 Wandrey Roberto dos Santos Brito1,2Greice de Lemos Cardoso-Costa2,3Lourival Marques Roland Junior2,4Keise Adrielle Santos Pereira1,2Felipe Teixeira Lopes1,2
Wandrey Roberto dos Santos Brito1,2Greice de Lemos Cardoso-Costa2,3Lourival Marques Roland Junior2,4Keise Adrielle Santos Pereira1,2Felipe Teixeira Lopes1,2 Bernardo Cintra dos Santos1Aline Cecy Rocha de Lima1,2Isabella Nogueira Abreu1,2Carlos Neandro Cordeiro Lima1,2
Bernardo Cintra dos Santos1Aline Cecy Rocha de Lima1,2Isabella Nogueira Abreu1,2Carlos Neandro Cordeiro Lima1,2 Sandra Souza Lima1
Sandra Souza Lima1 Izaura M. Vieira Cayres Vallinoto1,2
Izaura M. Vieira Cayres Vallinoto1,2 Eduardo José Melo dos Santos2,4João Farias Guerreiro3
Eduardo José Melo dos Santos2,4João Farias Guerreiro3 Antonio Carlos Rosário Vallinoto1,2*
Antonio Carlos Rosário Vallinoto1,2*- 1Laboratory of Virology, Institute of Biological Sciences, Federal University of Pará, Belém, Brazil
- 2Postgraduate Program in Biology of Infectious and Parasitic Agents, Institute of Biological Sciences, Federal University of Pará, Belém, Brazil
- 3Laboratory of Human and Medical Genetics, Institute of Biological Sciences, Federal University of Pará, Belém, Brazil
- 4Laboratory of Genetics of Complex Diseases, Institute of Biological Sciences, Federal University of Pará, Belém, Brazil
Human T-lymphotropic viruses 1 and 2 (HTLV-1 and HTLV-2) are retroviruses that originated on the African continent and dispersed throughout other continents through human migratory flows. This study describes the prevalence of HTLV-1 and HTLV-2 infection in residents of 11 quilombo remnant communities in the state of Pará, Brazil, and the associated risk factors. A total of 859 individuals (334 men and 525 women), aged between 7 and 91 years, participated in the study. All subjects answered a questionnaire with questions on sociodemographic characteristics and on risk factors associated with HTLV infection, and blood samples were collected and separated into plasma and leukocytes. An immunoenzymatic assay (ELISA; Murex HTLV-I+II, DiaSorin, Dartford, UK) was used as a screening test, and positive samples were subjected to line immunoassay confirmatory tests (Inno-LIA HTLV I/II Score FUJIREBIO) and DNA extraction for subsequent real-time PCR to differentiate the viral type. Four of the 859 individuals were seropositive for HTLV. HTLV-1 infection was confirmed in one individual from the Itamoari community (0.92%), and HTLV-2 infection was confirmed in two individuals from São Benedito (3.17%) and in one individual from Arimandeua (2.22%). Blood transfusion was the only risk factor associated with HTLV infection in this study. This study reports the occurrence of HTLV-1 and HTLV-2 in quilombo remnant communities in the state of Pará. Considering the African origin of the virus and its introduction into Brazil from the slave trade, the continued evaluation of quilombola communities in the state of Pará is essential to better characterize the distribution of infections in these populations and to create public health policies for the control of the spread of the virus and associated diseases.
Introduction
Human T-lymphotropic viruses 1 (HTLV-1) and 2 (HTLV-2) were the first isolated retroviruses to infect humans (1, 2). They are viruses with known tropism for T lymphocytes and belong to the family Retroviridae, subfamily Orthoretrovirinae, and genus Deltaretrovirus (3–5). Evidence suggests an African origin for both viruses from independent events of interspecies transmission of the simian T-lymphotropic virus (STLV-1 and STLV-2) from non-human primates to humans (6–8). HTLV-1 has been associated with several diseases, particularly a neoplasm, i.e., adult T cell leukemia/lymphoma (ATLL), and an inflammatory neurodegenerative disease, i.e., HTLV-1-associated myelopathy (HAM) (9–11). In addition, HTLV-1 is also associated with ocular (uveitis) (12, 13), rheumatologic (14) and pulmonary (15, 16) diseases, among other pathologies (17–19). HTLV-2, in turn, does not have clinical manifestations necessarily associated with infection; however, clinical symptoms have been described in some patients (20, 21).
The main forms of HTLV-1/2 transmission are unprotected sex (22, 23), blood transfusion (24), sharing syringes and needles (25), and vertical transmission, in particular, prolonged breastfeeding (26, 27). HTLV-1 is widely distributed in geographic areas such as sub-Saharan Africa, Japan, Melanesia, the Caribbean, and South America (28–31). HTLV-2 has a more restricted distribution to pygmy populations in Africa and to indigenous peoples of the Americas, especially in the Brazilian Amazon region (7, 8, 32–36).
The entry of HTLV-1 into Brazil must have occurred along the east coast of the country, between the 16th and 19th centuries, through the African slave trade (37, 38). HTLV-2 may have followed the oldest human migratory flows that occurred thousands of years ago from the Asian continent via the Bering Strait, reaching North America and moving toward South America and, thus, Brazil (35, 37, 39). In Brazil, the viruses are distributed throughout the territory, and the main foci of infection are found in the North and Northeast regions (40). In the North region of the country, in the state of Pará, HTLV-1, and HTLV-2 have been described in several population strata, including urban, rural, and riverine populations, blood donors, and pregnant women, in addition to the presence of coinfections in people living with HIV (PLHIV), intravenous drug users, and isolated populations such as indigenous and quilombola peoples (25, 41–47). During the colonial period in Brazil, enslaved blacks in search of freedom fled coffee and sugarcane farms to the forest interior, where they formed isolated societies called quilombos. In the state of Pará, there are indications that quilombos formed in the 18th century, of which many were formed on the banks of rivers, such as the Gurupi, Tocantins, and Trombetas rivers (48). Many quilombo remnant communities lack basic sanitation, which promotes the transmission of diseases and fosters precarious health conditions; thus, this is one of the most vulnerable populations in Brazil (49–51). Infections by HTLV-1 and HTLV-2 have already been described in quilombo remnant communities in the Marajó Archipelago (43), but there are no studies on these viruses in other quilombos in the state of Pará. Thus, the aim of this study was to describe the prevalence of HTLV-1 and HTLV-2 and the main risk factors in 11 quilombola communities in the state of Pará.
Materials and Methods
Study Population and Sample Collection
A total of 11 quilombola communities located in the state of Pará (northern Brazil) were visited from September 2020 to April 2021, and information was collected from 859 individuals. The following communities were studied: Poeirinha (n = 20), Umarizal Beira (n = 303), Arimandeua (n = 45), Aripijó (n = 31), Bacuri (n = 10), Cabanagem (n = 17), São Benedito (n = 63), Bela Aurora (n = 35), Camiranga (n = 89), Itamoari (n = 109), and Nova Jutaí (n = 137) (Figure 1).
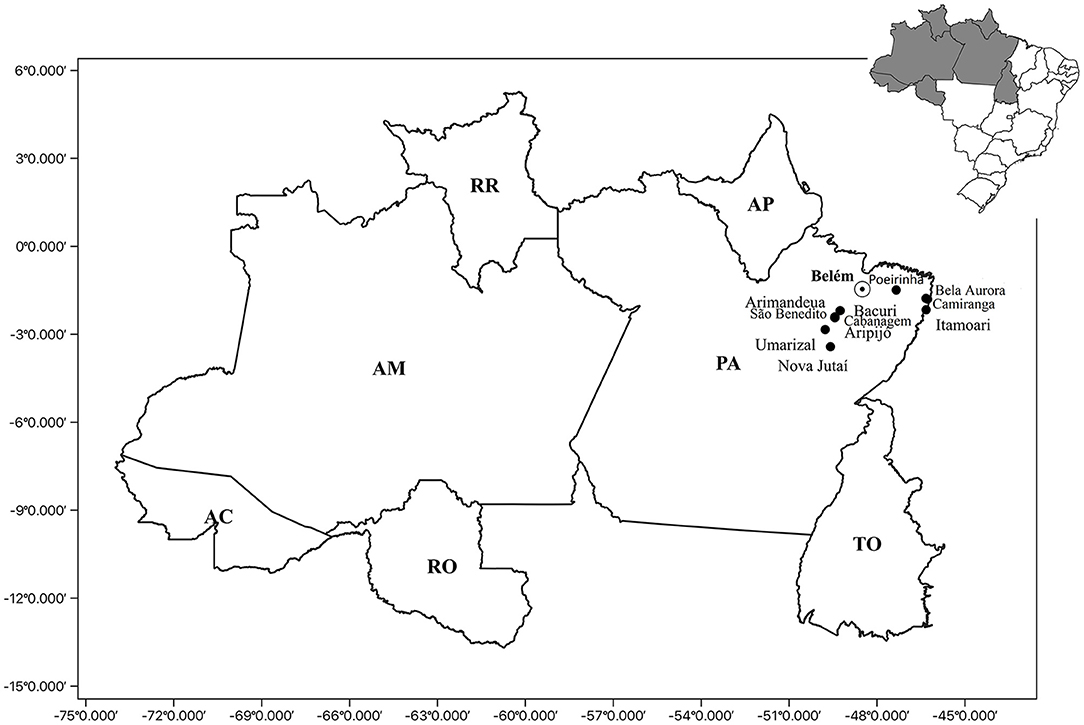
Figure 1. Geographic location of the quilombolas communities: Poeirinha, municipality of Bonito; Bela Aurora, Camiranga and Itamoari, municipality of Cachoeira do Piriá; Arimandeua, Aripijó Bacuri, Cabanagem, and São Benedito, municipality of Cametá; Umarizal Beira, municipality of Baião; and Nova Jutaí, municipality of Breu Branco. PA, Para State; Belém, capital of the Para State; AP, Amapá State; TO, Tocantins State; RR, Roramia State; AM, Amazonas State; AC, Acre State; RO, Rondônia State.
All study participants signed an informed consent form and answered a questionnaire with questions about sociodemographic aspects (age, sex, marital status, education, and family income) and behavioral risk factors for exposure to HTLV (“tattoos,” “use of illicit drugs,” “blood transfusion,” “piercings,” “sexually active,” “use of condoms,” and “previous diagnosis of STI,” among others). Individuals under 18 years old signed an informed assent form, and their legal guardians signed an informed consent form.
From all participants, peripheral blood samples (4 mL) were collected in vacuum tubes containing ethylenediaminetetraacetic acid (EDTA) as an anticoagulant. The samples were then subjected to centrifugation to separate the plasma and leukocyte fractions, followed by storage at −20°C until use.
Ethical Aspects
This study was approved by the National Research Ethics Committee (CONEP, acronym in Portuguese) (CAAE: 27290619.2.0000.0018), in compliance with resolution 466/12 of the Ministry of Health, which regulates research involving human beings. All subjects who voluntarily agreed to participate in the study signed an informed consent form.
Serological Analysis
Immunoenzymatic assays (Murex HTLV-I+II, DiaSorin, Dartford, UK) were used to detect anti-HTLV-1/2 antibodies in the tested samples following the manufacturer's instructions. Samples with positive results were subjected to line immunoassays (INNO-LIA® HTLV I/II Score, Fujirebio, Japan) and real-time PCR (Applied Biosystems Step One Plus Real Time PCR) to confirm infection and differentiate the viral type, respectively.
Real-Time PCR
To perform real-time PCR, DNA was extracted from the seropositive samples using a QiaAmp DNA mini kit (Qiagen, Germany) following the manufacturer's protocol. Molecular confirmation of infection was performed using a multiplex real-time PCR for three target sequences: the albumin gene (141 bp), as an endogenous control; the pol gene (186 bp) of HTLV-1; and the tax-2 gene (75 bp) of HTLV-2. The primer sequences used were 5′-ccctacaatccaaccagctcag-3′ (HTLV-1F), 5′-gtggtgaagctgccatcgggtttt-3′ (HTLV-1R), 5′-cgattgtgtacaggccgattg-3′ (HTLV-2F), 5′-caggagggcatgtcgatgtag-3′ (HTLV-2R), 5′-gctgtcatctcttgtgggctgt-3′ (F Albumin), 5′-aaactcatgggagctgctggtt-3′ (R Albumin); the probe sequences used were JOE-5′-ctttactgacaaacccgacctacccatgga-3′-BHQ (HTLV-1), FAM-5′-tgtcccgtctcaggtggtctatgttcca-3′-MGB (HTLV-2), and NED-5′-cctgtcatgcccacacaaatctc-3′-MGB (albumin). The reaction components, based on the TaqMan® Universal system, were as follows: 12.5 μL of Master Mix, 6.0 μL of water, 1.0 μL of Assay-by-Design (primer and probe set) and 0.5 μL of DNA in a final volume of 20 μL. For cycling, the protocol was as follows: 50°C for 2 min; 95°C for 10 min; and 50 cycles of 90°C for 50 s and 60°C for 1 min.
Statistical Analyses
The collected information was stored in a database using Epi-Info7.2 software. The socioeconomic aspects, behavioral factors, and risk factors for exposure to HTLV-1 and HTLV-2 are described as frequencies and percentages. The confidence interval (95% CI) was used to estimate overall and community prevalence. Fisher's exact test was used to evaluate the association of behavioral risk factors with the presence/absence of HTLV-1 or HTLV-2. The significance level adopted was 5%. Statistical analyses were performed using the programs BioEstat 5.3, GraphPad Prism 7.0 for Windows, and MINITAB Release 14 for Windows.
Results
The median age of the individuals was 39 years (IIQ: 32); 61.1% (n = 525) of the individuals were women, and 38.9% (n = 334) were men. A total of 49.9% (n = 429) of the individuals said they were married/living with a partner. Most of these individuals declared themselves black (60.5%; n = 520) and brown (33.5%; n = 288). Regarding education, 40.6% (n = 349) were literate, 16.5% (142) had completed elementary school, and 28.4% (n = 244) had completed secondary education. A total of 46.6% (n = 400) live on <1 (1) minimum wage, and 47.1% (n = 405) live on one (2) to three (3) minimum wages (Table 1).
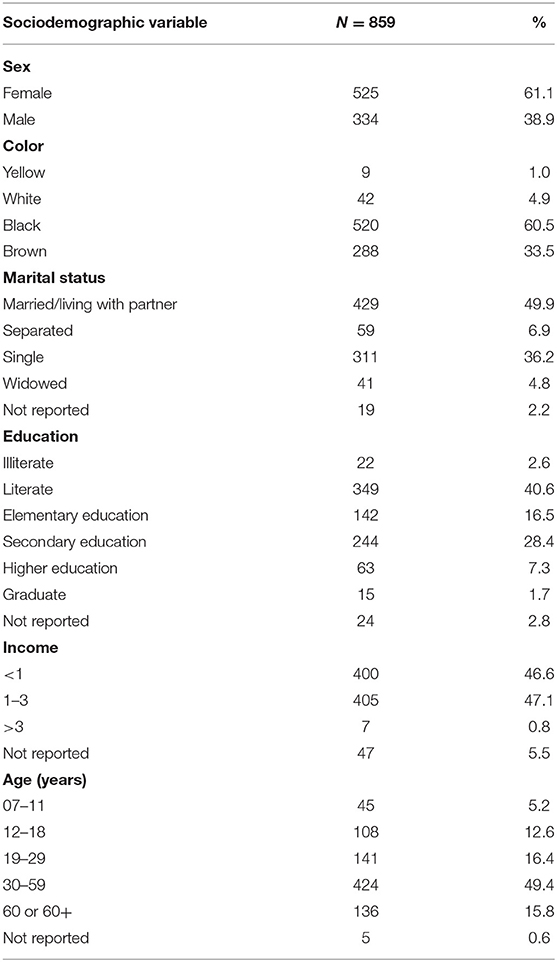
Table 1. Sociodemographic profile of the study participants.
HTLV-1/2 infection was detected in four individuals (0.4%, 95% CI: 0.13–1.19). Table 2 provides the distribution of infection by community, with 3.2% (2/63) of those tested in São Benedito (95% CI: 0.38–11) and 2.2% (1/45) of those tested in Arimandeua (95% CI: 0.05–11) being positive for HTLV-2 infection and 0.9% (1/109) of those tested in Itamoari (95% CI: 0.02–5.00) being positive for HTLV-1 infection; all of the communities are located in the northeastern region of the state of Pará. HTLV-1 infection was identified in a young, 24-year-old male. Two males and one female were diagnosed with HTLV-2; all three were over 60 years of age.
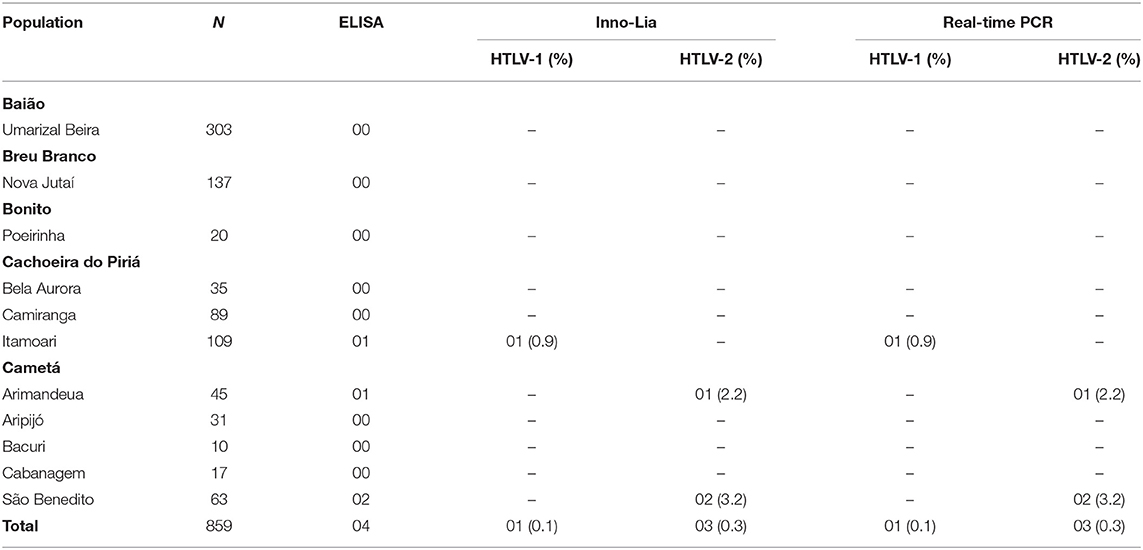
Table 2. Prevalence of HTLV-1 and HTLV-2 in the communities based on the tests used.
Only the individual diagnosed with HTLV-1 infection reported having a tattoo (25%). Three individuals (75%) denied having used illicit drugs, and one did not report anything. All of them denied having piercings, a previous diagnosis of an STI, or having more than one sexual partner. Two (50%) of those infected reported having received blood transfusions. Half (2) of the diagnosed individuals were sexually active and used condoms during sexual intercourse. Three (75%) of the individuals were breastfed, and one individual did not know (Table 3). According to Fisher's exact test, there was a significant association between blood transfusion (p = 0.0176) and HTLV-1/2 infection, with no association with any of the other factors investigated (Table 4).
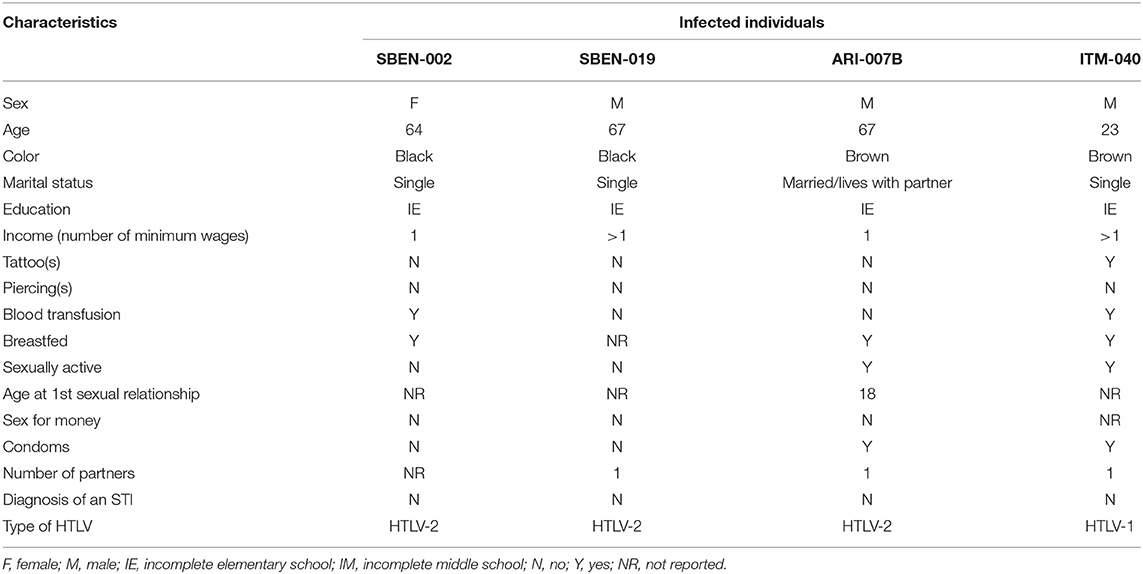
Table 3. Sociodemographic and behavioral characteristics of individuals with confirmed HTLV-1 and HTLV-2 infection.
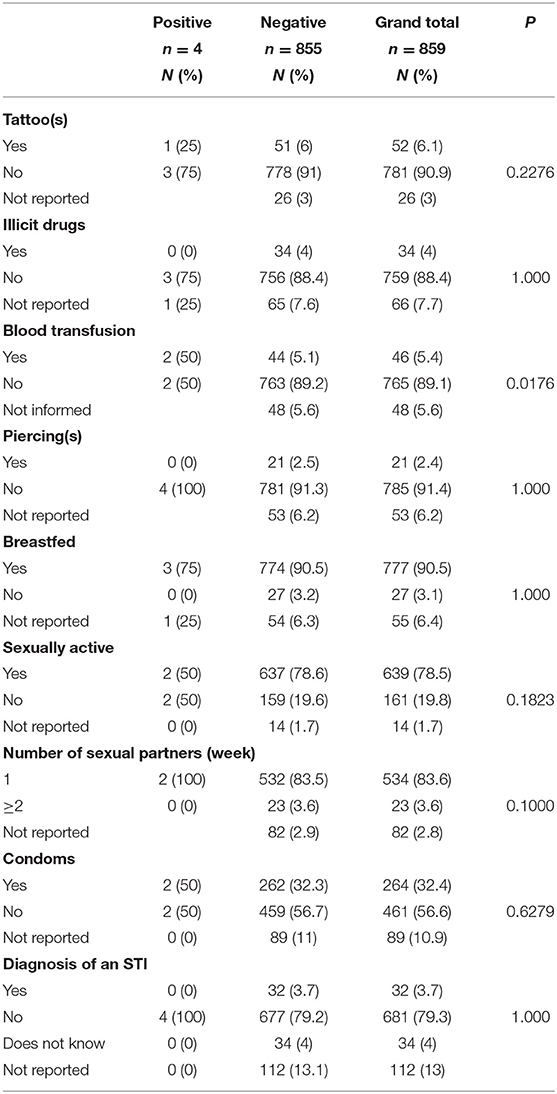
Table 4. Association of HTLV-1/2 infection with behavioral risk factors.
Discussion
Herein, we report the occurrence of anti-HTLV-1/2 antibodies in four of the 859 individuals tested, with confirmed HTLV-1 infection in only one resident of the Itamoari community and confirmed HTLV-2 infection in two communities—Arimandeua and São Benedito. This is the first time that HTLV-1 and HTLV-2 have been identified in these communities, and no previous studies have been conducted in these communities.
Vallinoto et al. (43) found that the prevalence rate of HTLV-1 in quilombolas of the Marajó Archipelago (Pará) ranged from 1.0% in the Ponta de Pedras community to 2.06% in Santana do Arari; these numbers are close to those found in this study. Regarding the prevalence of HTLV-2, the rates found in this study were also similar to those described in Santana do Arari (1.06%). Regarding other Afro-descendant populations studied in Brazil, the prevalence of HTLV-1 in the present study was similar to that found in quilombo remnant communities in Central Brazil (0.5%) (52).
The prevalence of HTLV-2 in the present study was lower than that reported by other studies involving traditional populations of Pará, such as indigenous populations. The prevalence in three Kayapó villages in the Xikrin territory was 29%, ranging from 21 to 38% among the villages (41). In turn, the prevalence data for this study are consistent with the data for the population of Belém, the capital of Pará, and for blood donors in this same state (42, 44).
Itamoari is a community located on the Pará side of the Gurupi River. The Gurupi River and the Turiaçu River (State of Maranhão) form a region called Turiaçu. The port in this region served as an entrance for a large number of slave through illegal slave trade during the 19th century (48). In this sense, the occurrence of HTLV-1 in the Itamoari community may be related to the African origin of the virus, and its entry into Brazil may have been by the slave trade from the African continent, considering that cases occur in isolated communities.
There are historical reports (48) that slaves sometimes found indigenous tribes during their escape into forests and lived with residents in locations highly endemic for HTLV-2 (48). Thus, the detection of HTLV-2 in São Benedito and Arimandeua can be attributed to the contact between indigenous populations and slaves.
History of an STI, multiple sexual partners, and non-use of condoms are risk factors that have been associated with a higher risk of HTLV-1/2 infection; however, in the present study, no associations were found (23, 25, 53). Nevertheless, two individuals infected with HTLV-2 reported not using condoms because they were no longer sexually active, leading to the hypothesis or inference that they did not use condoms in previous relationships. None of the four infected had any history of an STI or reported having more than one sexual partner.
Blood transfusion was a risk factor for HTLV-1/2 infection in this study as well as in other studies (54, 55). In November 1993, the Brazilian Ministry of Health filed Ordinance No. 1,376, through which blood donation candidates are subjected to clinical screening, including HTLV screening, to ensure their safety and that of recipients (56). Of the two individuals who reported receiving blood transfusions, the resident of São Benedito reported that this procedure was performed in 1994, while the other did not provide the date on which the transfusion was received. Because clinical screening was established shortly before the woman with HTLV-2 was transfused, there is no certainty as to whether she received screened blood, and thus, the transfusion may have been a source of infection. However, the association with blood transfusion could be a spurious result if we consider the small number of HTLV-1/2 positive subjects found in the present study, which could be considered a limitation of our study.
All three HTLV-2-infected patients have one surname in common; thus, it is possible that there is some degree of kinship between them due to the isolation of these communities. In addition, the 67-year-old woman who was infected reported that she had 11 pregnancies and breastfed all of her children for more than 6 months. However, her children could not be found to be tested, and thus, it is not known whether there was vertical transmission of the virus or if her infection occurred after her pregnancies. A new visit to the community is being arranged to investigate intrafamily transmission.
Although most of those infected with HTLV-1 are asymptomatic, this virus is associated with clinical manifestations that can lead to severe symptoms and death, and there is no cure or treatment available for the infection, which is neglected, not only in Brazil but also in several regions of the world (57). Therefore, HTLV-1/2 infection is a public health problem, especially in vulnerable populations (40, 57).
Although many Brazilian population segments are in a situation of vulnerability, there is a higher prevalence of black populations among the vulnerable populations, including those living in quilombo remnant communities (49, 58). These populations are vulnerable because of health determinants of individual control (behaviors) and collective control (low health conditions and poor infrastructure). Thus, measures such as (i) providing prenatal screening, (ii) providing screening for infection in different quilombola communities, (iii) performing confirmatory tests, (iv) increasing the awareness of the population about the virus and its modes of transmission, (v) encouraging the use of condoms, and (vi) providing counseling for infected pregnant women about the risk of transmission to the child through breastfeeding are means that can mitigate the transmission of HTLV in these communities; these actions promote health promotion/prevention from the perspective of comprehensive care, which is in line with the national policy of comprehensive health for the black population (59).
Conclusions
Considering the occurrence of HTLV-1/2 infection in populations associated with the African origin of the virus and its introduction into Brazil from the slave trade, the continuous evaluation of quilombola communities in the state of Pará and other locations in the Brazilian Amazon is needed to better characterize the distribution (prevalence) of infection in these populations to better formulate public health policies to control the spread of the virus and associated diseases.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by Human Research Ethics Committee of the Health Sciences Institute of the Federal University of Pará (CAAE: 55699316.6.0000.0018). The patients/participants provided their written informed consent to participate in this study.
Author Contributions
AV, JG, ES, IC, and GC-C conceived and designed the study. WB, LR, KP, FL, IA, CL, and AL assisted in subject recruitment and sample collection. BS, FL, WB, IA, and CL performed the serological and molecular analyses. SL and WB performed statistical analyses. WB, GC-C, IC, and AV wrote the manuscript. All authors read and approved the final manuscript.
Funding
This study was supported by the National Council for Scientific and Technological Development (CNPq; # 301869/2017-0; 442522/2019-3) and the Federal University of Pará(PAPQ-2022).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We thank all the individuals who agreed to participate in this study.
References
1. Poiesz BJ, Ruscetti FW, Gazdar AF, Bunn PA, Minna JD, Gallo RC. Detection and isolation of type C retrovirus particles from fresh and cultured lymphocytes of a patient with cutaneous T-cell lymphoma. Proc Natl Acad Sci U S A. (1980) 77:7415–9. doi: 10.1073/pnas.77.12.7415
2. Kalyanaraman VS, Sarngadharan MG, Robert-Guroff M, Miyoshi I, Golde D, Gallo RC. A new subtype of human T-cell leukemia virus (HTLV-II) associated with a T-cell variant of hairy cell leukemia. Science. (1982) 218:571–3. doi: 10.1126/science.6981847
3. Ijichi S, Ramundo MB, Takahashi H, Hall WW. In vivo cellular tropism of human T cell leukemia virus type II (HTLV-II). J Exp Med. (1992) 176:293–6. doi: 10.1084/jem.176.1.293
4. Richardson JH, Edwards AJ, Cruickshank JK, Rudge P, Dalgleish AG. In vivo cellular tropism of human T-cell leukemia virus type 1. J Virol. (1990) 64:5682–7. doi: 10.1128/jvi.64.11.5682-5687.1990
5. International Committee on Taxonomy of Viruses. Taxonomy History (ICTV): Primate T-Lymphotropic Virus 1 (2019). Available online at: https://talk.ictvonline.org/taxonomy/p/taxonomy-history?taxnode_id=202004999 (acessed October 18, 2019).
6. Koralnik IJ, Boeri E, Saxinger WC, Monico AL, Fullen J, Gessain A, et al. Phylogenetic associations of human and simian T-cell leukemia/lymphotropic virus type I strains: evidence for interspecies transmission. J Virol. (1994) 68:2693–707. doi: 10.1128/jvi.68.4.2693-2707.1994
7. Gessain A, Mauclère P, Froment A, Biglione M, Le Hesran JY, Tekaia F, et al. Isolation and molecular characterization of a human T-cell lymphotropic virus type II (HTLV-II), subtype B, from a healthy Pygmy living in a remote area of Cameroon: an ancient origin for HTLV-II in Africa. Proc Natl Acad Sci U S A. (1995) 92:4041–5. doi: 10.1073/pnas.92.9.4041
8. Vandamme AM, Salemi M, Van Brussel M, Liu HF, Van Laethem K, Van Ranst M, et al. African origin of human T-lymphotropic virus type 2 (HTLV-2) supported by a potential new HTLV-2d subtype in Congolese Bambuti Efe Pygmies. J Virol. (1998) 72:4327–40. doi: 10.1128/JVI.72.5.4327-4340.1998
9. Yoshida M, Miyoshi I, Hinuma Y. Isolation and characterization of retrovirus from cell lines of human adult T-cell leukemia and its implication in the disease. Proc Natl Acad Sci U S A. (1982) 79:2031–5. doi: 10.1073/pnas.79.6.2031
10. Osame M, Usuku K, Izumo S, Ijichi N, Amitani H, Igata A, et al. HTLV-I associated myelopathy, a new clinical entity. Lancet. (1986) 1:1031–2. doi: 10.1016/S0140-6736(86)91298-5
11. Ijichi S, Eiraku N, Osame M, Izumo S, Kubota R, Maruyama I, et al. Activated T lymphocytes in cerebrospinal fluid of patients with HTLV-I-associated myelopathy (HAM/TSP). J Neuroimmunol. (1989) 25:251–4. doi: 10.1016/0165-5728(89)90143-4
12. Chew R, Henderson T, Aujla J, Whist E, Einsiedel L. Turning a blind eye: HTLV-1-associated uveitis in Indigenous adults from Central Australia. Int Ophthalmol. (2018) 38:2159–62. doi: 10.1007/s10792-017-0659-3
13. Mochizuki M, Watanabe T, Yamaguchi K, Tajima K, Yoshimura K, Nakashima S, et al. Uveitis associated with human T lymphotropic virus type I: seroepidemiologic, clinical, and virologic studies. J Infect Dis. (1992) 166:943–4. doi: 10.1093/infdis/166.4.943
14. Nishioka K, Maruyama I, Sato K, Kitajima I, Nakajima Y, Osame M. Chronic inflammatory arthropathy associated with HTLV-I. Lancet. (1989) 1:441. doi: 10.1016/S0140-6736(89)90038-X
15. Einsiedel L, Chiong F, Jersmann H, Taylor GP. Human T-cell leukaemia virus type 1 associated pulmonary disease: clinical and pathological features of an under-recognised complication of HTLV-1 infection. Retrovirology. (2021) 18:5. doi: 10.1186/s12977-020-00543-z
16. Einsiedel L, Fernandes L, Spelman T, Steinfort D, Gotuzzo E. Bronchiectasis is associated with human T-lymphotropic virus 1 infection in an Indigenous Australian population. Clin Infect Dis. (2012) 54:43–50. doi: 10.1093/cid/cir766
17. Schierhout G, McGregor S, Gessain A, Einsiedel L, Martinello M, Kaldor J. Association between HTLV-1 infection and adverse health outcomes: a systematic review and meta-analysis of epidemiological studies. Lancet Infect Dis. (2020) 20:133–43. doi: 10.1016/S1473-3099(19)30402-5
18. Pinheiro SR, Lana-Peixoto MA, Proietti AB, Oréfice F, Lima-Martins MV, Proietti FA. HTLV-I associated uveitis, myelopathy, rheumatoid arthritis and Sjögren's syndrome. Arq Neuropsiquiatr. (1995) 53:777–81. doi: 10.1590/S0004-282X1995000500011
19. Vernant JC, Buisson G, Magdeleine J, De Thore J, Jouannelle A, Neisson-Vernant C, et al. T-lymphocyte alveolitis, tropical spastic paresis, and Sjögren syndrome. Lancet. (1988) 1:177. doi: 10.1016/S0140-6736(88)92744-4
20. Hjelle B, Appenzeller O, Mills R, Alexander S, Torrez-Martinez N, et al. Chronic neurodegenerative disease associated with HTLV-II infection. Lancet. (1992) 339:645–6. doi: 10.1016/0140-6736(92)90797-7
21. Jacobson S, Lehky T, Nishimura M, Robinson S, McFarlin DE, Dhib-Jalbut S. Isolation of HTLV-II from a patient with chronic, progressive neurological disease clinically indistinguishable from HTLV-I-associated myelopathy/tropical spastic paraparesis. Ann Neurol. (1993) 33:392–6. doi: 10.1002/ana.410330411
22. Paiva A, Casseb J. Sexual transmission of human T-cell lymphotropic virus type 1. Rev Soc Bras Med Trop. (2014) 47:265–74. doi: 10.1590/0037-8682-0232-2013
23. Murphy EL, Figueroa JP, Gibbs WN, Brathwaite A, Holding-Cobham M, Waters D, et al. Sexual transmission of human T-lymphotropic virus type I (HTLV-I). Ann Intern Med. (1989) 111:555–60. doi: 10.7326/0003-4819-111-7-555
24. Okochi K, Sato H, Hinuma Y. A retrospective study on transmission of adult T cell leukemia virus by blood transfusion: seroconversion in recipients. Vox Sang. (1984) 46:245–53. doi: 10.1159/000466190
25. Oliveira-Filho AB, Araújo APS, Souza APC, Gomes CM, Silva-Oliveira GC, Martins LC, et al. Human T-lymphotropic virus 1 and 2 among people who used illicit drugs in the state of Pará, northern Brazil. Sci Rep. (2019) 9:14750. doi: 10.1038/s41598-019-51383-7
26. Ando Y, Nakano S, Saito K, Shimamoto I, Ichijo M, Toyama T, et al. Transmission of adult T-cell leukemia retrovirus (HTLV-I) from mother to child: comparison of bottle- with breast-fed babies. Jpn J Cancer Res. (1987) 78:322–4.
27. Wiktor SZ, Pate EJ, Rosenberg PS, Barnett M, Palmer P, Medeiros D, et al. Mother-to-child transmission of human T-cell lymphotropic virus type I associated with prolonged breast-feeding. J Hum Virol. (1997) 1:37–44.
28. Gessain A, Cassar O. Epidemiological aspects and world distribution of HTLV-1 infection. Front Microbiol. (2012) 3:388. doi: 10.3389/fmicb.2012.00388
29. Einsiedel LJ, Pham H, Woodman RJ, Pepperill C, Taylor KA. The prevalence and clinical associations of HTLV-1 infection in a remote Indigenous community. Med J Aust. (2016) 205:305–9. doi: 10.5694/mja16.00285
30. Sagara Y, Iwanaga M, Morita M, Sagara Y, Nakamura H, Hirayama H, et al. Fine-scale geographic clustering pattern of human T-cell leukemia virus type 1 infection among blood donors in Kyushu-Okinawa, Japan. J Med Virol. (2018) 90:1658–65. doi: 10.1002/jmv.25239
31. Ramassamy JL, Cassar O, Toumbiri M, Diané A, Idam Mamimandjiami A, Bengone C, et al. High prevalence of human T-cell leukemia virus type-1b genotype among blood donors in Gabon, Central Africa. Transfusion. (2020) 60:1483–91. doi: 10.1111/trf.15838
32. Mauclère P, Afonso PV, Meertens L, Plancoulaine S, Calattini S, Froment A, et al. HTLV-2B strains, similar to those found in several Amerindian tribes, are endemic in central African Bakola Pygmies. J Infect Dis. (2011) 203:1316–23. doi: 10.1093/infdis/jir031
33. Leon-Ponte M, Noya O, Bianco N, Echeverría de Perez G. Highly endemic human T-lymphotropic virus type II (HTLV-II) infection in a Venezuelan Guahibo Amerindian group. J Acquir Immune Defic Syndr Hum Retrovirol. (1996) 13:281–6. doi: 10.1097/00042560-199611010-00011
34. Lowis GW, Sheremata WA, Wickman PR, Dube S, Dube K, Poiesz BJ. HTLV-II riskfactors in Native Americans in Florida. Neuroepidemiology. (1999) 18:37–47. doi: 10.1159/000026194
35. Vallinoto AC, Ishak MO, Azevedo VN, Vicente AC, Otsuki K, Hall WW, et al. Molecular epidemiology of human T-lymphotropic virus type II infection in Amerindian and urban populations of the Amazon region of Brazil. Hum Biol. (2002) 74:633–44. doi: 10.1353/hub.2002.0059
36. Ishak R, Harrington WJ Jr, Azevedo VN, Eiraku N, Ishak MO, Guerreiro JF, et al. Identification of human T cell lymphotropic virus type IIa infection in the Kayapo, an indigenous population of Brazil. AIDS Res Hum Retroviruses. (1995) 11:813–21. doi: 10.1089/aid.1995.11.813
37. Ishak R, Guimarães Ishak MO, Azevedo VN, Machado LFA, Vallinoto IMC, Queiroz MAF et al. HTLV in South America: origins of a silent ancient human infection. Virus Evol. (2020) 6:veaa053. doi: 10.1093/ve/veaa053
38. Aleluia MM, Mello MAG, Alcântara LCJ, Rego FFA, Santos LPS, Galvão-Castro B, et al. The origin of HTLV-1 in southern Bahia by phylogenetic, mtDNA and β-globin analysis. Virol Rep. (2015) 5:63–74. doi: 10.1016/j.virep.2015.05.002
39. Switzer WM, Black FL, Pieniazek D, Biggar RJ, Lal RB, Heneine W. Endemicity and phylogeny of the human T cell lymphotropic virus type II subtype A from the Kayapo Indians of Brazil: evidence for limited regional dissemination. AIDS Res Hum Retroviruses. (1996) 12:635–40. doi: 10.1089/aid.1996.12.635
40. Brasil. Prevalência da Infecção por HTLV-1/2no Brasil. Brasília: Ministério da Saúde. Boletim Epidemiológico. Secretaria de Vigilância em Saúde (2020).
41. Braço ILJ, de Sá KSG, Waqasi M, Queiroz MAF, da Silva ANR, Cayres-Vallinoto IMV, et al. High prevalence of human T-lymphotropic virus 2 (HTLV-2) infection in villages of the Xikrin tribe (Kayapo), Brazilian Amazon region. BMC Infect Dis. (2019) 19:459. doi: 10.1186/s12879-019-4041-0
42. Catalan-Soares B, Carneiro-Proietti AB, de F, Proietti FA. Heterogeneous geographic distribution of human T-cell lymphotropic viruses I andII (HTLV-I/II): serological screening prevalence rates in blood donorsfrom large urban areas in Brazil. Cad Saude Publica. (2005) 21:926–31. doi: 10.1590/S0102-311X2005000300027
43. Vallinoto ACR, Pontes GS, Muto NS, Lopes IGL, Machado LFA, Azevedo VN, et al. Identification of human T-cell lymphotropic virus infection in a semi-isolated Afro-Brazilianquilombo located in the Marajó Island (Pará, Brazil). Mem Inst Oswaldo Cruz. (2006) 101:103–5. doi: 10.1590/S0074-02762006000100020
44. Silva IC, Pinheiro BT, Nobre AFS, Coelho JL, Pereira CCC, Ferreira LSC, et al. Moderate endemicity of the human T-lymphotropic virus infection in the metropolitan region of Belém, Pará, Brazil. Rev Bras Epidemiol. (2018) 21:e180018. doi: 10.1590/1980-549720180018
45. Guerra AB, Siravenha LQ, Laurentino RV, Feitosa RNM, Azevedo VN, Vallinoto ACR, et al. Seroprevalence of HIV, HTLV, CMV, HBV and rubella virus infections in pregnant adolescents who received care in the city of Belém, Pará, Northern Brazil. BMC Pregnan Childbirth. (2018) 18:169. doi: 10.1186/s12884-018-1753-x
46. Ferreira LSC, Costa JHG, Costa CA, Melo MFC, Andrade ML, Martins LC, et al. Soroprevalência do vírus linfotrópico de células T humanas em comunidades ribeirinhas da região nordeste do Estado do Pará, Brasil. Rev Pan-Amaz Saude. (2010) 1:103–8. doi: 10.5123/S2176-62232010000300014
47. Alencar SP, Souza MC, Fonseca RRS, Menezes CR, Azevedo VN, Ribeiro ALR, et al. Prevalence and molecular epidemiology of human T-lymphotropic virus (HTLV) infection in people living with HIV/AIDS in the Pará State, Amazon Region of Brazil. Front Microbiol. (2020) 11:572381. doi: 10.3389/fmicb.2020.572381
48. Salles C. O Negro no Pará: Sob o Regime da Escravidão. Rio de Janeiro: Fundação Getúlio Vargas, Belém: UFPA (1971). 336 p.
49. Santos RP, França SAS, Arede ANF, Ramos EMLS. Condições Habitacionais e de Saúde da Comunidade Remanescente de Quilombo Mangueiras, Ilha Do Marajó, Pará, Brasil. RESMA. (2020) 10:43–59. Available online at: https://periodicos.ufms.br/index.php/sameamb/article/view/9145
50. Melo MFT, Silva HP. Doenças Crônicas e os Determinantes Sociais da Saúde em Comunidades Quilombolas do Pará, Amazônia, Brasil. Revista ABPN. (2015) 7:168–89. Available online at: http://www.abpnrevista.org.br/revista/index.php/revistaabpn1/article/view/103
51. Tavares RB, Silva HP. Educação Em Saúde E Ambiente Em Comunidades Quilombolas Do Pará/Brasil. Margens. (2016) 8:131–44. doi: 10.18542/rmi.v8i11.3246
52. Nascimento LB, Carneiro MAS, Teles SA, Lopes CLR, Reis RS, et al. Prevalência da infecção pelo HTLV-1, em remanescentes de quilombos no Brasil Central. Rev Soc Bras Med Trop. (2009) 42:657–60. doi: 10.1590/S0037-86822009000600009
53. Gotuzzo E, Sánchez J, Escamilla J, Carrillo C, Phillips IA, Moreyra L, et al. Human T cell lymphotropic virus type I infection among female sex workers in Peru. J Infect Dis. (1994) 169:754–9. doi: 10.1093/infdis/169.4.754
54. Hedayati-Moghaddam MR, Tehranian F, Bayati M. Human T-Lymphotropic Virus Type I (HTLV-1) infection among Iranian blood donors: first case-control study on the risk factors. Viruses. (2015) 7:5736–45. doi: 10.3390/v7112904
55. Santos RF, Conceição GC, Martins MS, Kraychete A, Penalva MA, Carvalho EM, et al. Prevalence and risk factors for Human T-Lymphotropic Virus Type 1 (HTLV-1) among maintenance hemodialysis patients. BMC Nephrol. (2017) 18:64. doi: 10.1186/s12882-017-0484-y
57. Rosadas C, Menezes MLB, Galvão-Castro B, Assone T, Miranda AE, Aragón MG, et al. Blocking HTLV-1/2 silent transmission in Brazil: Current public health policies and proposal for additional strategies. PLoS Negl Trop Dis. (2021) 15:e0009717. doi: 10.1371/journal.pntd.0009717
58. Mota AN, Maciel ES, Quaresma FRP, Araújo FA, Sousa LVA, et al. Um olhar para a vulnerabilidade: análise da ausência de acesso à saúde pelos quilombolas no Brasil. J Hum Growth. (2021) 31:302–9. doi: 10.36311/jhgd.v31.11404
Keywords: HTLV-1/2, Amazon, quilombos, epidemiology, vulnerable population
Citation: Brito WRdS, Cardoso-Costa GdL, Roland Junior LM, Pereira KAS, Lopes FT, Santos BCd, de Lima ACR, Abreu IN, Lima CNC, Lima SS, Cayres Vallinoto IMV, Santos EJMd, Guerreiro JF and Vallinoto ACR (2022) Prevalence and Risk Factors for HTLV-1/2 Infection in Quilombo Remnant Communities Living in the Brazilian Amazon. Front. Public Health 10:871865. doi: 10.3389/fpubh.2022.871865
Received: 08 February 2022; Accepted: 09 March 2022;
Published: 30 March 2022.
Edited by:
Yoav Keynan, University of Manitoba, CanadaReviewed by:
Roberta Bruhn, Vitalant Research Institute, United StatesFred Luciano Neves Santos, Gonçalo Moniz Institute (IGM), Brazil
Copyright © 2022 Brito, Cardoso-Costa, Roland Junior, Pereira, Lopes, Santos, de Lima, Abreu, Lima, Lima, Cayres Vallinoto, Santos, Guerreiro and Vallinoto. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Antonio Carlos Rosário Vallinoto, vallinoto@ufpa.br