 Haibo Lin
Haibo Lin Haijun Ren
Haijun Ren- 1Business School, Dalian University of Foreign Languages, Dalian, China
- 2Department of General Surgery, Dalian Municipal Friendship Hospital, Dalian, China
The impact of social participation (SP) on the health of the elderly has been widely recognized, and urban-rural differences in social participation have attracted attention. However, few studies discussed the impact of social participation on specific health indicators and the further subdivision of urban-rural differences. This research aims to use the dimensions of interpersonal behaviors and population density rather than simple urban-rural distinctions to justify community differences and compare these differences' direct and indirect effects on grip strength. This study used 15,871 respondents aged over 50 years from the China Health and Retirement Longitudinal Study (CHARLS). An SEM (Structural Equation Modeling) analysis was used to explore the joint effect of interpersonal behavior and population density on social participation and the consequent impact on changes in grip strength and compare the differences among different genders, ages, wealth levels, and family relationships. The results indicated that community differences characterized by interpersonal behavior and population density have direct effects on grip strength and indirect effects on it through social participation. The conclusion is that the frequency of social activities, such as mah-jong and dancing in the Metropolitan Fringe and county-level cities is higher than that in Metropolitan centers. The high frequency of these activities has a positive and indirect impact on grip strength, and community differences have a more significant impact on women's social participation than men. However, the direct effect of community differences as defined by interpersonal communication and population density on grip strength is greater than the indirect effect of other factors through social participation.
Introduction
Grip strength is an essential indicator of muscle ability (1–6) and weakness (1, 7, 8). Because of its ease of measurement and stability (9), grip strength can be used as an essential comparable biomarker for the standardized evaluation of human body functions (10). Increasingly, grip strength is becoming a major feature of studies on geriatric health. Such as Sayer and Kirkwood (10) said: “An intriguing implication is that grip strength might act as a biomarker of aging across the life course. This is not a new idea, but findings from Prospective Urban Rural Epidemiology PURE add support. Loss of grip strength is unlikely to lie on a single final common pathway for the adverse effects of aging. However, it might be an excellent marker of underlying aging processes?” Grip strength is directly related to cardiovascular disease (11), Alzheimer's disease (7), cognitive impairment (12), and the mortality rate (10, 13). However, the analysis of roles of factors affecting grip strength has not been detailed enough, and the conclusions are not sufficiently clear (14). It is generally believed that the influencing factors of grip strength include age, physical activity (PA), and social activity (SA) (15, 16). Of course, some studies discussed social status, economic conditions, education, and other factors that can affect grip strength through PA and SP (17, 18). However, studies with larger samples, examine the mechanisms of these effects and draw more precise conclusions are needed.
According to the theoretical framework of social ecology, the environment (broadly defined), behavior patterns, and health status interact with each other. Some studies have emphasized the importance of the infrastructural environment (19, 20). This article suggests that the difference between urban and rural areas in China is not only the population density but also the interpersonal habits, Differences in behavior patterns in communities in China are more likely to be the key factors that affect SP, which is considered to be very relevant to the health of elderly people. Accordingly, based on the analysis of the SA of elderly residents of urban and rural areas, this article proposed that the agricultural social customs (behavior patterns) and population density (environment) are important factors that affect the health of elderly people. In other words, community density and behavior affect the health (both physical and psychological) of elderly people through social participation.
In this study, based on a large sample from the China Health and Retirement Longitudinal Study (CHARLS), which was completed by Peking University, this article constructs a conceptual model of community differences, social activities, and change in grip strength through a structural equation model. This article aimed to reveal the joint effect of community differences and lifestyle habits on social participation and the consequent effect on changes in grip strength and to compare the differences among people with different genders, ages, wealth levels, and family relationships. Therefore, (1) This paper built an association model based on communication style and specific biomarkers and used a large sample size to test this relationship. (2) This article expected that a comparison of the intermediate and direct effects could show that non-interventional exogenous variables such as age and gender on grip strength will be partially endogenous (intervenable), rather than just controlling variables. (3) This paper proposed that it is not only the differences between urban and rural areas (in a broad geographical sense) but also the different population densities and cultural backgrounds of residential areas that should be used to classify communities here. In assessing community differences, this article scored types of communities differently than in the original questionnaire. By rearranging the scoring structure for different types of communities, this article revealed the characteristics of different urban communities and rural elderly SA in China and the impact of these differences on grip strength. (4) When discussing the relationship between social activities and grip strength, this article extended the measurable range of social activities. This article also included the occasional care of parents or grandchildren within the scope of active social activities.
Literature Review and Hypothesis
Grip Strength as a Biomarker of the Health of Elderly People
Grip strength is regarded as one of the indicators of the health of elderly people. The health of elderly people is divided into the following two categories (21): overall health (22) and specific signs (biomarkers). Different research strategies can also be divided into different categories, including multiple linear modeling with factor and mechanism analysis involving intermediate variables. Of course, there have been some recent studies based on longitudinal data. Specific analyses of the influencing factors of grip strength and muscle atrophy include (1) the impact of PA on grip strength (23, 24); (2) the impact of SA on grip strength (17, 25); (3) the influence of other individuals' heterogeneity on grip strength, the most important of which is age (26, 27); and (4) the relationship between medical indicators and physiological mechanisms, including PA, nutrient intake (protein), oxidative stress, inflammation, and hormone changes, and more systematic therapeutic interventions (14). High levels of serum interleukin (IL)-6, C-reactive protein (CRP), and α1-antichymotrypsin (ACT) are associated with decreased muscle strength or muscle mass (muscular sarcopenia) (28).
Relationship Between Physical Activity and Grip Strength
The relationship between PA and grip strength was generally investigated in comprehensive studies of a series of health indicators as well as correlation studies (29).
The effect of PA on grip strength is not very clear, and some studies have shown that physical exercise can improve grip strength in middle-aged elderly, and oldest-old groups (23, 30–33). There are fewer studies on the mechanism of this effect. Celis-Morales et al. have argued that grip strength has a moderating effect on the relationship between PA and mortality rate (34). In the oldest-old group, physical exercise has no relationship with improved muscle capacity (24, 30). However, it is generally believed that even if there is a connection between PA and grip strength (33), especially among older women (24), such a relationship would be small or not very significant (35).
Based on the conclusions of some studies with larger samples in the above literature, we propose Hypothesis HA: moderate PA has a positive relationship with grip strength.
Social Activities and Grip Strength
There are two lines of study of the relationship between SA and grip strength. First, social interaction directly affects health (broadly defined). There are definite conclusions about the impact of social interaction on mental and physical health. However, the positive and negative impacts need to be analyzed based on the specific SA (36, 37). For example, optimism and positivity are always good for health, and in general, frequent interpersonal activities can affect physical conditions. SA has been divided into categories, such as general social connections (38, 39) and semiformal social assistance and formal community support (volunteering) (40), and then discussed with the mediating role of community solidarity or community support (22). However, is the relation between social interaction and grip strength positive or negative regarding specific physical functions? In particular, such discussions have rarely been conducted based on examining different age groups within the elderly population. Some studies have emphasized personal income (25) and indicated that social participation could promote PA and stimulate hormone secretion (41). Theoretical support for the impact of social participation on grip strength suggests that social interaction promotes the secretion hormones, including sex hormones, adrenal hormones, and thyroid hormones (14). Therefore, stimulating the secretion of these hormones would alter muscle function.
The second line of study examines the effect of SA on PA and therefore, on physical health. Socializing online and participating in groups promote PA and self-rated health (36, 42–44). Many studies also seem to be too broad and fail to provide evidence of intermediate mechanisms. For example, Yorke et al. (45) reported a significant relationship between delayed retirement (assessed in a treatment group that differed in terms of their social participation from a peer control group that retired at the expected age) and muscle atrophy as assessed by grip strength. Nevertheless, the authors did not analyze the mechanism of delayed retirement.
Since it discusses a specific health index rather than a general concept of health, this study must find evidence that SA affects grip strength through PA. Studies have discussed the impact of SA and PA on cognitive function to a similar extent (46). Suppose PA is related to cognitive function and neural organization because muscle strength is also related to nerve tissue (47). In that case, it can be concluded that PA and grip strength may be related. However, this is still too general.
Because the mechanism of the relationship among SA, PA, and grip strength is not very clear, and because engagement in boring activities causes depression (43) (due to the secretion of hormones that are negative for health) (42), this article proposes hypothesis HB: positive types of SA ameliorate the decline in the grip strength of elderly people.
Factors That Affect Both Social Activities and Grip Strength
Many factors affect the SA of elderly people. Here, we focus on the factors that affect both SA and grip strength to compare their direct effects and the indirect effects through SA on grip strength. This approach will allow for a better decomposition of the effects. The community environment, family relations, economic status, age, and gender are of particular interest.
Community Differences
The community environment includes the physical environment and social environment (interpersonal environment is the primary representation). China is an urban-rural dual social form. It is recognized that there are significant differences between urban and rural elderly communities in China. It is impossible to analyze the urban-rural differences of Chinese elderly life using the analyzing framework of the United States (48–50). However, in addition to these differences, we note that the community environment that has advanced facilities does not necessarily positively impact social participation. Neighborhood relationship culture has attracted attention recently (51). In China, generally, the elderly in the city centers does not have more SA than the elderly communities at the junction of urban and rural areas (urban fringe). SA based on city center communities are more difficult to organize than those at the junction of urban, rural areas and towns. For example, mah-jongg games greatly increase social activities, while big cities are separated from rural areas (rural culture) for a long time Therefore, they are less keen on such activities, like square dance, which has the same characteristics (12, 52). Therefore, the community environment conducive to social communication can be greatly improved by not completely relying on the existing organizational forms and facility construction (53). So we propose hypothesis HC: The combination of population density and neighborhood relations is positively correlated with SP.
Wealth
By analyzing health data for elderly Europeans, Jancova-Vseteckova et al. (17) found that education, professional class, income, and wealth had a predictive effect on male grip strength, while only education and wealth had a predictive effect on female grip strength. However, they provided no further analysis of more complicated impact mechanisms; while they showed that wealth affected grip strength, there was no explanation for the effect. Regarding social status, studies have also reported its relationship with grip strength (18), but it is even harder to find logical analyses of this relationship. Therefore, hypothesis HD is proposed: living standard is positively related to grip strength.
Structural Equation Model
Only a few articles in the literature, such as Celis-Morales et al. (43) provided specific measures of the impact of PA and SA on grip strength. Therefore, this article proposess a structural equation model and performs factor analysis of latent variables to correct possible measurement errors. Moreover, this article classified essential variables, such as SP, PA, and Zone (Differences in residential communities) (Figure 1).
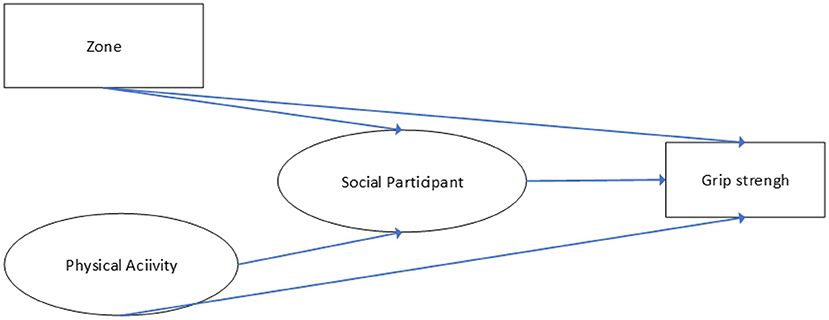
Figure 1. Construction of the conceptual model.
Method
Data
This study's database comes from the fourth wave of follow-up surveys conducted in 2015 for the CHARLS. The CHARLS is a national survey that provides comprehensive and high-quality data on population background, family characteristics, health behaviors, and Chinese citizens' status and retirement information (54). Using probability proportional to size (PPS) sampling and computer-assisted personal interview (CAPI) technology, interviews were conducted with middle-aged and elderly respondents in 450 communities in 150 counties in 28 provinces. The Biomedical Ethics Review Committee of Peking University approved the study (IRB00001052–11015). The baseline survey (the first wave) was conducted in 2011; among the community residents who participated in the baseline survey, 20,543 participated in 2015. To study the factors influencing the grip strength of the elderly population, this article limited the sample of respondents to those over 50 years old. This article included 15871 respondents (7807 male, 8064 female) who participated in the fourth wave of the study. More details can be found from http://charls.pku.edu.cn/Public/ashelf/public/uploads/document/2018-charls-wave4/application/CHARLS_2018_Users_Guide.pdf (55, 56).
Measurement
This study used measurement items for some constructs from the relevant literature. This article chose some items to assess PA, SP, and respondents' relationships with their adult children. Some items also collected demographic information about respondents, such as biomarkers, age, expenditure, and smoking and drinking behavior. All items were measured (converted to ordinal or quasi-ordinal scales) on a 7-point or 6-point scale from low to high due to the comparability of quantity or frequency.
Dependent Variable
Grip Strength
The grip strength index uses the average values for the left and right hands from the second test. The measurement method lets interviewees “Stand, hold the dynamometer at a right angle and squeeze the handle for a few seconds, then Conduct the hand strength measurements (unit: kilogram).” This article did not use the grip strength-to-weight ratio because many studies have indicated that the correlation between grip strength and weight is not very strong. The grip strength-to-weight ratio was entered into the model as an explanatory variable. The result was not much different in terms of the direction of the odds ratios.
Independent Variables
Differences in Residential Communities (Zone)
The population density in China's urban and rural areas gradually decreases from metropolises, provincial administrative centers, suburbs of large cities, general prefecture-level cities, county-level cities, and townships from 4,000, 2,000, 1,000, and 500 peoples/km2, respectively (57). Additionally, some studies have investigated the development of the suburbs of large cities (58, 59). The population density has a decisive effect on interpersonal communication based on the CHARLS data; regarding interpersonal communication methods, in China, the urban-rural fringe is more active and inclusive in relation to activities among the elderly- population than urban areas. Due to the non-enclosed residential areas and semi-urbanized (preserving more rural lifestyle habits) habits, towns (county-level cities) also have similar characteristics as the urban-rural fringe of a big city (the surrounding rural population settles in the city). According to this idea, this article found that the first type of interpersonal communication is entirely related to density (interaction with friends declined in recent years). The second activity (playing mah-jong, chess, or cards) is related to communication habits. Thus, this article made slight adjustments to the ranking order of the first three types of residential areas based on the original questionnaire's order according to the population density and the frequency of participation in mah-jong card games (Mah-jongg is a traditional Chinese game similar to playing cards and it has some gambling properties) and tested the ranking with the Pearson correlation coefficient. In other words, different kinds of regional rankings respect the original questionnaire, which is based on the dimension of population density. However, it is also adjusted according to the frequency of social activities, which aligns with the original intention of defining the community based on population density and social activities.
Residents of large cities come from different backgrounds, but they have a low level of intimacy. Except for these large cities, most of China's cities are predominantly populated by migrants from nearby rural areas or small cities. Therefore, there are no significant differences in residents' backgrounds in these cities. Most of these cities have rural Chinese social characteristics, which means that the community is not composed of sporadic long-distance immigrants; even if there are some long-distance immigrants, they cluster in groups. Because China's most significant cultural differences are not due to migrating from long distances but rather to the urban-rural binary, community residents who moved to the community from a rural area are not culturally diverse from their neighbors (60). In other respects, compared with their urban counterparts, rural residents have a limited number of social networks, but these networks are reliable and stable (52, 61–63).
Physical Activity
The original questionnaire distinguishes high-intensity PA, medium-intensity PA, and low-intensity PA. Since singing and dancing for leisure and entertainment have PA characteristics, singing and dancing are included as low-intensity PA as a supplementary indicator for intense PA.
Mediating Variable: Social Activity
Douglas et al. (22) recommended using the classification standards for broad social participation, semiformal social support, and formal social support. According to his definition, the government provides China's formal social support, but it is just at the beginning stage, So the previous data is insufficient to be used. Therefore, this article divides social activities into general social activities, helping others, and joining social groups instead of using such a classification.
Potential Confounding Variables
Potential confounding variables were considered the relationship with adult children, smoking, upper-body pain, and basic expenditure (Table 1).
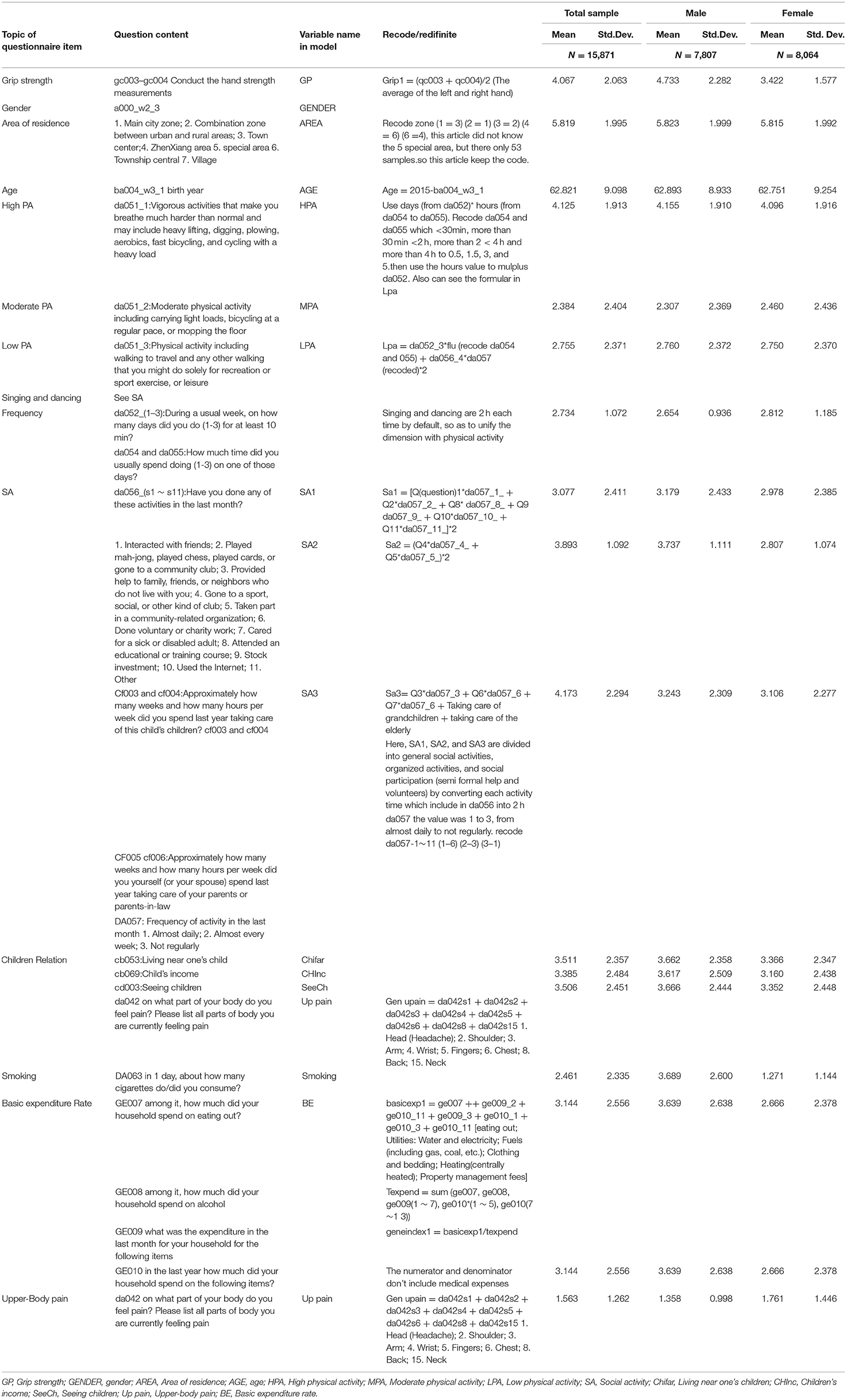
Table 1. Description of the main variables and descriptive statistics of the sample.
Analysis
Descriptive statistical analysis and structural equation modeling (SEM) were used in the study. SEM model is often used in such databases with many ordered variables (64–66). The structural equation model is advantageous for quantitative analysis and group comparison of multivariate interaction effects and can help correct measurement errors. Therefore, this article used a structural equation model to analyze the relationship among PA, community differences, social participation, family relations, and grip strength. All variables had good discrimination and were suitable for SEM. Furthermore, the sample size was larger than 1,000, and samples of this size can generally be considered to follow a normal distribution.
Confirmatory Factor Analysis
CFA was used to measure PA, relationships with adult children, and SP. According to the results, the composite reliability and validity coefficients in all measurement models were high, indicating that all measurement models had excellent reliability and validity and were suitable for SEM analysis.
Regarding the fit indexes of the entire sample model, the root mean square error of approximation (RMSEA) was 0.075, the ratio of chi-square to the degrees of freedom (X2/DF) was 4.902, the comparative fit index (CFI) was 0.912, the Tucker-Lewis index (TLI) was 0.903, and the standardized root mean square residual (SRMR) was 0.059; these fit indexes indicated that the models had a good fit, and they are shown in Table 2.

Table 2. Item reliability, composite reliability, convergent validity, and discriminant validity.
Results
Descriptive Statistics of the Sample
The total sample size was 15,871, including 7,807 males and 8,064 females. The average grip strength of males was significantly higher than that of females. The average community type score was 5.82, indicating that most of the respondents lived in non-large cities. Men had moderate PA levels that were slightly lower than those of women. Singing and dancing activities were more common among women than men. Women had higher levels of overall SA than men, but men engaged in more general social participation than women. Female upper-body pain was more common than male upper-body pain.
Composite Reliability and Convergent Validity
The CR values of the measured variables ranged from 0.746 to 0.962; a CR value above 0.6 is recommended by Bagozzi and Yi (67) and Fornell and Larcker (68); thus, the research variables were within the acceptable range. Finally, this article measured validity according to convergent and discriminant validity as proposed by Anderson and Gerbing (69). Table 2 shows that each measured variable reached significance. The AVE values ranged from 0.506 to 0.894; a value above 0.5 is recommended by; thus, the variables were all accepted. Therefore, the measurement model had good convergent validity. This result indicates that all measured models had excellent reliability and validity and were suitable for the SEM analysis.
Among the three items, the reliability (assessed by the squared multiple correlations, SMC) was the highest for PA. The validity of the general social interaction dimension of SA was relatively low but was still above 0.5. The reliability of children's income and frequency of parent-child interaction was not very strong but was still higher than the standard. The item validity values were 0.946 (PA), 0.711 (SP), and 0.898 (CR), which were all >0.7, indicating that the items had an excellent explanatory ability for the selected dimension.
Comparison of the Model Paths by Gender and Covariance Coefficient and Fit Indexes for the Whole Sample
When mediating variables are present in a model, the relationship between independent and dependent variables should be expressed as total, direct, and indirect effects. Table 3 and Figure 2 show the results of the entire sample model.

Table 3. Comparison of the model paths by age and the odds ratios and fit indexes.
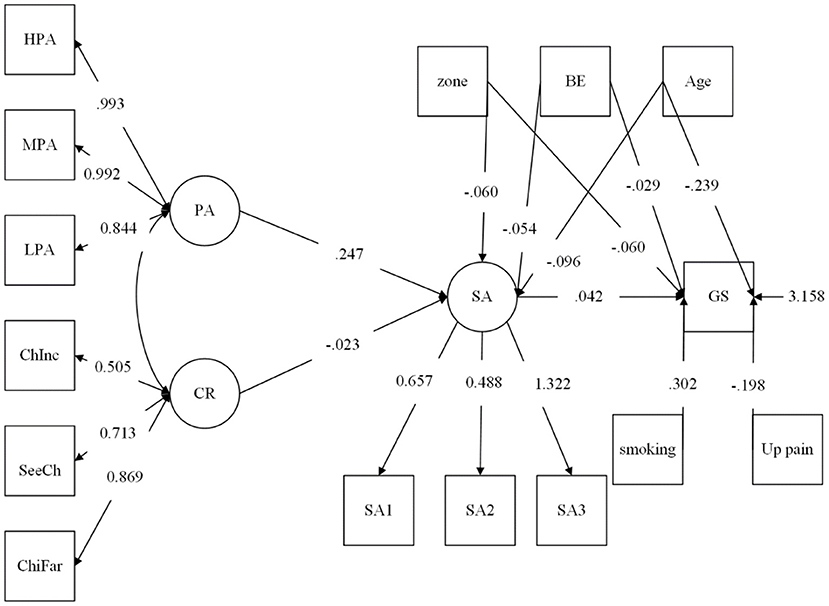
Figure 2. Standardized coefficients for the full sample model. GP, Grip strength; GENDER, gender; AREA, Area of residence; AGE, age; HPA, High physical activity; MPA, Moderate physical activity; LPA, Low physical activity; SA, Social activity; Chifar, Living near one's children; CHInc, Children's income; SeeCh, Seeing children; Up pain, Upper-body pain; BE, Basic expenditure rate.
The correlation between the relationship with adult children and SA was significant (−0.023), and the correlation between smoking and grip strength was −0.302. The correlations of upper-body pain and grip strength (−0.198), SA and PA (0.247), and SA and grip strength (0.042) were all significant.
Group Analysis
According to the various direct and indirect effects for the male and female groups, the total effect of PA on grip strength was significant for both the male group (0.007) and the female group (0.016). However, in terms of the effect of PA on grip strength, the direct effect in the male group was significant, and the direct effect in the female group was not significant, indicating that PA did not directly generate changes in grip strength. In contrast, social activity significantly affected grip strength in both the male and female groups. The effects of community differences on grip strength were significant in terms of both the total effect (−0.062) and the direct effect (−0.06) (but if this article used the 95% confidence interval, then the relationship between community differences and social participation was not significant in the male group). Thus, community difference was related to grip strength using the 95% confidence interval in the female group. Residents of areas with lower population density had lower SA levels, and residents of large cities had lower SA levels than residents of the urban-rural fringe and county-level cities. This finding shows that behavioral patterns based on an agricultural society and population density influence social participation. Notably, the direct effect of community differentiation (−0.06) on grip strength was more significant than the indirect effect (−0.002). This finding shows that community differences affect grip strength and social participation and may also affect grip strength through medical facilities and other reasons that are not yet clear. This discussion indicates a direction for follow-up research, but some studies have argued that this effect is not related to the question of whether infrastructure helps increase PA (70). The direct effect of individual age changes on grip strength (−0.243) was more significant than the indirect effect on grip strength through social participation (−0.004), indicating that the age effect of weakening grip strength is much higher than that of social participation.
Essential expenditure also affected grip strength, indicating that nutrition or eating habits also affect grip strength. The indirect effect of basic expenditure rate on grip strength through social interaction (−0.002) was much smaller than the direct effect on grip strength (−0.031), which shows that there was no significant correlation coefficient between social identity and grip strength (the direct correlation coefficient between expenditure and grip strength was much stronger than the relationship between expenditure level and social identity). See Table 3 for details. Therefore, Hypothesis A, B, C, and D are all accepted in the entire sample. However, in the male group, Hypotheses A is not accepted (see Table 4).
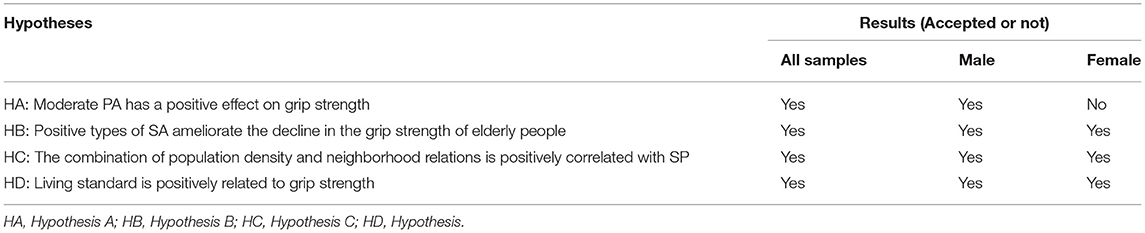
Table 4. Hypothesis test results.
Discussion
This article discussed the influence of SA and PA on grip strength based on a sample from the CHARLS, analyzed the factors that affect social interaction and PA and the interaction between the two variables, and finally examined these effects within structural equation models of the effect on the change in grip strength.
Regional Differences
Some studies have discussed the differences in behavior and health status between urban and rural areas in developed countries (71). Some papers studied the differences in social life, including health, between urban and rural areas in developing countries (72). However, it is not mentioned that the difference in interaction patterns between urban and rural areas in developed and developing countries is due to rural living habits. Especially in health research, various urban and rural community forms are divided in detail according to different population densities and behavior patterns (rather than simply separating into rural and urban areas). There are very few studies like that, concentrated on spatial economic analysis (73). As for the SEM of community differences (between urban and rural areas divided by population density and behavior)—social activities—health, it has not been found in the open literature. According to the empirical analysis results of this study, Chinese elderly people who visit their families and friends, play card games, and dance have more obvious correlations with grip strength. Result also shows that the community difference caused by the frequency of social activities can better explain the relationship between the grip strength of the elderly and the community difference than the difference caused by the simple population density. The reason behind this difference may be caused by different ways of interpersonal communication.
Age
The efforts of non- intervening exogenous variables such as age on grip strength can be found to be partially intervenable, rather than only be used as control variables (74, 75). However, the relationship between age growth and social activities is not so significant. This shows that it is a way to improve grip strength by intervening the correlation coefficient between age and social activities to increase beneficial social activities to delay the reduction of grip strength, although the effect is limited. Similarly, the effect of marital status on grip strength can also be decomposed by SEM.
Social Activities
Quirke et al. (76) believe that the impact of for the taking care of grandchildren on other social activities and self-rated well-being is complex. This study does not discuss the competitive relationship between the taking care of grandchildren and other social activities but expands the scope of social activities to consider the impact on grip strength. There is no such practice in other articles on grip strength and social activities (77, 78).
Physical Activity
The direct effect of PA on grip strength was significantly negative, and the effect of PA on promoting SA was significant. This result is similar to the idea of, Kuh et al. (35) and Jenkin et al. (79). Suppose grip strength is an essential indicator or even the only indicator of health (other than self-rated health) among elderly people. In that case, the strategy of increasing physical exercise among middle-aged and older people may be an option that needs to be more carefully reviewed. In other words, we need to pay more attention to the conclusion made by Yu et al. (78) that the change of grip strength can be improved by increasing social activities rather than physical activities.
Further Work
Areas for further work include the identification of more variables in the questionnaire that better describe community differences and the use of more biomarkers to indicate weakness to allow the analysis of environmental differences in more detail as well as physical exercise, social participation, and the relationship between specific indicators of the health of elderly people. In addition, in the future, it will also be necessary to use longitudinal data to reflect the cause-and-effect relationship when the sample size and sample periods are sufficient.
The relationship between cognition and SA was not examined in this study because cognition and SA have two-way interactions, and the relationship between grip strength and other variables such as cognition may also be two-way due to the complexity of the problem, rendering these variables more suitable for a separate research project.
The relationship between regional differences and social relations, as well as the relationship between regional differences and grip strength, may not be limited to differences in economic conditions, environmental conditions, and SP; they may also involve other aspects of urban and rural differences in China, such as long-term physical labor vs. grip strength and differences in the nutritional structure during adolescence. Therefore, a study making comparisons based on regional differences to examine the relationship between grip strength and regional differences through social interaction may have the problem of missing variables.
The social items on the questionnaire could be classified as general social interactions or different types of SP. However, according to this classification, the sample size for some types was too small, which affected the significance of the statistical results. In other words, due to the lack of data samples, such classifications could not be tested extensively. Therefore, our results suggest that general SA positively affects grip strength, and there is no way to distinguish between the differences among different kinds of activities.
The grip strength-to-weight ratio was not used because the correlation between grip strength and weight is not strong enough, and adding weight may complicate the problem.
Limitations
There are some limitations to this study. First, a more detailed analysis by age group is recommended; the sample used focused on the 50–69-year-old population, and the elderly population over 70 years old was much smaller than the younger elderly sample. Since the sample sizes of each age group were so different, the age groups were ignored. Second, regarding whether to use confirmatory factor analysis, there are also many works on the health of elderly people that do not use latent variables but directly use all measured variables. We also tried to construct a structural equation model with a single measurable indicator, and the general conclusion was similar to the result using factor analysis. The structural equation model, including factor analysis, was used to correct the measurement errors at the cost of not performing more detailed analyses.
Conclusion
The contribution of this study lies in (1) establishing a structural equation model including community differences, social activities, and specific biomarkers; (2) comparing the direct and intermediate effects of age and gender on grip strength, indicating that the effects of age and gender on grip strength can be intervened; (3) based on the difference of population density and social habits, we modified the scoring criteria of community types and ranked them, to reveal more insights into the difference of social activities between urban and rural areas on physical health indicators; (4) including the occasional care of grandchildren and elderly parents into the scope of active social activities. The positive effect of positive social activities on grip strength was further confirmed.
This study enriches the research of grip strength in the elderly population, increases the complexity of the understanding of the intermediate effects, and indicates that the influence of non-interventional exogenous variables such as age and gender on grip strength is partially endogenous (intervenable) through the separation of the intermediate effects and the comparison of the indirect and direct effects. The community differentiation approach differs from that in the original questionnaire, revealing the characteristics of the SA of elderly residents in urban and rural areas in China and the impact of these differences on grip strength.
The inspiration for this study to formulate policies and support for the elderly population lies in the importance of community differentiation. In contrast to common perception, the community interactions of elderly residents living at the junction of urban and rural areas are higher than those of elderly residents in large urban centers. This finding indicates that some behavioral patterns associated with agricultural society are beneficial to the SA of elderly people. In addition, according to the coefficient of the effect of basic expenditure level on grip strength, improving quality of life requires unremitting efforts to improve physical health. Finally, the importance of elderly people's interactions with their adult children for their health in East Asian countries needs to be emphasized. Encouraging childbirth is a policy option as circumstances permit.
Data Availability Statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found in the article/Supplementary Material.
Ethics Statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. The patients/participants provided their written informed consent to participate in this study. Ethical approval for all the CHARLS waves was granted from the Institutional Review Board at Peking University. The IRB approval number for the main household survey, including anthropometrics, is IRB00001052-11015; the IRB approval number for biomarker collection, was IRB00001052-11014.
Author Contributions
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
Funding
This research was funded by the Project of the Natural Science Foundation of Liaoning Province, China (Grant No. 71490735) and Social Science Fund of Liaoning Province, China (Grant No. L19BGL035).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2021.755695/full#supplementary-material
Abbreviations
PA, Physical activity; SP, Social participation; RL, Relation with adult children; SPA, Slight physical activity; GSP, General social participation; ISS, Informed social support; GS, Grip strength.
References
1. Alley DE, Shardell MD, Peters KW, McLean RR, Dam TTL, Kenny AM, et al. Grip strength cutpoints for the identification of clinically relevant weakness. J Gerontol A Biol Sci Med Sci. (2014) 69:559–66. doi: 10.1093/gerona/glu011
2. Bemben D, Stark C, Taiar R, Bernardo-Filho M. Relevance of whole-body vibration exercises on muscle strength/power and bone of elderly individuals. Dose Response. (2018) 16:1559325818813066. doi: 10.1177/1559325818813066
3. Cristino de Souza AL, Mendonça VA, Coelho de Oliveira AC, Ferreira da Fonseca S, Mello Santos LM, Cunha Fernandes JS, et al. Whole body vibration in the static modified push-up position in untrained healthy women stimulates neuromuscular system potentiating increased handgrip myogenic response. J Bodyw Mov Ther. (2020) 24:233–8. doi: 10.1016/j.jbmt.2020.06.021
4. Delaire L, Courtay A, Fauvernier M, Humblot J, Bonnefoy M. Integrating a prevention care path into the daily life of older adults with mobility disability risk: introducing a predictive response model to exercise. Clin Interv Aging. (2021) 16:1617–29. doi: 10.2147/CIA.S315112
5. Gómez F, Osorio-García D, Panesso L, Curcio C.-L. Healthy aging determinants and disability among older adults: SABE Colombia. Rev Panam Salud Publica. (2021) 45:e98. doi: 10.26633/RPSP.2021.98
6. Syddall H, Cooper C, Martin F, Briggs R, Aihie Sayer A. Is grip strength a useful single marker of frailty? Age Ageing. (2003) 32:650–6. doi: 10.1093/ageing/afg111
7. Buchman AS, Wilson RS, Boyle PA, Bienias JL, Bennett DA. Grip strength and the risk of incident Alzheimer's disease. Neuroepidemiology. (2007) 29:66–73. doi: 10.1159/000109498
8. Norman K, Stobäus N, Gonzalez MC, Schulzke JD, Pirlich M. Hand grip strength: outcome predictor and marker of nutritional status. Clin Nutr. (2011) 30:135–42. doi: 10.1016/j.clnu.2010.09.010
9. Cawthon PM, Travison TG, Manini TM, Patel S, Pencina KM, Fielding RA, et al. Establishing the link between lean mass and grip strength cut points with mobility disability and other health outcomes: proceedings of the sarcopenia definition and outcomes consortium conference. J Gerontol A Biol Sci Med Sci. (2020) 75:1317–23. doi: 10.1093/gerona/glz081
10. Sayer AA, Kirkwood TBL. Grip strength and mortality: a biomarker of ageing? Lancet. (2015) 386:226–7. doi: 10.1016/S0140-6736(14)62349-7
11. Peterson MD, Duchowny K, Meng Q, Wang Y, Chen X, Zhao Y. Low normalized grip strength is a biomarker for cardiometabolic disease and physical disabilities among U.S. and Chinese adults. J Gerontol Ser A. (2017) 72:1525–31. doi: 10.1093/gerona/glx031
12. Wang T, Wu Y, Li W, Li S, Sun Y, Li S, et al. Weak grip strength and cognition predict functional limitation in older EUROPEANS. J Am Geriatr Soc. (2018) 67:93–9. doi: 10.1111/jgs.15611
13. Han SH, Tavares JL, Evans M, Saczynski J, Burr JA. Social activities, incident cardiovascular disease, and mortality. J Aging Health. (2016) 29:268–88. doi: 10.1177/0898264316635565
14. Jeong SM, Seo BK, Park YC, Baek YH. A review of complementary and alternative medicine therapies on muscular atrophy: a literature review of in vivo/in vitro studies. Evid Based Complement Alternat Med. (2018) 2018:8654719. doi: 10.1155/2018/8654719
15. Boonpor J, Parra-Soto S, Petermann-Rocha F, Ferrari G, Welsh P, Pell JP, et al. Associations between grip strength and incident type 2 diabetes: findings from the UK Biobank prospective cohort study. BMJ Open Diabetes Res Care. (2021) 9:e001865. doi: 10.1136/bmjdrc-2020-001865
16. Jo NG, Kang SR, Ko MH, Yoon JY, Kim HS, Han KS, et al. Effectiveness of whole-body vibration training to improve muscle strength and physical performance in older adults: prospective, single-blinded, randomized controlled trial. Healthcare. (2021) 9:652. doi: 10.3390/healthcare9060652
17. Jancova-Vseteckova J, Bobak M, Kubinova R, Capkova N, Peasey A, Marmot MG, et al. Social patterning in grip strength, chair rise, and walk speed in an aging population: the czech HAPIEE study. J Aging Phys Act. (2015) 23:264–71. doi: 10.1123/japa.2013-0142
18. Petersen GL, Mortensen EL, Rod NH, Lange T, Flensborg-Madsen T, Hansen ÅM, et al. Occupational social class and personality traits in relation to leisure-time physical activity level: cross-sectional results from the copenhagen aging and midlife biobank. J Aging Health. (2017) 30:1263–83. doi: 10.1177/0898264317714928
19. Schulz M, Romppel M, Grande G. Built environment and health: a systematic review of studies in Germany. J Publ Health. 2018, 40:8–15. doi: 10.1093/pubmed/fdw141
20. Stappers NEH, Van Kann DHH, Ettema D, De Vries NK, Kremers SPJ. The effect of infrastructural changes in the built environment on physical activity, active transportation and sedentary behavior – a systematic review. Health Place. (2018) 53:135–49. doi: 10.1016/j.healthplace.2018.08.002
21. Rowe JW, Kahn RL. Successful aging 2.0: conceptual expansions for the 21st century. J Gerontol Ser B Psychol Sci Soc Sci. (2015) 70:593–6. doi: 10.1093/geronb/gbv025
22. Douglas H, Georgiou A, Westbrook J. Social participation as an indicator of successful aging: an overview of concepts and their associations with health. Austra Health Rev. (2017) 41:455. doi: 10.1071/AH16038
23. Pao YC, Chen CY, Chang CI, Chen CY, Tsai JS. Self-reported exhaustion, physical activity, and grip strength predict frailty transitions in older outpatients with chronic diseases. Medicine. (2018) 97:e10933. doi: 10.1097/MD.0000000000010933
24. Santanasto AJ, Glynn NW, Lovato LC, Blair SN, Fielding RA, Gill TM, et al. Effect of physical activity versus health education on physical function, grip strength and mobility. J Am Geriatr Soc. (2017) 65:1427–33. doi: 10.1111/jgs.14804
25. Mohd Hairi F, Mackenbach JP, Andersen-Ranberg K, Avendano M. Does socio-economic status predict grip strength in older Europeans? Results from the SHARE study in non-institutionalised men and women aged 50+. J Epidemiology Commun Health. (2009) 64:829–37. doi: 10.1136/jech.2009.088476
26. Faulkner JA, Larkin LM, Claflin DR, Brooks SV. Age-Related changes in the structure and function of skeletal muscle. Clin Exp Pharmacol Physiol. (2007) 34:1091–96. doi: 10.1111/j.1440-1681.2007.04752.x
27. Frederiksen H, Hjelmborg J, Mortensen J, McGue M, Vaupel J, Christensen K. Age trajectories of grip strength: cross-sectional and longitudinal data among 8,342 danes aged 46 to 102. Ann Epidemiol. (2006) 16:554–62. doi: 10.1016/j.annepidem.2005.10.006
28. Hamer M, Molloy GJ. Association of C-reactive protein and muscle strength in the english longitudinal study of ageing. Age. (2009) 31:171–7. doi: 10.1007/s11357-009-9097-0
29. Daskalopoulou C, Stubbs B, Kralj C, Koukounari A, Prince M, Prina AM. Physical activity and healthy ageing: a systematic review and meta-analysis of longitudinal cohort studies. Ageing Res Rev. (2017) 38:6–17. doi: 10.1016/j.arr.2017.06.003
30. Bann D, Hire D, Manini T, Cooper R, Botoseneanu A, McDermott MM, et al. Light intensity physical activity and sedentary behavior in relation to body mass index and grip strength in older adults: cross-sectional findings from the lifestyle interventions and independence for elders (LIFE) study. PLoS ONE. (2015) 10:e0116058. doi: 10.1371/journal.pone.0116058
31. Lang I, Guralnik J, Wallace RB, Melzer D. what level of alcohol consumption is hazardous for older people? Functioning and mortality in U.S. and english national cohorts. J Am Geriatr Soc. (2007) 55:49–57. doi: 10.1111/j.1532-5415.2006.01007.x
32. Leyk D, Gorges W, Ridder D, Wunderlich M, Rüther T, Sievert A, et al. Hand-grip strength of young men, women and highly trained female athletes. Eur J Appl Physiol. (2006) 99:415–21. doi: 10.1007/s00421-006-0351-1
33. Noble JW, Eng JJ, Kokotilo KJ, Boyd LA. Aging effects on the control of grip force magnitude: an fMRI study. Exp Gerontol. (2011) 46:453–61. doi: 10.1016/j.exger.2011.01.004
34. Celis-Morales CA, Lyall DM, Anderson J, Iliodromiti S, Fan Y, Ntuk UE, et al. The association between physical activity and risk of mortality is modulated by grip strength and cardiorespiratory fitness: evidence from 498 135 UK-Biobank participants. Eur Heart J. (2017) 38:116–22. doi: 10.1093/eurheartj/ehw249
35. Kuh D, Bassey EJ, Butterworth S, Hardy R, Wadsworth MEJ. Grip strength, postural control, and functional leg power in a representative cohort of british men and women: associations with physical activity, health status, socioeconomic conditions. J Gerontol Ser A. (2005) 60:224–31. doi: 10.1093/gerona/60.2.224
36. Malkesman O, Maayan R, Weizman A, Weller A. Aggressive behavior and HPA axis hormones after social isolation in adult rats of two different genetic animal models for depression. Behav Brain Res. (2006) 175:408–14. doi: 10.1016/j.bbr.2006.09.017
37. McGue M, Christensen K. Social activity and healthy aging: a study of aging danish twins. Twin Res Hum Genet. (2007) 10:255–65. doi: 10.1375/twin.10.2.255
38. Crooks VC, Lubben J, Petitti DB, Little D, Chiu V. Social network, cognitive function, and dementia incidence among elderly women. Am J Public Health. (2008) 98:1221–7. doi: 10.2105/AJPH.2007.115923
39. Momtaz YA, Haron SA, Ibrahim R, Hamid TA. Social embeddedness as a mechanism for linking social cohesion to well-being among older adults: moderating effect of gender. Clin Interv Aging. (2014) 9:863–70. doi: 10.2147/CIA.S62205
40. Lou VWQ, Chi I, Kwan CW, Leung AYM. Trajectories of social engagement and depressive symptoms among long-term care facility residents in Hong Kong. Age Ageing. (2012) 42:215–22. doi: 10.1093/ageing/afs159
41. Salvador A. Steroid hormones and some evolutionary-relevant social interactions. Motiv Emot. (2011) 36:74–83. doi: 10.1007/s11031-011-9265-2
42. Lyu J, Lee SH, Kim HY. Associations between healthy lifestyles and health outcomes among older Koreans. Geriatr Gerontol Int. (2015) 16:663–9. doi: 10.1111/ggi.12531
43. Robins LM, Hill KD, Finch CF, Clemson L, Haines T. The association between physical activity and social isolation in community-dwelling older adults. Aging Ment Health. (2016) 22:175–82. doi: 10.1080/13607863.2016.1242116
44. Ashida S, Sewell DK, Schafer EJ, Schroer AL, Friberg JE. Social network functions related to co-engagement in social activity and psychological well-being. Innovat Aging. (2017) 1:1178. doi: 10.1093/geroni/igx004.4292
45. Yorke AM, Curtis AB, Shoemaker M, Vangsnes E. The impact of multimorbidity on grip strength in adults age 50 and older: data from the health and retirement survey (HRS). Arch Gerontol Geriatr. (2017) 72:164–8. doi: 10.1016/j.archger.2017.05.011
46. Lindsay Smith G, Banting L, Eime R, O'Sullivan G, van Uffelen JGZ. The association between social support and physical activity in older adults: a systematic review. Int J Behav Nutr Phys Act. (2017) 14:56. doi: 10.1186/s12966-017-0509-8
47. Gilmore KJ, Kirk EA, Doherty TJ, Rice CL. Effect of very old age on anconeus motor unit loss and compensatory remodelling. Muscle Nerve. (2017) 57:659–63. doi: 10.1002/mus.25982
48. Carver LF, Beamish R, Phillips SP, Villeneuve M. A scoping review: social participation as a cornerstone of successful aging in place among rural older adults. Geriatrics. (2018) 3:75. doi: 10.3390/geriatrics3040075
49. Ho EC, Hawkley L, Dale W, Waite L, Huisingh-Scheetz M. Social capital predicts accelerometry-measured physical activity among older adults in the U.S: a cross-sectional study in the national social life, health, aging project. BMC Public Health. (2018) 18:804. doi: 10.1186/s12889-018-5664-6
50. Vogelsang EM. Older adult social participation and its relationship with health: rural-urban differences. Health Place. (2016) 42:111–9. doi: 10.1016/j.healthplace.2016.09.010
51. Lai DWL, Li J, Lee VWP, Dong X. Environmental factors associated with chinese older immigrants' social engagement. J Am Geriatr Soc. (2019) 67:S571–6. doi: 10.1111/jgs.15899
52. Wang R, Chen Z, Zhou Y, Shen L, Zhang Z, Wu X. Melancholy or mahjong? Diversity, frequency, type, and rural-urban divide of social participation and depression in middle- and old-aged chinese: a fixed-effects analysis. Soc Sci Med. (2019) 238:112518. doi: 10.1016/j.socscimed.2019.112518
53. Zheng Z, Chen H, Yang L. Transfer of promotion effects on elderly health with age: from physical environment to interpersonal environment and social participation. Int J Environ Res Public Health. (2019) 16:2794. doi: 10.3390/ijerph16152794
54. Lei X, Smith JP, Sun X, Zhao Y. Gender differences in cognition in China and reasons for change over time: evidence from CHARLS. J Econ Ageing. (2014) 4:46–55. doi: 10.1016/j.jeoa.2013.11.001
55. Zhao Y, Strauss J, Chen X, Wang Y, Gong J, Meng Q, et al. China Health and Retirement Longitudinal Study Wave 4 User's Guide. Beijing: Peking University (2020).
56. Zhao Y, Hu Y, Smith JP, Strauss J, Yang G. Cohort profile: the China health and retirement longitudinal study (CHARLS). Int J Epidemiol. (2014) 43:61–8. doi: 10.1093/ije/dys203
57. Yang R, Xu Q, Long H. Spatial distribution characteristics and optimized reconstruction analysis of China's rural settlements during the process of rapid urbanization. J Rural Stud. (2016) 47:413–24. doi: 10.1016/j.jrurstud.2016.05.013
58. Li J, Li J, Yuan Y, Li G. Spatiotemporal distribution characteristics and mechanism analysis of urban population density: a case of Xi'an, Shaanxi, China. Cities. (2019) 86:62–70. doi: 10.1016/j.cities.2018.12.008
59. Zhang Z, Liu F, Zhao X, Wang X, Shi L, Xu J, et al. Urban expansion in China based on remote sensing technology: a review. Chin GeographAQQ29 Sci. (2018) 28:727–43. doi: 10.1007/s11769-018-0988-9
60. Norstrand JA, Xu Q. Social capital and health outcomes among older adults in china: the urban-rural dimension. Gerontologist. (2011) 52:325–34. doi: 10.1093/geront/gnr072
61. Li L, Lantao W. Research on rural public space reconstruction for the aged from the perspective of community endowment—taking jinqiao village in fengyang as an example. IOP Conf Ser Earth Environ Sci. (2020) 525:012076. doi: 10.1088/1755-1315/525/1/012076
62. Lin M, Graefe AR. Roller-skating into the big city: a case study of migrant workers' informal leisure activity in Guangzhou, China. J Leisure Res. (2019) 50:181–200. doi: 10.1080/00222216.2019.1568846
63. Liu J, Rozelle S, Xu Q, Yu N, Zhou T. Social engagement and elderly health in China: evidence from the China health and retirement longitudinal survey (CHARLS). Int J Environ Res Public Health. (2019) 16:278. doi: 10.3390/ijerph16020278
64. Cheval B, Orsholits D, Sieber S, Courvoisier D, Cullati S, Boisgontier MP. Relationship between decline in cognitive resources and physical activity. Health Psychol. (2020) 39:519–28. doi: 10.1037/hea0000857
65. Hu H, Liu W, Zhang S, Pan J, Zheng X. Depression mediates the relationship between smoking and pain: evidence from a nationally representative study in a low- and middle-income country. Addict Behav. (2021) 119:106937. doi: 10.1016/j.addbeh.2021.106937
66. Li L, Loo BPY. Mobility impairment, social engagement, and life satisfaction among the older population in China: a structural equation modeling analysis. Qual Life Res. (2016) 26:1273–82. doi: 10.1007/s11136-016-1444-x
67. Bagozzi RP, Yi Y. On the evaluation of structural equation models. J Acad Market Sci. (1988) 16:74–94. doi: 10.1007/BF02723327
68. Fornell C, Larcker DF. Structural equation models with unobservable variables and measurement error: algebra and statistics. J Market Res. (1981) 18:382. doi: 10.2307/3150980
69. Anderson JC, Gerbing DW. Structural equation modeling in practice: a review and recommended two-step approach. Psychol Bull. (1988) 103:411–23. doi: 10.1037/0033-2909.103.3.411
70. Zheng Z, Yang L. Neighborhood environment, lifestyle, and health of older adults: comparison of age groups based on ecological model of aging. Sustainability. (2019) 11:2077. doi: 10.3390/su11072077
71. Johnson JA, Johnson AM. Urban-Rural differences in childhood and adolescent obesity in the united states: a systematic review and meta-analysis. Childh Obes. (2015) 11:233–41. doi: 10.1089/chi.2014.0085
72. McGee TG. Managing the rural–urban transformation in East Asia in the 21st century. Sustain Sci. (2008) 3:155–67. doi: 10.1007/s11625-007-0040-y
73. Helbich M, Leitner M. Spatial analysis of the urban-to-rural migration determinants in the Viennese metropolitan area. A transition from suburbia to postsuburbia? Appl Spatial Anal Policy. (2009) 2:237–260. doi: 10.1007/s12061-009-9026-8
74. Massy-Westropp NM, Gill TK, Taylor AW, Bohannon RW, Hill CL. Hand grip strength: age and gender stratified normative data in a population-based study. BMC Res Notes. (2011) 4:127. doi: 10.1186/1756-0500-4-127
75. Beller J, Miething A, Regidor E, Lostao L, Epping J, Geyer S. Trends in grip strength: age, period, and cohort effects on grip strength in older adults from Germany, Sweden, and Spain. SSM Popul Health. (2019) 9:100456. doi: 10.1016/j.ssmph.2019.100456
76. Quirke E, König HH, Hajek A. Association between caring for grandchildren and feelings of loneliness, social isolation and social network size: a cross-sectional study of community dwelling adults in Germany. BMJ Open. (2019) 9:e029605. doi: 10.1136/bmjopen-2019-029605
77. Shah KN, Lin FV, Yu F, McMahon JM. Activity engagement and physical function in old age sample. Arch Gerontol Geriatr. (2017) 69:55–60. doi: 10.1016/j.archger.2016.11.007
78. Yu B, Steptoe A, Niu K, Jia X. Social isolation and loneliness as risk factors for grip strength decline among older women and men in China. J Am Med Dir Assoc. (2020) 21:1926–30. doi: 10.1016/j.jamda.2020.06.029
Keywords: health of elderly people, grip strength, community differences, interpersonal environment, social participant, gender differences
Citation: Lin H and Ren H (2021) The Influence of Interpersonal Behaviors and Population Density on Grip Strength of Elderly People: An Analysis of the Direct vs. Indirect Effects via Social Participation. Front. Public Health 9:755695. doi: 10.3389/fpubh.2021.755695
Received: 11 August 2021; Accepted: 05 November 2021;
Published: 10 December 2021.
Edited by:
Marcia G. Ory, Texas A& M University, United StatesReviewed by:
Mario Bernardo-Filho, Rio de Janeiro State University, BrazilPatricia M. Alt, Towson University, United States
Copyright © 2021 Lin and Ren. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Haijun Ren, renhaijun456@outlook.com; orcid.org/0000-0001-9957-9902