 Paul Köbler1*
Paul Köbler1* Eva K. Krauss-Köstler1
Eva K. Krauss-Köstler1 Barbara Stein1Joachim H. Ficker2
Barbara Stein1Joachim H. Ficker2 Martin Wilhelm3Alexander Dechêne4
Martin Wilhelm3Alexander Dechêne4 Christiane Waller1
Christiane Waller1- 1Department of Psychosomatic Medicine and Psychotherapy, Paracelsus Medical Private University, Nuremberg General Hospital, Nuremberg, Germany
- 2Department of Internal Medicine 3, Respiratory Medicine, Paracelsus Medical Private University, Nuremberg General Hospital, Nuremberg, Germany
- 3Department of Internal Medicine 5, Oncology/Hematology, Paracelsus Medical Private University, Nuremberg General Hospital, Nuremberg, Germany
- 4Department of Internal Medicine 6, Gastroenterology, Paracelsus Medical Private University, Nuremberg General Hospital, Nuremberg, Germany
Introduction: Specialized biopsychosocial care concepts are necessary to overcome the dualism between physical and psychosocial treatment in acute care hospitals. For patients with complex and chronic comorbid physical and mental health problems, neither standardized psychiatric/psychosomatic nor somatic care units alone are appropriate to their needs. The “Nuremberg Integrated Psychosomatic Acute Unit” (NIPA) has been developed to integrate treatment of both, psychosocial and physical impairments, in an acute somatic care setting.
Method: NIPA has been established in inpatient internal medical wards for respiratory medicine, oncology and gastroenterology. One to two patients per ward are regularly enrolled in the NIPA treatment while remaining in the same inpatient bed after completion of the somatic care. In a naturalistic study design, we evaluated treatment effects by assessment of symptom load at admission and at discharge using the Patient Health Questionnaire (PHQ) and the Generalized Anxiety Disorder Scale-7 (GAD-7). Furthermore, we assessed the severity of morbidity using diagnosis data during treatment. At discharge, we measured satisfaction with treatment through the Patient Satisfaction Questionnaire (ZUF-8).
Results: Data from 41 NIPA patients were analyzed (18–87 years, 76% female). Seventy-eight percent suffered from at least moderate depression and 49% from anxiety disorders. Other diagnoses were somatoform pain disorder, somatoform autonomic dysfunction, eating disorder and posttraumatic stress disorder. Hypertension, chronic lung diseases and musculoskeletal disorders as well as chronic oncological and cardiac diseases were the most common somatic comorbidities. Treatment resulted in a significant reduction of depressive mood (admission: M = 10.9, SD = 6.1, discharge: M = 7.6, SD = 5.3, d = 0.58, p = 0.001), anxiety (admission: M = 10.6, SD = 4.9, discharge: M = 7.3, SD = 4.1, d = 0.65, p< 0.001) and stress (admission: M = 6.0, SD = 3.6, discharge: M = 4.1, SD = 2.5, d = 0.70, p< 0.001). Somatic symptom burden was reduced by NIPA treatment (admission: M = 10.9, SD = 5.8, discharge: M = 9.6, SD = 5.5, d = 0.30), albeit not statistically significant (p = 0.073) ZUF-8 revealed that 89% reported large or full satisfaction and 11% partial dissatisfaction with treatment.
Discussion: NIPA acute care is bridging the gap for patients in need of psychosocial treatment with complex somatic comorbidity. Further long-term evaluation will show whether psychosocial NIPA care is able to reduce the course of physical illness and hospital costs by preventing hospitalization and short-term inpatient re-admissions.
Introduction
Worldwide, there are proven and established treatment structures regarding somatic issues on one hand and psychosomatic-psychiatric care on the other. However, a high prevalence of mental comorbidities is present in patients with chronic and complex somatic diseases affecting daily clinical practice. Studies show regularly an elevated somatic comorbidity in people with psychiatric and psychosomatic diagnoses and higher rates of manifest mental illnesses in patients with physical disorders (1, 2).
A meta-analysis estimated the prevalence of clinically relevant depression in patients suffering from chronic obstructive pulmonary disease (COPD) to be 40% and the prevalence of anxiety and panic disorders to be 37% (3, 4). The prevalence of depressive disorders is estimated to be about 20% in patients with heart failure and coronary artery disease, which is 2 to 4 times higher than in the general population (5–7). Additionally, other diagnoses e.g. posttraumatic stress or bodily distress disorder are regularly seen in chronic physical diseases (8, 9). Other psychosomatic syndromes can also significantly increase the symptom severity and suffering in somatic diseases. Patients with, e.g. eating disorders, show a high prevalence of typical gastrointestinal symptoms such as constipation or diarrhea up to ileus-like symptoms which are difficult to treat without knowledge of the underlying psychosocial problems (10).
These observations lead to a constant adaptation of the health system to define and characterize psychosomatic complexity, which is represented by an update of the international classification of diseases. With new diagnostic entities (DSM V: Somatic Symptom Disorder, ICD 11: Bodily Distress Disorder), the high degree of overlap and mutual interaction of psychological and physical symptoms, especially in chronic conditions such as cardiovascular, lung or cancer diseases, is taken into account (11–14). Attention to these clinical phenomena is highly needed, considering elevated mortality rates, functional impairment and societal costs due to lost workdays and greater utilization of health care associated with psychiatric and psychosomatic comorbidity in somatic patients (15–17). In addition, prolonged hospitalization for mental disorders has been demonstrated for some constellations (18).
In everyday clinical practice, these implications can be observed frequently and in a wide variety of manifestations, e.g. intense anxiety reduces self-management skills in dealing with the somatic disease. This can be illustrated by COPD patients fearing physical exertion and therefore tend to be less willing to exercise or withdraw from active daily life due to fears of social stigmatization (19).
Depressive symptoms such as anhedonia or lack of interest, social withdrawal and sleep disturbances are associated with a significantly reduced quality of life of patients and result in an impaired ability to actively cope with the disease. Panic attacks occurring in the context of anxiety disorders with somatic comorbidity often lead to repetitive emergency room admission and inpatient treatment, increasing the risk of worsening the underlying chronic disease. Recent research has shown that depressive symptoms are associated with a higher risk of COPD exacerbation and poorer prognosis and therefore highlights the need for psychotherapeutic (co-) treatment (19–21). Strong associations between psychological distress and treatment results, disease progression, and quality of life have also been shown for coronary artery disease (7, 22). Both depressive and anxiety disorders are associated with an increased risk of cardiovascular morbidity and mortality [e.g. (23)]. Accordingly, the related statement of the German Society of Cardiology explicitly recommends psychotherapeutic interventions to address these associations (24). Furthermore, there are patients with somatization on internal wards, who show twice as many utilizations and medical care costs than non-somatizing patients (25).
Psychiatric and psychosomatic comorbidities are usually not diagnosed in the common somatic setting, so that these disorders often become chronic (15, 26–28) and result in repetitive and mismatched inpatient admission and treatment with increasing overall financial costs for the health system (29, 30). These patients have rather the problem of refused admission to medical wards (when mental comorbidity is striking) and to psychosomatic or psychiatric wards (when somatic symptoms are too severe) and sometimes even suffer from premature discharge because of difficulties in treatment within the framework of traditional care structures (31). When psychosomatic or psychiatric comorbidities interfere with care, treatment staff can quickly become overwhelmed, which in turn leads to shortages of care for this patient population (32).
According to Huyse and Stiefel, complex medically ill patients benefit from “complexity models, such as the biopsychosocial model—which focuses more on interactions such as compliance, the quality of the patient–doctor relationship, or interdependence between psychological stressors and physical disorders, rather than on separate disease identities [to] enrich the quality of service delivery to these patient groups” [(33), p. 257].
Biopsychosocial Inpatient Treatment Models
Following a short overview of the existing integrated care models and their development, the NIPA concept is presented as an innovative psychosomatic treatment unit and sorted into the previous models in terms of its ability to close the gap in biopsychosocial care for the chronically and complex medically ill. Initial clinical data evaluating treatment effect complete the report.
There have been efforts around the world in recent decades to enhance integrated care models, which are defined as coordinated care between general and mental health as well as social service disciplines. There is a wide range of models that differ in terms of the manner of collaboration between these care providers (34). Inpatient integrated treatment is particularly necessary when outpatient care is insufficient due to the severity, complexity or acute nature of the complaints and when multimodal treatment is needed (1). The first milestone in this integrated perspective was the development and expansion of consultation and liaison services (C-L) of psychiatry in general hospitals, which was started in the 1950s/60s in the USA and established in the following decades in Europe, Asia and Oceania as well as in South America (35). There are also forms of integration that provide for physical health liaison within mental health settings (36). Kathol et al. present a four-level categorization of integrated treatment models, which are termed Medical Psychiatry Units or Psychiatric Medicine Units, and are referenced by treatment programs worldwide (37). Type I and Type II follow the traditional approach and are most likely to be represented by psychiatric wards with somatic C-L support (Type I) or general hospital wards with psychiatric C-L support (Type II) (38, 39). Type III and IV would care for patients with moderate to severe psychiatric and somatic symptom severity in a stronger organizational integration whereas Type IV units “can diagnose and treat the same medical problems as general-medicine wards, regardless of the severity, together with any psychiatric condition generally handled in an acute-care psychiatric ward” [(31), p. 355]. Since the type definitions overlap and are sometimes not distinctive enough (40), the summarizing term Complexity Intervention Unit, which was introduced by Kathol et al. in 2009 (41) seems more appropriate for all these units providing more integrated biopsychosocial care. All over the world these kinds of clinical organizations were developed, differing in administration (psychiatry or general medicine), location (e.g., public, academic or private hospital) and specification (e.g., specific chronic conditions or disorders) (42). The vast majority of these units are more or less large bed units that allow for multimodal treatment of mental as well as somatic comorbidities (e.g., by lockable rooms on the one hand and oxygen supplies on the other). Illustrative examples can be found, among many others, in Alberque et al. (31) (USA), Wullschleger et al. (43) (Switzerland), Buckley et al. (44) (Ireland), Leue et al. (45) (Netherlands), Gertler et al. (46) (Australia) or Nomura et al. (47) (Japan). The most numerous efforts in this regard are directed toward the integrated care of severe mental illnesses especially schizophrenia, bipolar disorder and major depressive disorder (2, 48).
In Germany, a particular development of integrated medicine influenced by psychodynamic theory resulted in the establishment of the independent medical specialty of psychosomatic medicine with its distinct care units (35, 49). Modern psychosomatic therapy has since integrated a variety of method- and disorder-specific techniques drawn from a number of approved therapeutic disciplines (50). Comparable developments of independent psychosomatic specialties can be found in a number of countries, such as the other German-speaking states of Switzerland and Austria, but also, for example, in Japan and the Baltic states (51–54). The population treated in psychosomatic care is slightly different to Medical Psychiatry Units e.g., in the United States. The most prevalent diseases which are treated in psychosomatic wards in Germany are affective and anxiety disorders as well as somatoform disorders, eating disorders and trauma- and stress-related disorders in a specialized group setting with a comprehensive treatment plan (35, 50). Meta-analyses showed moderate to strong treatment effects of inpatient psychosomatic treatment in terms of symptom severity, well-being, and overall functioning (55, 56). However, complex and chronic somatically ill patients often do not fit to these standard psychosomatic wards due to the severity of their physical comorbidities and their need of continuous and specialized somatic co-care.
In line with the presented developments in integrated care, models have been established to realize an inpatient biopsychosocial based approach which exceeds the general treatment options of typical specialized psychosomatic inpatient units (Figure 1, bottom right). These units do not provide adequate internal medicine care competence and equipment appropriate to complex medically ill patients. In Nuremberg General Hospital, like in many others around Germany, a psychosomatic C-L service is integrated throughout the hospital and enables comprehensive psychosomatic co-care of complex and chronically diseased patients by specialized staff assigned to the departments (35, 57) (Figure 1, bottom left). For patients with higher biopsychosocial treatment needs, this therapy model is not always sufficient. Building on this, a specialized inpatient Psychiatric Medicine Unit for biopsychosocial care of the comorbid somatic and mentally ill patients has been successfully established (57) (Figure 1, top left). In this unit, patients are treated who require regular somatic co-care but who are resilient enough to fit effectively into a psychotherapeutic treatment program lasting 6 to 8 weeks consisting of group-based interventions.
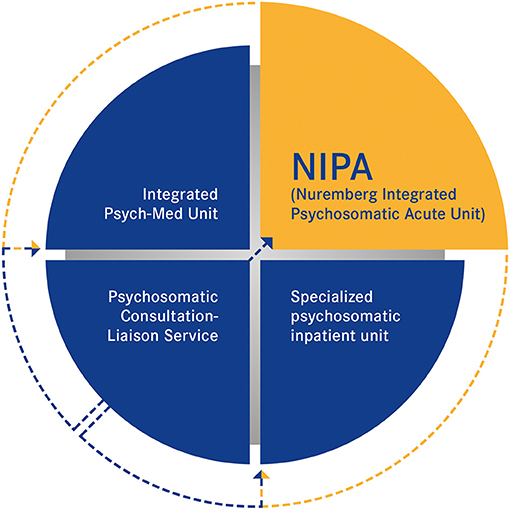
Figure 1. Illustration of the treatment gap in the biopsychosocial care of psychosomatic patients in Germany. NIPA represents an important component for rounding off the infrastructure in healthcare for the complex medically ill. Referral is made by the CL service from the internal medicine wards of general hospital. NIPA, in turn, can be a “door opener” to further psychosomatic treatment programs if needed.
Finally, there remains a gap in the care of chronically ill and often complex patients who need psychotherapeutic treatment, because they are often too impaired to participate in this kind of intensive treatment plan, especially in a group setting. For these patients, all kinds of established psychosomatic inpatient, but also outpatient care is often inaccessible, in particular due to limited mobility. Furthermore, these patients often have no idea how to benefit from biopsychosocial support because of lack of psychotherapeutic experience, which often results in reduced motivation for therapy. Additionally, the experience of psychotherapists in working with physically ill patients is generally low.
Another major challenge in accessing these patients are the long waiting times for psychosomatic treatment, often lasting several weeks to months. For complexly ill, mentally and somatically impaired patients, however, longer waiting times often mean a prolongation of hospitalization in somatic wards, which worsens the course of the disease, as explained above. A more rapid treatment perspective is therefore urgently needed. The Nuremberg Integrated Psychosomatic Acute Unit (NIPA) is trying to improve treatment options regarding all these points and therefore, closes the gap in biopsychosocial care in Germany (Figure 1, top right).
As for evaluation, we would like to explore whether NIPA treatment is resulting in a reduction of symptom burden and is well accepted by the patient group. Thus we hypothesize that anxiety and depressiveness and stress can be significantly reduced and satisfaction with the treatment is high.
Materials and Methods
Clinical Setting
Since 2018, NIPA has been established in inpatient wards of the departments for respiratory medicine, oncology and gastroenterology. One to two patients per ward are regularly included in the NIPA treatment while remaining in the same inpatient bed after somatic stabilization. This approach enables the acute admission of patients to psychosocial mental health care and increases the patient's compliance and motivation since the treatment setting continues to include specialized somatic treatment. For example, hospitalized COPD patients with frequent recurrent inpatient treatments (19) benefit more from this approach.
The initiative for psychosocial co-treatment is taken by the internal medicinal referral to a psychosomatic consultation—liaison service for assessment, partially in the course of a proactive consultation model to improve case detection (41). In case of relevant psychosomatic comorbidity, a psychosomatic-psychotherapeutic treatment in NIPA is planned. After improvement of somatic complaints, psychosomatic conditions are the leading cause for hospitalization and patients are included in NIPA treatment.
An individual treatment plan is drawn up in line with therapy goals, which are achieved by low-threshold, psychoeducational and practice-based interventions. The aim of this biopsychosocial approach is 1. to provide acute and low-threshold psychosocial support and 2. to serve as a “door-opener” for further specialized psychosocial mental health treatment in the outpatient or day-care sector. This is realized by extending the patients' disease model by focusing on psychosomatic and psychosocial understanding of disease processes, supporting stabilization and resource activation. The important psychoeducational content is based especially on clarifying psychosomatic relationships between anxiety, tension and stress with bodily signals such as dyspnea and pain, as well as showing the effectiveness of relaxation on the organism, combined with experiential exercises (e.g., relaxation and imagination techniques). In NIPA, resource activation is primarily focused on those areas of life that are important to the patients and addresses how participation can still be achieved despite limitations—perhaps with the help of additional resources or with a slightly different intensity than before. Another important component is the optimization of drug therapy, e.g. with regard to improving sleep or energy. Physical therapy units aim at enhancing mobilization and movement. The NIPA treatment modules are designed to motivate chronically ill patients without overwhelming them. The multi-professional psychosocial team consists of medical, psychological, art therapeutic, body therapeutic, physiotherapeutic and nursing professional staff. Another important treatment module is the co-management by social services, that focuses on improvement of domestic care as well as on helping with the integration to diverse community offers (e.g., outpatient social psychiatry services) (Table 1).
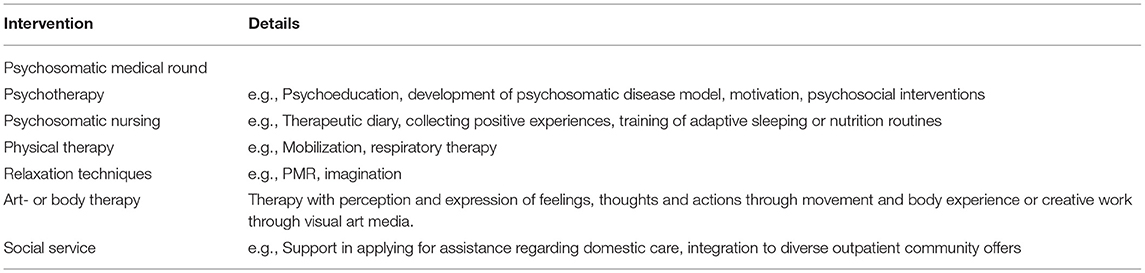
Table 1. NIPA treatment modules.
The psychosomatic therapy program is continuously accompanied by daily medical and nursing care of the somatic ward. By virtue of close, interdisciplinary exchange, a quick response to any changes in the general somatic condition can be guaranteed through specialized somatic care.
Psychometric Instruments
In a naturalistic study design, we assessed the severity of morbidity using diagnosis data during treatment. The severity of mental health problems at admission and at discharge was measured using the Patient Health Questionnaire [PHQ (58, 59)] and Generalized Anxiety Disorder Scale-7 [GAD-7 (60)]. Furthermore, a general assessment of treatment, the relevance to patient needs and satisfaction with treatment were evaluated using the Patient Satisfaction Questionnaire [ZUF-8 (61)].
Statistical Analyses
A Wilcoxon signed-rank test was calculated to compare the severity of symptoms at admission and discharge. Data are presented in mean (M) and standard deviation (SD) with p < 0.05 considered statistically significant. Statistical power (d) was additionally calculated. In a second step, we calculated the effective symptom changes of the individual patients by a description of frequencies in the sample. Both PHQ (PHQ9/PHQ15) as well as GAD-7 enabled this by categorization of symptom severity (severe, moderate, mild, normal symptom manifestation). We described patients with improvement over two categories as having major improvement, and patients with improvement over one category as having moderate improvement. Satisfaction of treatment (ZUF-8) was analyzed by a description of frequencies in the sample.
Results
Until May 2021 we treated 41 patients in NIPA for an average of 15.7 days (SD = 5.3, min = 2, max = 29). The mean age of the patients was 59.9 years (18-87 years). Thirty-one patients were female (76%) and 10 male (24%). The sample showed a high rate of various mental and somatic diagnoses (Table 2). Besides the main psychosomatic diagnosis, the median of mental comorbidities was 1 (min = 0; max = 4), the median of somatic comorbidities was 9 (min = 2, max = 25). We included 38 patients in the analysis of the treatment outcome (admission vs. discharge) due to missing data regarding the symptom evaluation at discharge from three patients (two because of premature dropout from treatment, one because of necessary transfer to intensive care unit due to somatic symptom worsening).
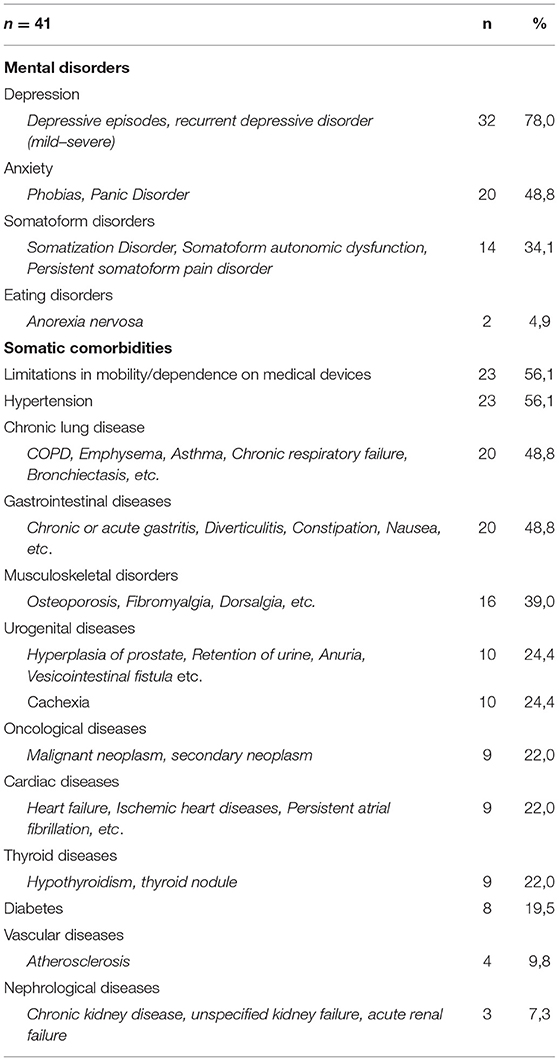
Table 2. Diagnoses in NIPA treatment.
Treatment (n = 38) resulted in a significant reduction of depressive mood (admission: M = 10.9, SD = 6.1, discharge: M = 7.6, SD = 5.3, d = 0.58, p = 0.001, PHQ9), anxiety (admission: M = 10.6, SD = 4.9, discharge: M = 7.3, SD = 4.1, d = 0.65, p< 0.001, GAD-7) and stress (admission: M = 6.0, SD = 3.6, discharge: M = 4.1, SD = 2.5, d = 0.70, p< 0.001, PHQ). Changes in somatic symptom burden were not significant (admission: M = 10.9, SD = 5.8, discharge: M = 9.6, SD = 5.5, d = 0.30, p = 0.073, PHQ15) (Figure 2).
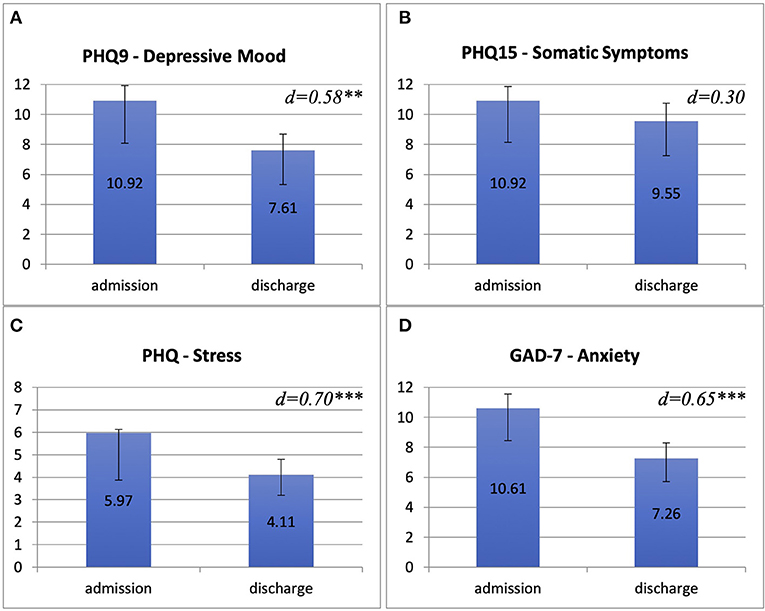
Figure 2. NIPA treatment outcomes compared between admission and discharge on the four symptom scales assessed. We compared means (Y-axis) of Patient Health Questionnaire for depressive mood [PHQ9, (A)], Patient Health Questionnaire for somatic symptoms [PHQ15, (B)], PHQ-stress-scale (C) and Generalized Anxiety Disorder Scale-7 [GAD-7, (D)].
In terms of categorial symptom changes regarding the whole sample, in depressive symptoms (PHQ9) seven patients (18.4%) showed major and 11 (28.9%) showed moderate improvement whereas three patients (7.9%) showed minor worsening and one patient (2.6%) showed major worsening. Sixteen patients (42.1%) reported no categorial changes in depressive symptoms. Eight patients (21.1%) showed major and 14 patients (36.8%) showed moderate improvement in anxiety symptom burden (GAD-7), whereas two patients (5.3%) reported minor worsening, one patient (2.6%) reported major worsening and 13 patients (34.2%) were unchanged. In somatic symptoms (PHQ15) we found moderate improvement in 16 patients (42%), minor worsening in six patients (15.8%), major worsening in two patients (5.3%) and no categorial change in 14 patients (36.8%). In total, four patients (10.5 %) reported no improvement in any of the outcome measures. Out of these, two showed a symptom increase on all scales.
Eighty-nine percent of patients reported large or full satisfaction with treatment (ZUF-8) (somewhat or very helpful in dealing with their problems; therapy meeting most or almost all of their needs, respectively). No patient rated the therapy unsatisfactory, although 11% of patients reported partial dissatisfaction across all diagnosis groups. Key items regarding this dissatisfaction were 1. because they expected greater extent of support regarding their somatic issues and 2. wished for more assistance in dealing with their resulting problems appropriately (Figure 3).
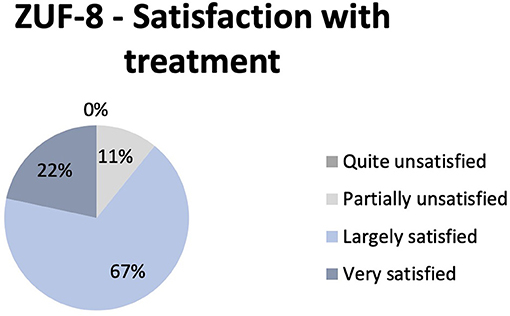
Figure 3. Reported satisfaction with NIPA treatment as measured by Patient Satisfaction Questionnaire (ZUF-8). Diagram shows the frequency of the different levels of satisfaction.
Discussion
Our clinical experience with the NIPA concept to date shows advantages for both patients and treatment providers. Firstly, it offers biopsychosocial stressed, underserved patient groups the chance of specialized and individualized psychosomatic-psychotherapeutic treatment. Secondly, it expands the intervention repertoire of psychosomatic clinics in the urgently needed expansion of treatment capacities for somatically ill patients. In terms of categorization according to Kathol et al. (37), the NIPA concept can be classified a type III Psychiatric Medicine Unit, as it is a highly specialized integrated treatment context, but does not treat medical patients with high acuity. Thus, it can be well-described by the more modern term Complexity Intervention Unit, which is characterized, in particular, by administration through an alliance of general and psychosomatic care, location in general hospital with physical and mental health safety features and capabilities to treat patients with high health complexity (41). Most of these Complexity Intervention Units worldwide focus on integrated treatment of severe mental illnesses e.g., to provide acute medical care for people with serious psychotic symptoms. NIPA, by comparison, follows rather the psychosomatic treatment approach, which has its unique developmental roots in Germany and focusses of biopsychosocial support for a wide range of patients, including affective and anxiety disorders, trauma-related syndromes as well as bodily distress in complex medically ill patients. Similarly to patients with severe mental illnesses, this broader group of patients could gain a substantial enhancement of physical health outcomes due to biopsychosocial care e.g. in terms of education and motivation to more adequate health behavior or improvement of their activity level (62).
The treatment structure comes closest to the model of integrated medical/psychiatric care at the Royal Prince Alfred Hospital in Sydney presented by Gertler et al. especially with regard to the small size of the unit (4–5 beds) and indication defined by: “(1) the patient's medical/surgical problem no longer required acute care on the general ward and residual symptoms or continuing physical care would not interfere with the patient's participation in the ward therapeutic program; (2) the patient was sufficiently mobile to attend to his/her personal hygiene; (3) the patient was transferred to the [Medical Psychiatry Unit] on a voluntary basis; (4) the patient was not suffering from drug or alcohol withdrawal, but could have a history of such abuse; […] (6) internists and surgeons who had previously cared for the patient on the general wards would continue to supervise the relevant aspects of the patient's management and be available in an emergency either to consult, or if necessary, accept transfer back to their care.” [(46), p. 27].
Differences exist in the NIPA-team's stronger multidisciplinary approach to specialized professions such as psychologists, art therapists, and social workers in combination with specialized nursing staff. Furthermore, the unique approach of a decentralized structure enables flexibility. Integrated beds across multiple somatic wards ensure specialized biopsychosocial therapy within the somatic clinical setting best suited to patients' physical symptoms. As requested by Caarls et al., this further lowers the barriers to mental treatment and allows for even greater integration and faster availability of care (39). Increased awareness of mental health comorbidities among the internal medical staff is stimulated by proactive case detection, which is ensured by the psychosomatic C-L structures (35). The multimodal treatment of this complex medically ill patient group also brings benefits to the medical and nursing staff in general hospital since their need of support is well-described in the literature [e.g. (32)].
In Germany, there were already models that provided for the psychosomatic care of “interspersed beds” [“Steglitzer Belegbetten-Modell” (63)] or implemented the psychosomatic treatment unit [“Marburg Model” (64)] on somatic wards. The outlined potentials were observed, but also difficulties in maintaining these structures due to a lack of specialized psychosomatic indication options since these models were the stand-alone treatment possibilities back then. The realization of the NIPA concept is only achievable if it is established in addition to a wide range of treatment options offered by highly qualified psychosomatic care, thus closing the gap that has existed to date in the treatment of complexly and chronically ill patients.
Nevertheless, the need for precise definition of admission criteria for integrated units is frequently stated in the literature (39, 48). The occasionally vague nature of these criteria is a risk for confounding communication and connectivity between patients, caregivers, referrers, and payers that we could also observe in the NIPA treatment context. To improve this situation, Caarls et al. formulated five clusters of criteria for the decision making regarding admission to integrated care units, involving patient and organizational variables as well as psychiatric and medical symptoms and treatment capabilities, which can be assessed by a short questionnaire (39). Another promising, systematic approach, the INTERMED method, identifies complex patients and filters out their treatment priorities quickly and economically using a structured interview (65). An improvement of the NIPA concept in this regard is useful and intended. The major economic challenges faced by many Medical Psychiatry Unit approaches (35) are alleviated in the NIPA treatment by, among other things, lower additional costs as the model leverages existing infrastructure.
The results of the treatment show that it was effective in reducing symptoms of depression, anxiety and stress in patients with complex and chronic somatic comorbidity, which support the assumption that NIPA can close a gap in the care of these complex medically ill patients. A considerable proportion of the treatment group showed measurable categorial improvements in symptom burden. The minor changes in somatic symptoms correspond in part to the clinical impression, since the treated group is composed of multiple and often chronically ill patients with often severe somatic comorbidities, thus a significant improvement would not be expected. Furthermore, PHQ 15 measures the distress caused by the occurrence of a wide range of somatic symptoms over a reference period of four weeks. Considering that NIPA treatment has a median duration of about two weeks, the PHQ-15 does not seem to be an appropriate measure to gain meaningful data in terms of assessing change. For this purpose, future evaluations of treatment should involve measurements of health-related quality of life within a shorter reference time period. Due to the naturalistic design, this evaluation study has limitations, especially with regard to the currently still small sample size and a missing control group.
Regarding a more comprehensive evaluation of treatment success, long-term follow-up data are needed to be collected and supplemented by data regarding the quality of life and the frequency of further medical treatment plus a comparison with an appropriate control cohort, which could be obtained, for example, by propensity score matching in the framework of a quasi-experimental design, as presented by Baumgardt et al. (66). Existing evidence indicates the possibility of reducing healthcare utilization and associated socioeconomical costs due to sufficient treatment, e.g. in patients with somatoform disorders (67). Corresponding observations would be of great assistance to many integrated biopsychosocial treatment units such as NIPA. A transfer of this therapy program into other medical disciplines (e.g., surgery) seems to be reasonable. Clinical impressions indicate that the treatment could be helpful for patients of all genders. The greater number of female patients reported for psychosomatic treatments in general was also evident in NIPA treatment. However, due to the small sample, no valid statements can be made on gender aspects.
Naylor et al. state: “From an integrated care perspective, some of the most significant opportunities for innovation lie in building community-facing liaison services that stretch beyond hospital boundaries and work in new ways with community partners” [(36), p. 54]. Especially with regard to many patients' huge dependence on social care or support from the social sector, the strengthening and improvement of collaboration between inpatient and outpatient facilities as well as between the different mental, physical and social caregivers is necessary (48). The NIPA concept, with its focus on low-threshold interventions and the “door-opener” function for further treatment options, e.g., more intensive biopsychosocial treatment in specialized psychosomatic inpatient units or outpatient psychotherapeutic and social psychiatric care, takes important steps in this direction, although these need to be further intensified and extended.
The here presented treatment model requires careful and interdisciplinary coordination, especially with regard to a rapid response to somatic deterioration in the frequent case of multimorbidity. If this challenge is met with effective procedures, one of the great strengths of the concept will have been realized, because this kind of individualized treatment would not be possible in any other context.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
PK, EK-K, BS, and CW contributed to the conception and design of NIPA. JF, AD, and MW supported the concept and contributed to the realization in their departments. PK performed the statistical analyses and wrote the first draft of the manuscript. CW wrote sections of the manuscript. All authors contributed to manuscript revision, read, and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
The authors would like to thank Michaela Meth for creating and authorizing the figure showing the contribution of NIPA regarding the treatment gap in biopsychosocial care (Figure 1).
References
1. Beutel ME, Bleichner F. Inpatient psychosomatic treatment of anxiety disorders: Comorbidities, predictors, and outcomes. Int J Clin Health Psychol. (2011) 11:443–57.
2. De Hert M, Correll CU, Bobes J, Cetkovich-Bakmas M, Cohen D, Asai I, et al. Physical illness in patients with severe mental disorders. I Prevalence, impact of medications and disparities in health care. World Psychiatry. (2011) 10:52–77. doi: 10.1002/j.2051-5545.2011.tb00014.x
3. Yohannes AM, Willgoss TG, Baldwin RC, Connolly MJ. Depression and anxiety in chronic heart failure and chronic obstructive pulmonary disease: prevalence, relevance, clinical implications and management principles. Int J Geriatr Psychiatry. (2010) 25:1209–21. doi: 10.1002/gps.2463
4. Yohannes AM, Baldwin RC, Connolly MJ. Mood disorders in elderly patients with chronic obstructive pulmonary disease. Rev Clin Gerontol. (2000) 10:193–202. doi: 10.1017/S0959259800002100
5. Rutledge T, Reis VA, Linke SE, Greenberg BH., Mills PJ. Depression in heart failure. (2006) 48:11. doi: 10.1016/j.jacc.2006.06.055
6. Thombs BD, Bass EB, Ford DE, Stewart KJ, Tsilidis KK, Patel U, et al. Prevalence of depression in survivors of acute myocardial infarction: Review of the evidence. J Gen Intern Med. (2006) 21:30–8. doi: 10.1111/j.1525-1497.2005.00269.x
7. Rumsfeld JS, Magid DJ, Plomondon ME, Sales AE, Grunwald GK, Every NR, et al. History of depression, angina, and quality of life after acute coronary syndromes. Am Heart J. (2003) 145:493–9. doi: 10.1067/mhj.2003.177
8. Pacella ML, Hruska B, Delahanty DL. The physical health consequences of PTSD and PTSD symptoms: a meta-analytic review. J Anxiety Disord. (2013) 27:33–46. doi: 10.1016/j.janxdis.2012.08.004
9. Härter M, Baumeister H, Reuter K, Jacobi F, Höfler M, Bengel J, et al. Increased 12-month prevalence rates of mental disorders in patients with chronic somatic diseases. Psychother Psychosom. (2007) 76:354–60. doi: 10.1159/000107563
10. Riedlinger C, Schmidt G, Weiland A, Stengel A, Giel KE, Zipfel S, et al. Which symptoms, complaints and complications of the gastrointestinal tract occur in patients with eating disorders? A systematic review and quantitative analysis. Front Psychiatry. (2020) 11:195. doi: 10.3389/fpsyt.2020.00195
11. Kop WJ, Toussaint A, Mols F, Löwe B. Somatic symptom disorder in the general population: Associations with medical status and health care utilization using the SSD-12. Gen Hosp Psychiatry. (2019) 56:36–41. doi: 10.1016/j.genhosppsych.2018.10.004
12. Henningsen P. Management of somatic symptom disorder. Dialogues Clin Neurosci. (2018) 20:9. doi: 10.31887/DCNS.2018.20.1/phenningsen
13. Burton C, Fink P, Henningsen P, Löwe B, Rief W. Functional somatic disorders: discussion paper for a new common classification for research and clinical use. BMC Med. (2020) 18:34. doi: 10.1186/s12916-020-1505-4
14. Häuser W, Hausteiner-Wiehle C, Henningsen P, Brähler E, Schmalbach B, Wolfe F. Prevalence and overlap of somatic symptom disorder, bodily distress syndrome and fibromyalgia syndrome in the German general population: a cross sectional study. J Psychosom Res. (2020) 133:110111. doi: 10.1016/j.jpsychores.2020.110111
15. Felker B, Yazel JJ, Short D. Mortality and medical comorbidity among psychiatric patients: a review. Psychiatr Serv. (1996) 47:1356–63. doi: 10.1176/ps.47.12.1356
16. Kathol RG. Medical psychiatry units: the wave of the future. Gen Hosp Psychiatry. (1994) 16:1–3. doi: 10.1016/0163-8343(94)90080-9
17. Druss BG, Rosenheck RA, Sledge WH. Health and disability costs of depressive illness in a major U. S. corporation. Am J Psychiatry. (2000) 157:1274–8. doi: 10.1176/appi.ajp.157.8.1274
18. Bressi SK, Marcus SC, Solomon PL. The impact of psychiatric comorbidity on general hospital length of stay. Psychiatr Q. (2006) 77:203–9. doi: 10.1007/s11126-006-9007-x
19. Pooler A, Beech R. Examining the relationship between anxiety and depression and exacerbations of COPD which result in hospital admission: a systematic review. Int J Chron Obstruct Pulmon Dis. (2014) 9:315. doi: 10.2147/COPD.S53255
20. Jennings JH, DiGiovine B, Obeid D, Frank C. The association between depressive symptoms and acute exacerbations of COPD. Lung. (2009) 187:128–35. doi: 10.1007/s00408-009-9135-9
21. Long H, Howells K, Peters S, Blakemore A. Does health coaching improve health-related quality of life and reduce hospital admissions in people with chronic obstructive pulmonary disease? A systematic review and meta-analysis. Br J Health Psychol. (2019) 24:515–46. doi: 10.1111/bjhp.12366
22. Bradley SM, Rumsfeld JS. Depression and cardiovascular disease. Trends Cardiovasc Med. (2015) 25:614–22. doi: 10.1016/j.tcm.2015.02.002
23. Carney RM, Freedland KE. Depression and coronary heart disease. Nat Rev Cardiol. (2017) 14:145–55. doi: 10.1038/nrcardio.2016.181
24. Albus C, Waller C, Fritzsche K, Gunold H, Haass M, Hamann B, et al. Bedeutung von psychosozialen Faktoren in der Kardiologie – Update 2018: positionspapier der Deutschen Gesellschaft für Kardiologie. Kardiologe. (2018) 12:312–31. doi: 10.1007/s12181-018-0271-4
25. Barsky AJ, Orav EJ, Bates DW. Somatization increases medical utilization and costs independent of psychiatric and medical comorbidity. Arch Gen Psychiatry. (2005) 62:903. doi: 10.1001/archpsyc.62.8.903
26. von Leupoldt A, Kenn K. The psychology of chronic obstructive pulmonary disease: Curr Opin Psychiatry. (2013) 26:458–63. doi: 10.1097/YCO.0b013e328363c1fc
27. Seelig MD, Katon W. Gaps in depression care: why primary care physicians should hone their depression screening, diagnosis, and management skills. J Occup Environ Med. (2008) 50:451–8. doi: 10.1097/JOM.0b013e318169cce4
28. Goldman LS, Nielsen NH, Champion HC. Awareness, diagnosis, and treatment of depression. J Gen Intern Med. (1999) 14:569–80. doi: 10.1046/j.1525-1497.1999.03478.x
29. Sporinova B, Manns B, Tonelli M, Hemmelgarn B, MacMaster F, Mitchell N, et al. Association of mental health disorders with health care utilization and costs among adults with chronic disease. JAMA Netw Open. (2019) 2:e199910. doi: 10.1001/jamanetworkopen.2019.9910
30. Dalal AA, Shah M, Lunacsek O, Hanania NA. Clinical and economic burden of depression/anxiety in chronic obstructive pulmonary disease patients within a managed care population. COPD J Chronic Obstr Pulm Dis. (2011) 8:293–9. doi: 10.3109/15412555.2011.586659
31. Alberque C, Gex-Fabry M, Whitaker-Clinch B, Eytan A. The five-year evolution of a mixed psychiatric and somatic care unit: a European experience. Psychosomatics. (2009) 50:354–61. doi: 10.1176/appi.psy.50.4.354
32. Rettke H, Petry H, von Känel R, Jordan K-D, Ernst J. Patientinnen und Patienten mit psychiatrischen Komorbiditäten im Akutspital: Ein Spannungsfeld mit interprofessionellem Handlungsbedarf. Pflege. (2020) 33:85–91. doi: 10.1024/1012-5302/a000718
33. Huyse FJ, Stiefel FC. Controversies in consultation–liaison psychiatry. J Psychosom Res. (2007) 62:257–8. doi: 10.1016/j.jpsychores.2006.07.025
34. Babajide A, Ortin A, Wei C, Mufson L, Duarte CS. Transition cliffs for young adults with anxiety and depression: is integrated mental health care a solution? J Behav Health Serv Res. (2020) 47:275–92. doi: 10.1007/s11414-019-09670-8
35. Wulsin LR, Söllner W, Pincus HA. Models of integrated care. Med Clin North Am. (2006) 90:647–77. doi: 10.1016/j.mcna.2006.05.005
36. Naylor C, Das P, Ross S, Honeyman M, Thompson J, Gilburt H. Bringing Together Physical and Mental Health. London: Kings Fund (2016).
37. Kathol RG, Harsch HH, Hall RCW, Shakespeare A, Cowart T. Categorization of types of medical/psychiatry units based on level of acuity. Psychosomatics. (1992) 33:376–86. doi: 10.1016/S0033-3182(92)71942-2
38. Kishi Y, Kathol RG. Integrating medical and psychiatric treatment in an inpatient medical setting: the type IV program. Psychosomatics. (1999) 40:345–55. doi: 10.1016/S0033-3182(99)71230-2
39. Caarls PJ, van Schijndel MA, Berk G., van den, Boenink AD, Boerman D, Lijmer JG, et al. Factors influencing the admission decision for Medical Psychiatry Units: A concept mapping approach. PLoS ONE. (2019) 14:e0221807. doi: 10.1371/journal.pone.0221807
40. Van Schijndel MA, Jansen LAW, van de Klundert JJ. Empirical types of medical psychiatry units. Psychother Psychosom. (2019) 88:127–8. doi: 10.1159/000493689
41. Kathol RG, Kunkel EJS, Weiner JS, Mccarron RM, Worley LLM, Yates WR, et al. Psychiatrists for medically complex patients: bringing value at the physical health and mental health/substance-use disorder interface. Psychosomatics. (2009) 50:93–107. doi: 10.1176/appi.psy.50.2.93
42. Eytan A, Bovet L, Gex-Fabry M, Alberque C, Ferrero F. Patients' satisfaction with hospitalization in a mixed psychiatric and somatic care unit. Eur Psychiatry. (2004) 19:499–501. doi: 10.1016/j.eurpsy.2004.09.004
43. Wullschleger A, Khazaal Y, Heinze M. Editorial: new models of care for patients with severe mental illness—bridging in- and outpatients. Front Psychiatry. (2018) 9:3. doi: 10.3389/fpsyt.2018.00003
44. Buckley P, Freyne A, Walshe N. The medical-psychiatry unit. Psychosomatics. (1994) 35:515–9. doi: 10.1016/S0033-3182(94)71719-9
45. Leue C, Driessen G, Strik JJ, Drukker M, Stockbrügger RW, Kuijpers PM, et al. Managing complex patients on a medical psychiatric unit: An observational study of university hospital costs associated with medical service use, length of stay, and psychiatric intervention. J Psychosom Res. (2010) 68:295–302. doi: 10.1016/j.jpsychores.2009.04.010
46. Gertler R, Kopec-Schrader EM, Blackwell CJ. Evolution and evaluation of a Medical Psychiatric Unit. Gen Hosp Psychiatry. (1995) 17:26–31. doi: 10.1016/0163-8343(94)00063-J
47. Nomura S, Shigemura J, Nakamura M, Hosaka T, Berger D, Takahashi Y. Evaluation of the first Medical Psychiatry Unit in Japan. Psychiatry Clin Neurosci. (1996) 50:305–8. doi: 10.1111/j.1440-1819.1996.tb00569.x
48. Davidsen AS, Davidsen J, Jønsson ABR, Nielsen MH, Kjellberg PK, Reventlow S. Experiences of barriers to trans-sectoral treatment of patients with severe mental illness. A qualitative study Int J Ment Health Syst. (2020) 14:87. doi: 10.1186/s13033-020-00419-x
49. Deter H-C, Kruse J, Zipfel S. History, aims and present structure of psychosomatic medicine in Germany. Biopsychosoc Med. (2018) 12:1. doi: 10.1186/s13030-017-0120-x
50. Albani C, Becker-Pfaff J, Gramich B, Hildenbrand G, Kneer-Weidenhammer S, Rothe H-M. Krankenhausbehandlung im Gebiet Psychosomatische Medizin und Psychotherapie Grundlagen. DGPM Fortbildungsakademie (2020).
51. Ancãne G, Utinãns A, Ancãns A, Miksons A. Psychosomatic medicine in the Baltic States, Soviet Union, and the Russian Federation. In: Leigh H, editor. Global Psychosomatic Medicine and Consultation-Liaison Psychiatry: Theory, Research, Education, and Practice. Cham: Springer (2019). p. 365–81. doi: 10.1007/978-3-030-12584-4_16
52. Murakami M, Nakai Y. Current state and future prospects for psychosomatic medicine in Japan. Biopsychosoc Med. (2017) 11:1. doi: 10.1186/s13030-017-0088-6
53. Buddeberg C. Psychosocial and psychosomatic medicine as well as psychotherapy in Switzerland – developments over the past fifty years. Z Psychosom Med Psychother. (2004) 50:346–54. doi: 10.13109/zptm.2004.50.4.346
54. Pieringer W, Schüssler G. Psychosomatic medicine and psychotherapy in Austria. Z Psychosom Med Psychother. (2004) 50:241–52. doi: 10.13109/zptm.2004.50.3.241
55. Liebherz S, Rabung S. Do patients' symptoms and interpersonal problems improve in psychotherapeutic hospital treatment in Germany? - a systematic review and meta-analysis. PLoS ONE. (2014) 9:e105329. doi: 10.1371/journal.pone.0105329
56. Liebherz S, Rabung S. Wirksamkeit psychotherapeutischer Krankenhausbehandlung im deutschsprachigen Raum: Eine Meta-Analyse. Psychother Psychosom Med Psychol. (2013) 63:355–64. doi: 10.1055/s-0033-1337909
57. Stein B, Wentzlaff E, Söllner W. Das Nürnberger Modell der integrierten Psychosomatik: Wächst hier zusammen, was zusammen gehört? Psychol Med. (2018) 3:26–35.
58. Spitzer RL. Validation and utility of a self-report version of PRIME-MDThe PHQ primary care study. JAMA. (1999) 282:1737. doi: 10.1001/jama.282.18.1737
59. Kocalevent R-D, Hinz A, Brähler E. Standardization of a screening instrument (PHQ-15) for somatization syndromes in the general population. BMC Psychiatry. (2013) 13:91. doi: 10.1186/1471-244X-13-91
60. Spitzer RL, Kroenke K, Williams JBW, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. (2006) 166:1092. doi: 10.1001/archinte.166.10.1092
61. Schmidt J, Lamprecht F, Wittmann WW. Zufriedenheit mit der stationären Versorgung. Entwicklung eines Fragebogens und erste Validitätsuntersuchungen. Psychother Psychosom Med Psychol. (1989) 39:248–55.
62. De Hert M, Cohen D, Bobes J, Cetkovich-Bakmas M, Leucht S, Ndetei DM, et al. Physical illness in patients with severe mental disorders. II Barriers to care, monitoring and treatment guidelines, plus recommendations at the system and individual level. World Psychiatry. (2011) 10:138–51. doi: 10.1002/j.2051-5545.2011.tb00036.x
63. Deter H-C, Weber C, Adolph D, Stehle S, Blum B, Martienssen R, et al. Von der angewandten Psychosomatik zur integrierten Medizin - Erfahrungen mit dem Steglitzer Belegbettenmodell. Psychother Psychosom Med Psychol. (2004) 54:161–4. doi: 10.1055/s-2003-814789
64. Schüffel W. Die andere Krankenhausbehandlung - Warum 1 mal 36 nicht gleich 6 mal 6 ist. Münch Med Wochenschr MMW Organ Für Amtliche Prakt Ärzte. (1998) 140:36–41.
65. Latour CHM, Huyse FJ, de Vos R, Stalman WAB. A method to provide integrated care for complex medically ill patients: the INTERMED. Nurs Health Sci. (2007) 9:150–7. doi: 10.1111/j.1442-2018.2007.00292.x
66. Baumgardt J, Schwarz J, von Peter S, Holzke M, Längle G, Brieger P, et al. Aufsuchende Krisenbehandlung mit teambasierter und integrierter Versorgung (AKtiV): Eine naturalistische multizentrische kontrollierte Studie zur Evaluierung stationsäquivalenter psychiatrischer Behandlung in Deutschland. Nervenheilkunde. (2020) 39:739–45. doi: 10.1055/a-1213-8999
Keywords: integrated care, biopsychosocial approach, psychosomatics, internal medicine, chronic disease, Psychiatric Medicine Units, psychotherapy
Citation: Köbler P, Krauss-Köstler EK, Stein B, Ficker JH, Wilhelm M, Dechêne A and Waller C (2022) Specialized Biopsychosocial Care in Inpatient Somatic Medicine Units—A Pilot Study. Front. Public Health 10:844874. doi: 10.3389/fpubh.2022.844874
Received: 28 December 2021; Accepted: 21 March 2022;
Published: 12 April 2022.
Edited by:
Christos Theleritis, National and Kapodistrian University of Athens, GreeceReviewed by:
Atsuko Koyama, Kindai University, JapanHans-Christian Deter, Charité Universitätsmedizin Berlin, Germany
Copyright © 2022 Köbler, Krauss-Köstler, Stein, Ficker, Wilhelm, Dechêne and Waller. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Paul Köbler, paul.koebler@klinikum-nuernberg.de