, Pereira RM, Brandão MB. Clinical manifestations of children with COVID-19: a systematic review. Pediatr Pulmonol. (2020) 55:1892–9. doi: 10.1002/ppul.24885
21. O'Driscoll M, Ribeiro Dos Santos G, Wang L, Cummings DAT, Azman AS, Paireau J, et al. Age-specific mortality and immunity patterns of SARS-CoV-2. Nature. (2021) 590:140–5. doi: 10.1038/s41586-020-2918-0
22. Guan W, Ni Z, Hu Y, Liang W, Ou C, He J, et al. Clinical characteristics of coronavirus disease 2019 in China. New Eng J Med. (2020) 382:1708–20. doi: 10.1056/NEJMoa2002032
23. Wang J-G, Cui H-R, Tang H-B, Deng X-L. Gastrointestinal symptoms and fecal nucleic acid testing of children with 2019 coronavirus disease: a systematic review and meta-analysis. Sci Rep. (2020) 10:17846. doi: 10.1038/s41598-020-74913-0
24. Mantovani A, Rinaldi E, Zusi C, Beatrice G, Saccomani MD, Dalbeni A. Coronavirus disease. (2019). (COVID-19) in children and/or adolescents: a meta-analysis. Pediatr Res. (2021) 89:733–7. doi: 10.1038/s41390-020-1015-2
25. Cui X, Zhao Z, Zhang T, Guo W, Guo W, Zheng J, et al. A systematic review and meta-analysis of children with coronavirus disease. (2019). (COVID-19). J Med Virol. (2021) 93:1057–69. doi: 10.1002/jmv.26398
26. Thompson HA, Mousa A, Dighe A, Fu H, Arnedo-Pena A, Barrett P, et al. SARS-CoV-2 setting-specific transmission rates: a systematic review and meta-analysis. Clin Infect Dis. (2021) 3:e754–64doi: 10.1093/cid/ciab100
27. Madewell ZJ, Yang Y, Longini IM, Halloran ME, Dean NE. Household transmission of SARS-CoV-2. JAMA Netw Open. (2020) 3:e2031756. doi: 10.1001/jamanetworkopen.2020.31756
28. Cevik M, Tate M, Lloyd O, Maraolo AE, Schafers J, Ho SARS-CoV-2 A SARS-CoV and MERS-CoV viral load dynamics duration duration of viral shedding and infectiousness: a systematic review and meta-analysis. Lancet Microbe. (2021) 2:e13–22. doi: 10.1016/S2666-5247(20)30172-5
29. Spinelli M, Lionetti F, Pastore M, Fasolo M. Parents' stress and children's psychological problems in families facing the COVID-19 outbreak in Italy. Front Psychol. (2020)11:1713. doi: 10.3389/fpsyg.2020.01713
30. Freeman JL, Caldwell PHY, Scott KM. The role of trust when adolescents search for and appraise online health information. J Pediatr. (2020) 221:215–23.e5. doi: 10.1016/j.jpeds.2020.02.074
31. Neufcourt L, Joannèes C, Maurel M, Kelly-Irving M, Delpierre C. EPIDEMIC – Le Respect des Gestes Barrières Face au Covid-19, Synthèse du 01/07/2020. Programme Interdisciplinaire EPIDEMIC – IFERISS FED4142, Toulouse Published Online First. (2020) Available online at: http://www.iferiss.org/images/IFERISS/Projets/EPIDEMIC/Synthese_EPIDEMIC_Gestes-Barrieres_010720.pdf (accessed July 1, 2020).
32. Cobham VE, McDermott B, Haslam D, Sanders MR. The role of parents, parenting and the family environment in children's post-disaster mental health. Curr Psychiatry Rep. (2016) 18:53. doi: 10.1007/s11920-016-0691-4
33. Oosterhoff B, Palmer C. Attitudes and psychological factors associated with news monitoring, social distancing, disinfecting, and hoarding behaviors among US adolescents during the coronavirus disease. (2019) Pandemic. JAMA Pediatr. (2020) 174:1184–90. doi: 10.1001/jamapediatrics.2020.1876
34. Brooks SK, Webster RK, Smith LE, Woodland L, Wessely S, Greenberg N, et al. The psychological impact of quarantine and how to reduce it: rapid review of the evidence. Lancet. (2020) 395:912–20. doi: 10.1016/S0140-6736(20)30460-8
Keywords: adolescents, birth cohort, cluster analysis, COVID-19, household transmission, preventive measures, stress, COVID-19 lockdown
Citation: Citerne A, Rancière F, Roda C and Momas I (2022) Coronavirus Disease 2019 (COVID-19) Lockdown: Morbidity, Perception, Behaviors, and Attitudes in French Families From the PARIS Birth Cohort. Front. Public Health 10:907456. doi: 10.3389/fpubh.2022.907456
Received: 29 March 2022; Accepted: 20 April 2022;
Published: 24 May 2022.
Edited by:
Luigi Vimercati, University of Bari Aldo Moro, ItalyReviewed by:
Iman H. Kamel, National Research Centre, EgyptMirosława Huflejt-Łukasik, University of Warsaw, Poland
Copyright © 2022 Citerne, Rancière, Roda and Momas. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Célina Roda, celine.roda@u-paris.fr
†These authors have contributed equally to this work and share last authorship