 Massimo Apicella1*
Massimo Apicella1* Marcella Caterina Pisa1Roberto Averna1Milena Labonia1
Marcella Caterina Pisa1Roberto Averna1Milena Labonia1 Maria Pontillo1
Maria Pontillo1 Stefano Vicari1,2
Stefano Vicari1,2- 1Child Neuropsychiatry Unit, Department of Neuroscience, Bambino Gesù Children’s Hospital, IRCCS, Rome, Italy
- 2Department of Life Sciences and Public Health, Catholic University, Rome, Italy
Introduction: Few studies on adolescents have investigated intelligence quotient (IQ) in mood disorders. Evidence on Disruptive Mood Dysregulation Disorder (DMDD), a controversial entity among depressive disorders, is more limited.
Materials and methods: We performed an exploratory study on adolescent inpatients with unipolar mood disorders to test specific impairment in cognitive and adaptive profile. We also considered common psychopathological comorbidities. We retrospectively collected data on inpatients with a diagnosis of major depressive disorder (MDD), DMDD or Depressive Disorder – Not Otherwise Specified (DD-NOS) evaluated with Wechsler Scales of Intelligence, Adaptive Behavior Assessment System (ABAS-II), and Children’s Global Assessment Scale (C-GAS).
Results: Out of 198 inpatients (85.9% females), 33.3% had MDD, 60.1% DD-NOS and 6.6% DMDD. DMDD patients had higher rates of ADHD (15.4%) and learning disorders (LD, 23.1%), a lower mean IQ (87.8 ± 10.7; p = 0.001) and ABAS-II scores (general composite 68.8 ± 16.8; p = 0.002) than other groups. In linear regression analysis, DMDD retained a significant correlation with lower IQ and adaptive abilities when controlling for sex, and comorbidities. Among comorbidities, LD correlated with lower perceptual reasoning and IQ, and ADHD with lower conceptual adaptive abilities. In all diagnosis groups, working memory and processing speed were lower than verbal comprehension and perceptual reasoning.
Discussion: While impairment in working memory and processing speed is a non-specific correlate of active mood disorder, DMDD is burdened by lower general intelligence and adaptive abilities and higher rate of neurodevelopmental comorbidities. Lower IQ in the normal range is a correlate of DMDD among variables examined, not explained by the effect of neurodevelopmental comorbidities. These findings are discussed with regards to possible implications for the consideration of DMDD as a bridge condition between neurodevelopmental disorders and mood disorders.
1 Introduction
Mood disorders in adolescents are common and increasing in prevalence in recent times (1, 2). Unipolar depression is a particularly common and potentially disabling condition in adolescence (3), while bipolar disorder is rarer, but particularly severe (4). Chronic irritability is a common reason for a child and adolescent psychiatric consultation (5) and requires a careful psychodiagnostics evaluation. In DSM-5 (6), it appears among the diagnostic criteria of different non affective disorders such as Oppositional Defiant Disorder (ODD) and intermittent explosive disorder, among others (7). In children and adolescents, it is a main diagnostic feature for major depression. At this age, however, severe irritability is also the most common presentation of mania (8). Leibenluft et al. (9) described “broad phenotype” of pediatric bipolar disorder as characterized by chronic severe irritability. Following studies, however, clarified that children and adolescents with chronic irritability uncommonly progress to adult bipolar phenotypes (10) and more commonly develop major depressive disorder (MDD) and anxiety disorders (11). Furthermore, patients with severe mood dysregulation (SMD), an operationalization of severe chronic disability before DSM-5, rarely have family history of bipolar disorder (12). DSM-5, therefore, introduced the diagnosis of Disruptive Mood Dysregulation Disorder (DMDD) among depressive and related disorders to avoid overdiagnosis of pediatric bipolar disorder. This diagnosis and its placement among depressive and related disorders, however, has been criticized by many authors. Some remark the difficulty to distinguish DMDD from bipolar disorder in clinical settings (13), others comment on the difficulty to distinguish it from ODD (14) and neurodevelopmental disorders (15, 16). Some criticize the conceptualization of DMDD as a unique and separate disorder (17, 18), underlining possible overlap in neurobiology (19) and trajectory (16) between DMDD and attention deficit hyperactivity disorder (ADHD) subtypes. One study has recently evaluated DMDD in the framework of depressive and related disorders, by comparing clinical correlates, natural course, and vulnerability factors of inpatients with MDD, persistent depressive disorder and DMDD (20). Vulnerability factors were comparable among groups, but DMDD was characterized by more externalizing and trauma-related disorders, peer-relationship and school difficulties in comparison to MDD and persistent depressive disorder.
Cognitive domain is underinvestigated in mood disorders of adolescents in comparison to adults, and evidence on DMDD is particularly limited. A cognitive symptoms cluster is relevant in depression (21–23) and mania (24) and cognitive impairment may help characterize mood disorders and understand neural substrates involved in their pathogenesis (25).
There is some evidence that a lower Intelligence Quotient (IQ) is a nonspecific correlate across all psychiatric diagnoses (26, 27). With regard to studies on adults, IQ and working memory index (WMI) are impaired during unipolar depression (28) and cognitive impairment correlates with the severity of depressive symptoms in both unipolar and bipolar depression (29). Adults with bipolar disorder show a grade of impairment with lower inhibitory control, selective attention and verbal and visual memory performances even when euthymic (30). Premorbid IQ of patients with bipolar disorder, however, is not lower than the general population (31, 32).
Studies on cognition in adolescents with mood disorders are fewer and report less remarkable differences in neuropsychological profiles, compared to those on adults. Lower premorbid IQ in developmental age has also been described as a risk factor for MDD (33). A study with Wechsler Intelligence Scale for Children (WISC) III and executive functions in children found only lower PSI and trial making test performance in patients with MDD (34).
Association between DMDD and lower school functioning is remarkable (35, 36), and this is partly accounted for by a high rate of comorbid learning disorders (LD) (37). Studies on neuropsychology of patients with SMD are apparently contradictory. In Adelman et al. (38) no differences were found in IQ between patients with SMD or bipolar disorder and controls, while in Rau et al. (39) SMD patients had slightly lower IQ at Wechsler abbreviated scale of intelligence. Recent literature has shown poorer motor inhibition, more developmental motor coordination disorder and written language disorder in DMDD than in psychiatric controls (37).
In a transdiagnostic approach, irritability has been shown to impact the association between inattention symptoms and difference in processing efficiency between conflict and non-conflict conditions in ADHD (40). This finding suggests DMDD patients may have a specific impairment when ADHD is also present. ADHD and LD are frequent comorbidities in adolescent depressive disorders, particularly in DMDD (20), and are known to influence intellective performance on Wechsler scales. Few studies have investigated cognitive abilities in mood disorders comorbid with ADHD and LD. In a study on adolescents with autism spectrum disorder, ADHD, or LD and comorbid anxiety, depression and behavior disorders, neurodevelopmental disorder modified significantly WISC III scores, while anxiety and affective comorbidities did not (41). In a more recent study on neuropsychology of neurodevelopmental and affective comorbid disorders in adults, however, depression exhibited a distinctive additive effect on ADHD patients, with more impaired processing speed, delayed recall of conceptual verbal information and shifting tasks (42).
Adaptive abilities and functioning show a grade of correlation with intelligence (43) but represent different constructs and hardly overlap. Performing adaptive abilities requires the integration of cognition, emotions, and behaviors to meet the demands of different environments (44). Tests of adaptive abilities measure abilities which are actually performed, a parameter which can be modified over time more than cognition (45). Functioning does not only relate to adaptive abilities performed, but is also affected by different maladaptive behaviors (46). Adaptive abilities are under-investigated in adolescents with mood disorders. General functioning in adolescents with different depressive and related disorders has been studied by some authors with mixed results (42).
We performed an exploratory study on cognitive, adaptive ability and general functioning in a cohort of adolescent inpatients with unipolar mood disorders, admitted in our psychiatry inpatients unit for acute decompensation, to better describe consistency of these different phenotypes. We aim to test two hypotheses:
1. Different unipolar disorders (MDD, DMDD and depressive disorder Not Otherwise specified DD-NOS) are characterized by distinctive impairment in cognitive and adaptive profile and functioning.
2. The diagnosis of mood disorder accounts for a difference in cognitive and adaptive profile and functioning among the different groups studied when controlling for neurodevelopmental and other psychopathological comorbidities.
2 Materials and methods
2.1 Population
We conducted a retrospective study on inpatients admitted from 2020 to 2022 to the Child Neuropsychiatry Unit of a referral center for children and adolescent psychiatry. We collected data on consecutive patients admitted for the first time, referred by either our own or regional emergency departments, secondary care (child psychiatrists in national healthcare centers) or our own outpatient service. We included children and adolescents of both sexes aged ≥11 to <18 years at admission with a diagnosis of DMDD, MDD or DD-NOS. We excluded patients with intellectual disability of mild to profound severity and/or full-scale IQ <70, patients with a diagnosis of (hypo)manic/mixed episode, patients with a diagnosis of substance-induced mood disorder and/or mood disorder due to another medical condition according to DSM-5 (6), patients with neurological comorbidities reported on history or diagnosed during hospitalization. Parents/legal guardians of each patient provided written, informed consent at clinic intake for potential research analysis and anonymous reporting of findings in aggregate form, in compliance with research ethics and with Italian legal and ethical requirements for clinical data. The study was approved by our institutional review board (Ethics Committee, Ospedale Pediatrico Bambino Gesù, Reference no. 2921/2022).
2.2 Measures of evaluation
Sociodemographic data were collected on clinical records on admission. Neuropsychological and psychopathology assessment was completed within 48 hours of admission. Diagnoses were assessed with the Kiddie-Schedule for Affective Disorders and Schizophrenia for School-aged Children, Present and Lifetime version (K-SADS-PL) (47), following DSM-5 criteria (6). Comorbidities were assessed with the same instrument of evaluation. Data on LD were collected by chart review, and confirmed only if structured standardized tests appropriate to scholarity had been performed and confirmed the presence of a LD. If subthreshold psychotic symptoms were detected or in case of clinical suspicion, SIPS/SOPS interview (48) was administered to investigate the presence of prodromal syndrome (ultra-high-risk state for psychosis, UHR), which has been further analyzed as a comorbid condition. The interview is composed of 19 items, each representing a different possible subthreshold psychotic symptom, yielding 4 constructs: positive, negative, disorganized, and general symptoms. Each item is rated on a 7-point scale (49) and the spectrum of high-risk states was defined as per current literature (50).
All diagnoses were reviewed before discharge by two independent expert clinicians (M.A. and R.A.) and agreement was reached in every included case.
Measures of cognitive profile were Wechsler intelligence batteries. WISC-IV (51) was used for patients aged 16 or under and Wechsler Adult Intelligence Scale (WAIS-IV) (52) was used for patients 17 years old or above. Both batteries comprised of 10 core subtests which combine to form four psychometrically validated factor scores: the Verbal Comprehension Index (VCI), the Perceptual Reasoning Index (PRI), the WMI and the PSI. All 10 subtests combine to form a full-scale IQ (FSIQ) score. FSIQ and composite scores of VCI, PRI, WMI and PSI were used for the analysis. Single subtests of the scale were always less discrepant than 5 points at an individual case level in included patients, so the four indexes were interpretable, supplemental subtests were not used. When the FSIQ was difficult to interpret because of a difference between the most discrepant indexes of 22 or more, a General Ability Index was calculated based on VCI and PRI alone and used as a measure of general intellect (53).
Adaptive abilities were assessed with the Adaptive Behavior Assessment System, Second Edition (ABAS-II) (54), which was administered to both parents/principal caregiver if parents were missing. It is a parent-report questionnaire which measures skills related to development, behavior, and cognitive abilities in 10 functioning areas, gathered in three main adaptive domains: conceptual (CAD), practical (PAD), social (SAD), and a comprehensive score, General Adaptive Composite (GAC), given by the sum of scaled scores from the functioning areas.
The Children’s Global Assessment Scale (C-GAS) (55) was used to assess global functioning.
2.3 Statistical analysis
Categorical variables are presented as number and percentage. Continuous variables are presented as mean and standard deviation (SD). In the section on the description of the cohort characteristics, association between variables was tested with Pearson’s or Fisher’s test, as appropriate. The Bonferroni correction for multiple comparisons was applied.
To test the 1st hypothesis, means of cognitive, adaptive abilities and general functioning scores were compared in the different diagnosis groups by a multivariate analysis of variance (MANOVA). Mean IQ, Wechsler scale indexes (VCI, PRI, WMI, PSI), adaptive behavior general composite score and scales (Communication, Daily living skills, Socialization) and C-GAS score were compared between the 3 diagnosis groups. Variance–covariance homogeneity assumption was tested with Box’s test and was not violated. Pillai’s trace was chosen to assess the significance of the model. Eta squares (η2) were reported as a measure of effect size of the model. Post-hoc analyses were performed using Fisher’s LSD test. Odds ratios (OR) with 95% confidence intervals were reported. SPSS generalized linear model for repeated measures was used to test differences between VCI, PRI, WMI and PSI within patients with the same mood disorder diagnosis. VCI, PRI, WMI and PSI were computed as repeated measures and the three mood diagnosis disorder groups were tested independently.
To test the 2nd hypothesis, linear regression modeling was used to test the effect of mood disorder diagnosis controlling for potential confounding effect of age, sex and comorbidities known to potentially affect cognitive functioning, adaptive abilities and general functioning. Among these, we tested the variables which were found to be significantly different among mood disorder diagnoses in the previous analyses as predictors. FSIQ and indexes (VCI, PRI, WMI and PSI) were tested as predicted variables in repeated analyses. Furthermore, mood disorder diagnosis FSIQ and indexes, sex and comorbidities (if found to be significantly different among mood disorder diagnoses in previous analyses), were tested as predictors and ABAS-II general composite score and subscales as predicted variables. Lastly, mood disorder diagnoses, FSIQ and indexes, ABAS-II general composite score and subscales age, sex, comorbidities (if significantly different among mood disorder diagnoses in the previous analyses), were tested as predictors of C-GAS score.
A p value of 0.05 or less was considered significative. Analyses were conducted with Microsoft Office 365 – Excel and IBM SPSS Statistics V26 software.
3 Results
3.1 Characteristics of the cohort
During the study period, data on 198 patients (85.9% females) were collected. The diagnosis was of MDD in 33.3% (number = 66), DMDD in 6.6% (number = 13) and DD-NOS in 60.1% (number = 119). UHR for psychosis was present in 22.7% of patients. Patients had a mean 0.62 active comorbidities (SD 0.67, range 0–3). Female prevalence was lower in DMDD (61.5%, p = 0.012). DMDD patients had higher rates of ADHD (15.4%), LD (23.1%) and CD (7.7%) than other mood disorder groups and lower rates of current (n = 0) or past anxiety disorders (23.2%) or eating disorders (n = 0). Difference in prevalence of comorbid eating disorder was not significative after applying Bonferroni correction for multiple comparisons.
3.2 Hypothesis 1: cognitive and adaptive profiles and functioning differ according to mood disorder diagnosis
For a complete description of the cohort, see Table 1. Cognitive evaluation was carried out with WISC-IV in 84.3% cases and WAIS in the remaining cases. FSIQ was interpretable in 91.4%.

Table 1. Description of the cohort.
DMDD was characterized by a mean FSIQ of 87.8, which was significantly lower than MDD (105.2) and DD-NOS (102.1).
VCI and PRI were significantly lower in DMDD than in MDD and DD-NOS. WMI was significantly higher in MDD than in DD-NOS and DMDD, while in DMDD it was not significantly lower than in DD-NOS. Significant differences in PSI were found on post-hoc analysis in all comparisons between group, and PSI in MDD was significantly higher than in DD-NOS and in DMDD. Additionally, PSI in DD-NOS was significantly higher than in DMDD.
With regard to within-group difference between indexes, WMI and PSI were significantly lower than VCI and PRI in all diagnosis groups (F = 18.6, p < 0.001, partial η2 = 0.47 in MDD group; F = 55.3, p < 0.001, partial η2 = 0.59 in DD-NOS group; F = 6.5, p = 0.01, partial η2 = 0.66 in DMDD group;). Pairwise comparisons of VCI vs. WMI, VCI vs. PSI, PRI vs. WMI, and PRI vs. PSI were significant with p ≤ 0.001 in MDD group and in DD-NOS group. In DD-NOS, VCI was also significantly higher than PRI (108.6 ± 14.1 vs. 105.5 ± 14.8, p = 0.023). In DMDD group, pairwise comparisons of VCI vs. WMI and VCI vs. PSI were significant with p = 0.001, pairwise comparison of PRI vs. WMI was significant with p = 0.002 and pairwise comparison of PRI vs. PSI was significant with p = 0.008.
With regard to adaptive abilities, patients with DMDD have lower mean General Adaptive Composite scores than MDD and DD-NOS; lower mean Conceptual Adaptive Domain scores than MDD and DD-NOS; lower mean Social Adaptive Domain scores than MDD and DD-NOS; and lower mean Practical Adaptive Domain scores than MDD and DD-NOS.
Global functioning measured with C-GAS was not significantly different among mood disorder diagnosis groups (p = 0.503).
For further details, please refer to Table 1.
3.3 Hypothesis 2: cognitive and adaptive profiles and functioning differ according to mood disorder diagnosis after controlling for comorbidities
We tested the effect of mood disorder diagnoses in predicting FSIQ and Wechsler scale indexes controlling for the effect of possible confounding variables which potentially influence cognitive indexes studied and significantly differ between groups of mood disorder diagnoses. In more detail, FSIQ and subsequently each index (VCI, PRI, WMI, and PSI) were set as predicted variables and mood disorder diagnosis, together with female sex, comorbid anxiety disorders, comorbid ADHD, comorbid LD and comorbid CD as predictors in five consecutive regression analyses. Results are shown in Table 2. A diagnosis of DMDD was a significant predictor of FSIQ, VCI, PRI, and PSI, correlating with lower scores even controlling for the effect of sex and comorbidities. However, comorbid LD was a significant predictor of FSIQ and of PRI, correlating with lower scores. PSI, in addition, was also significantly predicted by female sex and comorbid anxiety disorder, which were correlated with higher scores.
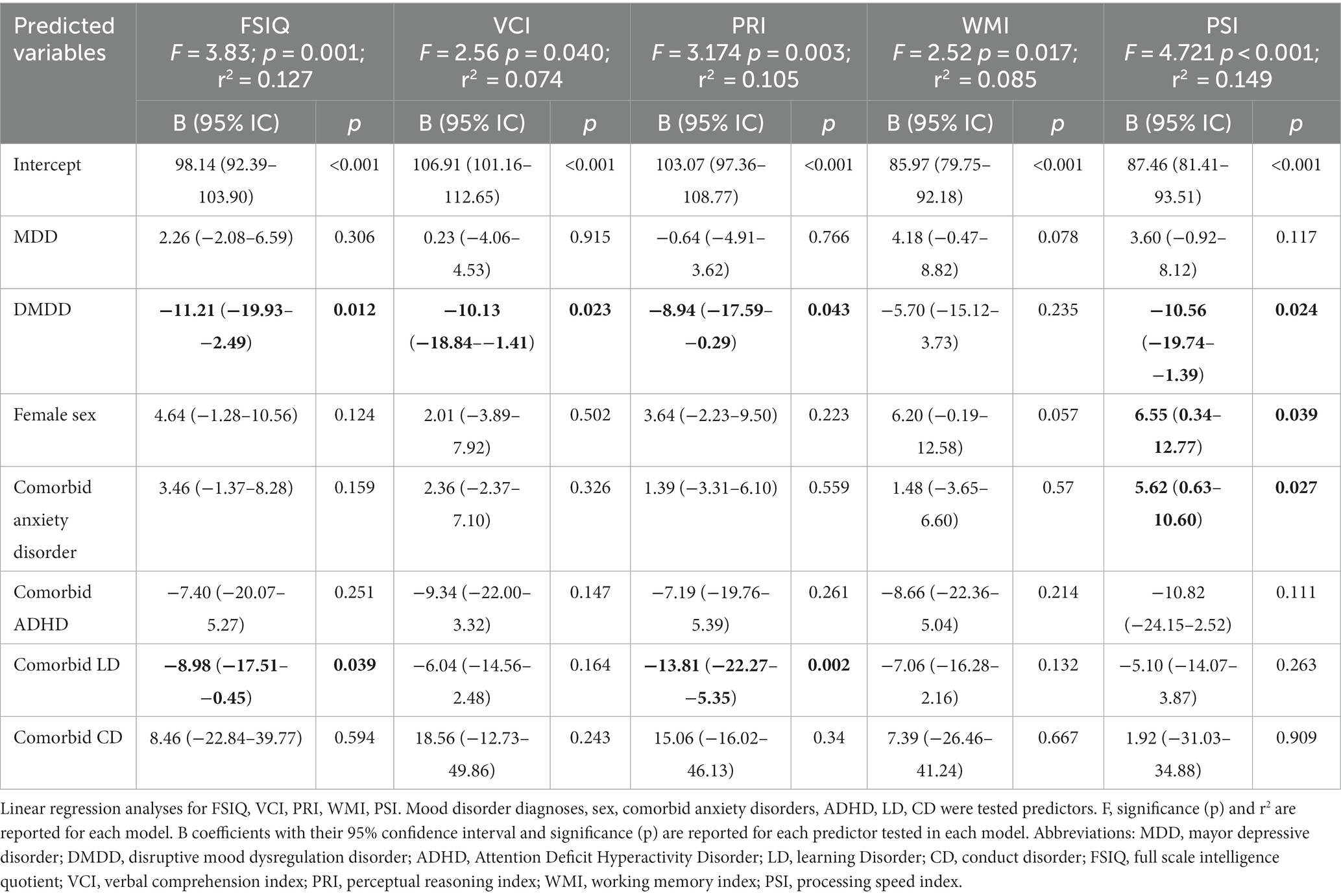
Table 2. Linear regression analyses for FSIQ, VCI, PRI, WMI, PSI.
Thereafter, we tested the effect of mood disorder diagnosis in predicting adaptive abilities scores, controlling for the effect of FSIQ and indexes, female sex, comorbid anxiety disorders, comorbid ADHD, comorbid LD and comorbid CD in four consecutive regression analyses. Results are shown in Table 3. DMDD diagnosis was a significant predictor of ABAS II GAC, VCI and ABAS II SAD, correlating with lower scores even controlling for the effect of IQ, sex and comorbidities. Furthermore, WMI was a significant predictor of ABAS II GAC, of ABAS II CAD, ABAS II SAD, of ABAS II PAD, with a positive correlation. The effect of comorbid ADHD was significant on ABAS II CAD, correlating with lower scores.
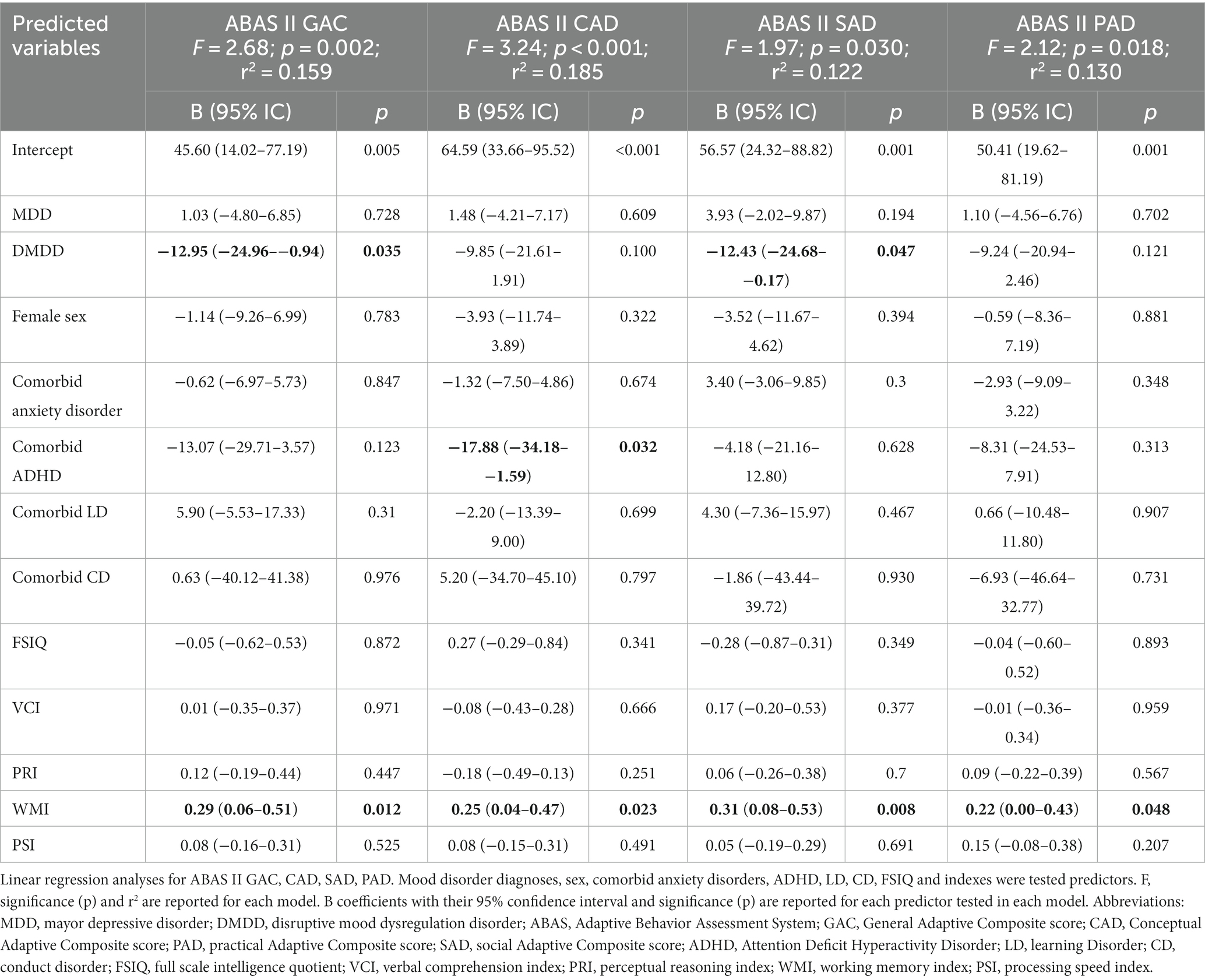
Table 3. Linear regression analyses for ABAS II GAC, CAD, SAD, PAD.
Lastly, we tested the effect of mood disorder diagnosis in predicting general functioning, controlling for the effect of adaptive abilities, FSIQ and indexes, female sex, comorbid anxiety disorders, comorbid ADHD, comorbid LD and comorbid CD in a regression analyses. Results are shown in Table 4. Specific mood disorder diagnoses were not significant predictors of functioning, while comorbid anxiety disorders were weakly associated with higher C-GAS scores.
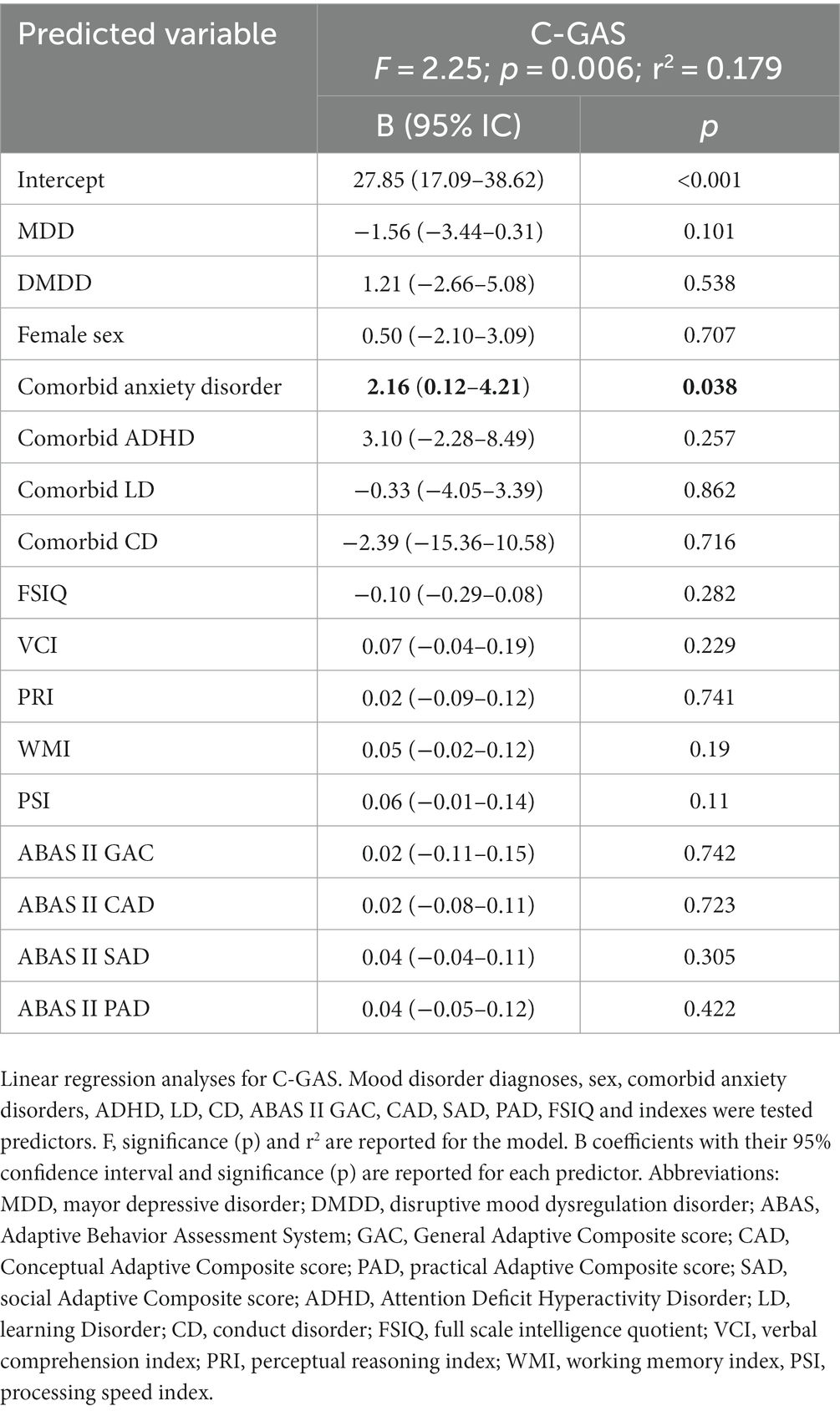
Table 4. Linear regression analyses for C-GAS.
4 Discussion
We analyzed a cohort of adolescents with depressive disorders to identify relevant differences in cognitive, adaptive profile and functioning between the different groups of mood disorder diagnoses. Participants were selected from an inpatient setting, where they were admitted for acute decompensation of current psychopathology. All participants were in an active phase of the psychiatric disorder and a degree of impairment was evident in all.
In patients with DMDD, general intelligence and adaptive abilities were significantly lower. Furthermore, patients with DMDD were characterized by a higher rate of neurodevelopmental comorbidities. In more detail, patients with DMDD had more comorbid ADHD and LD, as well as CD, and lower lifetime and present anxiety comorbidities. WMI and PSI were significantly lower than VCI and PRI in all patients, as a nonspecific signature of mood disorder.
In regression analyses, the effect of DMDD on lower IQ, VCI, PRI and PSI was significant; an effect of LD on IQ and PRI was significant too. The effect of DMDD on lower adaptive abilities was significant and more marked in the social adaptive domain, while ADHD had a significant effect on conceptual adaptive domain. Functioning was low on average in all groups, and not significantly affected by specific mood disorder diagnoses. It was slightly higher, however, in patients with anxiety comorbidities.
DMDD is a debated entity among depressive disorders, however our exploratory findings on cognition and adaptive impairment relative to psychopathological comorbidities, in the landscape of previous literature, may point toward its conceptualization as a distinct disorder, whose features cannot be exhaustively included in the mood disorder chapter. We contemplate a reconsideration of DMDD as a bridge entity between neurodevelopmental and mood disorders.
We assessed comorbidities systematically and analyzed their possible impact on cognition, adaptive abilities and functioning in regression analyses. This was particularly relevant for ADHD and LD, which are known to influence Wechsler scales examination scores. The effect of bidirectional interaction between neurodevelopmental and mood disorders on cognition is an under investigated issue, which is worth exploring in future studies. ADHD and LD affected cognitive profiles more than anxiety, depression, and behavior disorders in one study (41), while ADHD and depression showed specific and additive effects on PSI in another one (42). Our evidence indicates that a correlation of DMDD with lower cognitive and adaptive performances is a correlate of DMDD itself and not only explained by associated neurodevelopmental comorbidities. This is also consistent with the findings of Haller et al. (40), who recently described significant interactive effects between ADHD and DMDD in cognitive processing and a pivotal role for irritability in processing efficiency between conflict and non-conflict conditions. This is also consistent with the recent description of Benarous et al. (37) of DMDD as an admixture of mood and developmental disturbances which is not explained by its association with ADHD. Patients with DMDD in our study can be described as children with chronic impairing irritability, with a mild grade of cognitive impairment and frequent overlapping neurodevelopmental disorders, with remarkably lower social abilities. On this basis, we describe DMDD as a distinct entity, straddling neurodevelopmental and mood disorders.
DMDD in our cohort appears distinct from pediatric bipolar disorders (10, 56) since studies on high-risk cohorts for bipolar disorder found a premorbid social and cognitive functioning comparable to the general population and more internalizing comorbidities than neurodevelopmental disorders (16). It also appears distinct from ADHD for the grade and quality of impairment. Some authors argue that DMDD may be conceptualized as a subtype of ADHD characterized by temper and mood lability (16, 57). Our patients with DMDD, however, have an impairment which encompasses all domains of cognition and affects skills for relation with others, while an additive effect of ADHD on mood disorder is more apparent in conceptual domain. Both conceptual and social adaptive domains affect academic functioning, but social skills may be viewed as a more general requisite for becoming independent in the context of a community and developing identity in adolescence (58). Language and communication give access to self-regulatory strategies and provide alternatives to disruptive outbursts, a maladaptive coping strategy which is a hallmark of DMDD (59). Recent studies (60) have investigated a specific neuropsychologic background which may underlie development of DMDD, characterized by deficits in emotion recognition, which may limit social adaptation and self-regulation. Neurobiology models of dysfunction of reward circuitry and learning in severe chronic irritability support this view. Brotman et al. (56) described a translational model, in which subjects with severe irritability are characterized by abnormal threshold and reactivity to frustration, with diffuse alterations in prefrontal and anterior cingulate cortex, striatum and amygdala. As noted by Benarous et al. (61), failure of children with DMDD to develop effective emotional regulation skills is rooted in early development and involves impairments in instrumental learning and in performing and learning from parent–child interactions.
These considerations are also interesting in light of recent studies on “emotional dysregulation” construct, conceptualized as a distinct neurodevelopmental, early-onset disorder (62). DMDD may be viewed as a neurodevelopmental early-onset disorder, where regulation of emotions is particularly affected on a cognitive deficiency basis, which reinforces social maladaptation over time. It would be worth exploring in further studies the possible construct overlap of emotional dysregulation, studied with specifically designed instruments, such as RIPoSt-Y (62), with DMDD and ADHD.
Our patients with DMDD had higher rates of ADHD, LD and CD, which is consistent with the studies of Benarous et al. (20, 37), but also lower rates of anxiety disorders. This may be due to the fact that we observed young patients, who are in the early phase of their psychopathological trajectory, a phase in which anxiety comorbidities may be less prevalent, while it is known that anxiety is relevant in longitudinal follow-up studies of chronically irritable children (63).
We also analyzed MDD, DD-NOS and DMDD to find differences in cognitive performance in different domains within each group to identify distinctive profiles. Impairment in working memory and processing speed appeared as a non-specific correlate of current mood disorder across all diagnoses. Literature on adults (28, 64, 65) and more sparse literature on adolescents (34) supports our finding of WMI and PSI being lower than VCI and PRI in mood disorders. WMI and PSI are critical during development for the acquisition of new learning and actual application of crystallized knowledge. WMI significantly correlated with adaptive abilities, accordingly. Of note, DD-NOS in our cohort showed a grade of cognitive and adaptive impairment comparable with MDD. A reflection on this significant impairment in depressed adolescents not meeting MDD criteria is needed, and we remark that these pictures may be impairing during the age of development and must not be overlooked. However, for a correct interpretation of this finding, we must comment on the intrinsic limit posed by the heterogeneity of DD-NOS diagnosis, characterized by definition by depressive symptoms which do not meet severity and duration criteria for MDD. DD-NOS are also often characterized by emotional dysregulation and mood instability which do not meet criteria for a bipolar disorder or for a DMDD diagnosis. A significant lowering of WMI in this group may be implied by further psychopathology which could have been observed only in a longitudinal study. Of note, our inpatients with DD-NOS also frequently met criteria for UHR for psychosis (28%).
PSI was the most discriminant index between groups. It was higher in females, consistently with literature (66), and since our sample is made predominantly of female patients, interpretation of this finding has some limitations. PSI links causally to other elements of intelligence (67, 68), permitting more effective use of WM and enhancing fluid reasoning (69, 70). Its impairment has been observed in euthymic adults with a previous diagnosis of MDD (64) and first-degree relatives of patients with mood disorders (29). Our results, in the wake of the cited literature, highlight its relevance in early-onset psychopathology. PRI and VCI seem to be relatively preserved in MDD and DD-NOS, with mean scores around 100. A lower PRI, however, is a correlate of LD, consistently with previous literature on visual–spatial and motion perception impairment in developmental dyslexia (71).
General functioning in our study was low on average in all groups, due to the inpatient setting of our study, where patients are admitted for acute decompensation of their psychopathology. Previous studies report mixed findings on functioning. A study on depressive disorders did not find differences in global functioning but reported more school and peer-relationship difficulties in DMDD compared to MDD (20). A study on inpatients found higher discharge Global Assessment of Functioning (GAF) scores in patients with DMDD (72), while another found lower GAF scores on admission and discharge (57).
A strength of our study is providing data on cognitive and adaptive profile of DMDD, whereas literature is limited. The evaluation procedure was standardized, providing a synoptic overview on cognition, adaptation and functioning, and all patients were evaluated in an early and acute phase of their psychopathological trajectory. There are, however, considerable limitations. Firstly, the study was exploratory, DMDD patients were a minority, and the sample size was underpowered. Chronic irritability is more often managed in outpatient units, limiting the number of our observations of DMDD to patients needing prompt start of a pharmacological treatment. Furthermore, due to the cross-sectional design of the study, some patients may have been provisionally classified as DD-NOS for not meeting the criteria for a diagnosis of another mood disorder (such as Persistent depressive disorder, or bipolar and related disorders, or even DMDD) at first clinical observation. Excessive prevalence of females in our cohort is consistent with differential incidence of mood disorders between sexes but limits the detection of sex differences in the outcomes studied. Finally, our cohort is made of inpatients, which are all characterized by higher severity of current psychopathology. These limitations are worth addressing in specifically designed perspective studies.
Data availability statement
The datasets presented in this article are not readily available because of the nature of the research, due to ethical reasons. Further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by Ospedale Pediatrico Bambino Gesù. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
Author contributions
MA: Conceptualization, Formal analysis, Writing – original draft, Writing – review & editing. MCP: Data curation, Methodology, Writing – review & editing. RA: Conceptualization, Investigation, Methodology, Writing – review & editing. ML: Data curation, Investigation, Writing – review & editing. MP: Methodology, Supervision, Writing – review & editing. SV: Conceptualization, Investigation, Supervision, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported by the Italian Ministry of Health with Current Research funds. The supporters had no role in the design, analysis, interpretation, or publication of this study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Racine, N, McArthur, BA, Cooke, JE, Eirich, R, Zhu, J, and Madigan, S. Global prevalence of depressive and anxiety symptoms in children and adolescents during COVID-19. JAMA Pediatr. (2021) 175:1142–50. doi: 10.1001/jamapediatrics.2021.2482
2. Apicella, M, Serra, G, Trasolini, M, Andracchio, E, Chieppa, F, Averna, R, et al. Urgent psychiatric consultations for suicide attempt and suicidal ideation before and after the COVID-19 pandemic in an Italian pediatric emergency setting. Front Psych. (2023) 14:14. doi: 10.3389/fpsyt.2023.1135218
3. Thapar, A, Collishaw, S, Pine, DS, and Thapar, AK. Depression in adolescence. Lancet. (2012) 379:1056–67. doi: 10.1016/S0140-6736(11)60871-4
4. Van Meter, A, Moreira, ALR, and Youngstrom, E. Updated Meta-analysis of epidemiologic studies of pediatric bipolar disorder. J Clin Psychiatry. (2019) 80:21938. doi: 10.4088/JCP.18r12180
5. Leibenluft, E, and Stoddard, J. The developmental psychopathology of irritability. Dev Psychopathol. (2013) 25:1473–87. doi: 10.1017/S0954579413000722
6. DSM-5: American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 5th ed. US: APA (2013).
7. Bruno, A, Celebre, L, Torre, G, Pandolfo, G, Mento, C, Cedro, C, et al. Focus on disruptive mood dysregulation disorder: a review of the literature. Psychiatry Res. (2019) 279:323–30. doi: 10.1016/j.psychres.2019.05.043
8. Serra, G, Uchida, M, Battaglia, C, Casini, MP, De Chiara, L, Biederman, J, et al. Pediatric mania: the controversy between Euphoria and irritability. Curr Neuropharmacol. (2017) 15:386–93. doi: 10.2174/1570159X14666160607100403
9. Leibenluft, E, Charney, DS, Towbin, KE, Bhangoo, RK, and Pine, DS. Defining clinical phenotypes of juvenile mania. Am J Psychiatry. (2003) 160:430–7. doi: 10.1176/appi.ajp.160.3.430
10. Stringaris, A, Cohen, P, Pine, DS, and Leibenluft, E. Adult outcomes of youth irritability: a 20-year prospective community-based study. Am J Psychiatry. (2009) 166:1048–54. doi: 10.1176/appi.ajp.2009.08121849
11. Brotman, MA, Schmajuk, M, Rich, BA, Dickstein, DP, Guyer, AE, Costello, EJ, et al. Prevalence, clinical correlates, and longitudinal course of severe mood dysregulation in children. Biol Psychiatry. (2006) 60:991–7. doi: 10.1016/j.biopsych.2006.08.042
12. Brotman, MA, Kassem, L, Reising, MM, Guyer, AE, Dickstein, DP, Rich, BA, et al. Parental diagnoses in youth with narrow phenotype bipolar disorder or severe mood dysregulation. Am J Psychiatry. (2007) 164:1238–41. doi: 10.1176/appi.ajp.2007.06101619
13. Mitchell, RHB, Timmins, V, Collins, J, Scavone, A, Iskric, A, and Goldstein, BI. Prevalence and correlates of disruptive mood dysregulation disorder among adolescents with bipolar disorder. J Child Adolesc Psychopharmacol. (2016) 26:147–53. doi: 10.1089/cap.2015.0063
14. Mayes, SD, Waxmonsky, JD, Calhoun, SL, and Bixler, EO. Disruptive mood dysregulation disorder symptoms and association with oppositional defiant and other disorders in a general population child sample. J Child Adolesc Psychopharmacol. (2016) 26:101–6. doi: 10.1089/cap.2015.0074
15. Mayes, SD, Waxmonsky, J, Calhoun, SL, Kokotovich, C, Mathiowetz, C, and Baweja, R. Disruptive mood dysregulation disorder (DMDD) symptoms in children with autism, ADHD, and neurotypical development and impact of co-occurring ODD, depression, and anxiety. Res Autism Spectr Disord. (2015) 18:64–72. doi: 10.1016/j.rasd.2015.07.003
16. Duffy, A, Carlson, G, Dubicka, B, and MHJ, H. Pre-pubertal bipolar disorder: origins and current status of the controversy. Int J Bipolar Disor. (2020) 8:18. doi: 10.1186/s40345-020-00185-2
17. Baweja, R, Mayes, SD, Hameed, U, and Waxmonsky, JG. Disruptive mood dysregulation disorder: current insights. Neuropsychiatr Dis Treat. (2016) 12:2115–24. doi: 10.2147/NDT.S100312
18. Roy, AK, Lopes, V, and Klein, RG. Disruptive mood dysregulation disorder: a new diagnostic approach to chronic irritability in youth. Am J Psychiatry. (2014) 171:918–24. doi: 10.1176/appi.ajp.2014.13101301
19. Hamshere, ML, Langley, K, Martin, J, Agha, SS, Stergiakouli, E, Anney, RJ, et al. High loading of polygenic risk for ADHD in children with comorbid aggression. Am J Psychiatry. (2013) 170:909–16. doi: 10.1176/appi.ajp.2013.12081129
20. Benarous, X, Renaud, J, Breton, JJ, Cohen, D, Labelle, R, and Guilé, JM. Are youths with disruptive mood dysregulation disorder different from youths with major depressive disorder or persistent depressive disorder? J Affect Disord. (2020) 265:207–15. doi: 10.1016/j.jad.2020.01.020
21. Bell, E, Bryant, R, Boyce, P, Porter, R, and Malhi, G. Irritability through research domain criteria: an opportunity for transdiagnostic conceptualisation. BJPsych Open. (2021) 7:E36. doi: 10.1192/bjo.2020.168
22. Vicent-Gil, M, Portella, MJ, Serra-Blasco, M, Navarra-Ventura, G, Crivillés, S, Aguilar, E, et al. Dealing with heterogeneity of cognitive dysfunction in acute depression: a clustering approach. Psychol Med. (2021) 51:2886–94. doi: 10.1017/S0033291720001567
23. Dunn, RT, Kimbrell, TA, Ketter, TA, Frye, MA, Willis, MW, Luckenbaugh, DA, et al. Principal components of the Beck depression inventory and regional cerebral metabolism in unipolar and bipolar depression. Biol Psychiatry. (2002) 51:387–99. doi: 10.1016/s0006-3223(01)01244-6
24. Rossi, A, Daneluzzo, E, Arduini, L, Di Domenico, M, Stratta, P, and Petruzzi, C. Cognitive symptoms of mania in pure and mixed episodes evaluated with the positive and negative syndrome scale. Eur Arch Psychiatry Clin Neurosci. (2000) 250:254–6. doi: 10.1007/s004060070015
25. Roiser, JP, Rubinsztein, JS, and Sahakian, BJ. Neuropsychology of affective disorders. Psychiatry. (2009) 8:91–6. doi: 10.1016/j.mppsy.2008.11.007
26. Weiser, M, Reichenberg, A, Rabinowitz, J, Knobler, HY, Lubin, G, Yazvitzky, R, et al. Cognitive performance of male adolescents is lower than controls across psychiatric disorders: a population-based study. Acta Psychiatr Scand. (2004) 110:471–5. doi: 10.1111/j.1600-0447.2004.00385.x
27. Mortensen, EL, Sørensen, HJ, Jensen, HH, Reinisch, JM, and Mednick, SA. IQ and mental disorder in young men. Br J Psychiatry. (2005) 187:407–15. doi: 10.1192/bjp.187.5.407
28. Matsuo, J, Hori, H, Ishida, I, Hiraishi, M, Ota, M, Hidese, S, et al. Performance on the Wechsler adult intelligence scale (WAIS) in Japanese patients with bipolar and major depressive disorders in euthymic and depressed states. Psychiatry Clin Neurosci. (2021) 75:128–37. doi: 10.1111/pcn.13191
29. Bo, Q, Dong, F, Li, X, Li, F, Li, P, Yu, H, et al. Comparison of cognitive performance in bipolar disorder, major depressive disorder, unaffected first-degree relatives, and healthy controls. Psychiatry Clin Neurosci. (2019) 73:70–6. doi: 10.1111/pcn.12797
30. Ozdel, O, Karadag, F, Atesci, FC, Oguzhanoglu, NK, and Cabuk, T. Cognitive functions in euthymic patients with bipolar disorder. Ann Saudi Med. (2007) 27:273–8. doi: 10.5144/0256-4947.2007.273
31. MacCabe, JH, Lambe, MP, Cnattingius, S, Torrång, A, Björk, C, Sham, PC, et al. Scholastic achievement at age 16 and risk of schizophrenia and other psychoses: a national cohort study. Psychol Med. (2007) 38:1133–40. doi: 10.1017/S0033291707002048
32. Zammit, S, Allebeck, P, David, AS, Dalman, C, Hemmingsson, T, Lundberg, I, et al. A longitudinal study of premorbid IQ score and risk of developing schizophrenia, bipolar disorder, severe depression and other non-affective psychoses. Arch Gen Psychiatry. (2004) 61:354–60. doi: 10.1001/archpsyc.61.4.354
33. Glaser, B, Gunnell, D, Timpson, NJ, Joinson, C, Zammit, S, Smith, GD, et al. Age- and puberty-dependent association between IQ score in early childhood and depressive symptoms in adolescence. Psychol Med. (2011) 41:333–43. doi: 10.1017/S0033291710000814
34. Favre, T, Hughes, C, Emslie, G, Stavinoha, P, Kennard, B, and Carmody, T. Executive functioning in children and adolescents with Major depressive disorder. Child Neuropsychol. (2009) 15:85–98. doi: 10.1080/09297040802577311
35. Copeland, WE, Angold, A, Costello, EJ, and Egger, H. Prevalence, comorbidity, and correlates of DSM-5 proposed disruptive mood dysregulation disorder. Am J Psychiatry. (2013) 170:173–9. doi: 10.1176/appi.ajp.2012.12010132
36. Althoff, RR, Crehan, ET, He, JP, Burstein, M, Hudziak, JJ, and Merikangas, KR. Disruptive mood dysregulation disorder at ages 13-18: results from the National Comorbidity Survey-Adolescent Supplement. J Child Adolesc Psychopharmacol. (2016) 26:107–13. doi: 10.1089/cap.2015.0038
37. Benarous, X, Iancu, C, Guilé, JM, Consoli, A, and Cohen, D. Missing the forest for the trees? A high rate of motor and language impairments in disruptive mood dysregulation disorder in a chart review of inpatient adolescents. Eur Child Adolesc Psychiatry. (2020) 30:1579–90. doi: 10.1007/s00787-020-01636-y
38. Adleman, NE, Fromm, SJ, Razdan, V, Kayser, R, Dickstein, DP, Brotman, MA, et al. Cross-sectional and longitudinal abnormalities in brain structure in children with severe mood dysregulation or bipolar disorder. J Child Psychol Psychiatry. (2012) 53:1149–56. doi: 10.1111/j.1469-7610.2012.02568.x
39. Rau, G, Blair, KS, Berghorst, L, Knopf, L, Skup, M, Luckenbaugh, DA, et al. Processing of differentially valued rewards and punishments in youths with bipolar disorder or severe mood dysregulation. J Child Adolesc Psychopharmacol. (2008) 18:185–96. doi: 10.1089/cap.2007.0053
40. Haller, SP, Stoddard, J, Pagliaccio, D, Bui, H, MacGillivray, C, Jones, M, et al. Computational modeling of attentional impairments in disruptive mood dysregulation and attention-deficit/hyperactivity disorder. J Am Acad Child Adolesc Psychiatry. (2021) 60:637–45. doi: 10.1016/j.jaac.2020.08.468
41. Mayes, SD, and Calhoun, SL. Similarities and differences in Wechsler intelligence scale for children--third edition (WISC-III) profiles: support for subtest analysis in clinical referrals. Clin Neuropsychol. (2004) 18:559–72. doi: 10.1080/13854040490888530
42. Larochette, AC, Harrison, AG, Rosenblum, Y, and Bowie, CR. Additive neurocognitive deficits in adults with attention-deficit/hyperactivity disorder and depressive symptoms. Arch Clin Neuropsychol. (2011) 26:385–95. doi: 10.1093/arclin/acr033
43. Alexander, RM, and Reynolds, MR. Intelligence and adaptive behavior: a Meta-analysis. Sch Psychol Rev. (2020) 49:85–110. doi: 10.1080/2372966X.2020.1717374
44. Papazoglou, A, Jacobson, LP, and Zabel, TA. More than intelligence: distinct cognitive/behavioral clusters linked to adaptive dysfunction in children. J Int Neuropsychol Soc. (2013) 19:189–97.
45. Rush, SC, Major-Sanabria, M, and Corcoran, S. Chapter 16 - using the ABAS-II with adolescents and young adults In: T Oakland and PL Harrison, editors. ScienceDirect. San Diego: Academic press (2008). 313–30.
46. Bellini, J. Mental retardation: definition, classification, and Systems of Supports. Ment Retard. (2003) 41:135–40. doi: 10.1352/0047-6765(2003)041<0135:BR>2.0.CO;2
47. Kaufman, J, and Al, E. K-SADS-PL DSM-5®: intervista diagnostica per la valutazione dei disturbi psicopatologici in bambini e adolescenti. Trento: Erickson, Cop (2019).
48. McGlashan, TH, Miller, TJ, Woods, SW, Hoffman, RE, and Davidson, L. Instrument for the assessment of prodromal symptoms and states. Early Interven Psychotic Disor. (2001) 91:135–49. doi: 10.1007/978-94-010-0892-1_7
49. Miller, TJ, McGlashan, TH, Rosen, JL, Cadenhead, K, Cannon, T, Ventura, J, et al. Prodromal assessment with the structured interview for prodromal syndromes and the scale of prodromal symptoms: predictive validity, interrater reliability, and training to reliability. Schizophr Bull. (2003) 29:703–15. doi: 10.1093/oxfordjournals.schbul.a007040
50. Fusar-Poli, P, Borgwardt, S, Bechdolf, A, Addington, J, Riecher-Rössler, A, Schultze-Lutter, F, et al. The psychosis high-risk state: a comprehensive state-of-the-art review. JAMA Psychiatry. (2013) 70:107–20. doi: 10.1001/jamapsychiatry.2013.269
51. Orsini, A, Pezzuti, L, and Picone, L. Wechsler intelligence scale for children IV Edizione Italiana. Florence, Italy: Organizzazioni Speciali (2012).
52. Orsini, A, and Pezzuti, L. WAIS-IV: Wechsler adult intelligence scale, Edizione Italiana. Florence, Italy: Organizzazioni Speciali (2013).
53. Prifitera, A, Saklofski, DH, and Weiss, L. WISC-IV clinical use and interpretation: Scientist-practitioner perspectives. Burlington, MA: Elsevier Academic Press (2005).
54. Oakland, T. Adaptive behavior assessment system – second edition In: JS Kreutzer, J DeLuca, and B Caplan, editors. Encyclopedia of clinical neuropsychology. New York, NY: Springer (2011)
55. Shaffer, D, Gould, MS, Brasic, J, Ambrosini, P, Fisher, P, Bird, H, et al. A children’s global assessment scale (CGAS). Arch Gen Psychiatry. (1983) 40:1228–31. doi: 10.1001/archpsyc.1983.01790100074010
56. Brotman, MA, Kircanski, K, Stringaris, A, Pine, DS, and Leibenluft, E. Irritability in youths: a translational model. Am J Psychiatry. (2017) 174:520–32. doi: 10.1176/appi.ajp.2016.16070839
57. Margulies, DM, Weintraub, S, Basile, J, Grover, PJ, and Carlson, GA. Will disruptive mood dysregulation disorder reduce false diagnosis of bipolar disorder in children? Bipolar Disord. (2012) 14:488–96. doi: 10.1111/j.1399-5618.2012.01029.x
58. Meyers, E, DeSerisy, M, and Roy, AK. Disruptive mood dysregulation disorder (DMDD): an RDoC perspective. J Affect Disord. (2017) 216:117–22. doi: 10.1016/j.jad.2016.08.007
59. Carlson, GA, Potegal, M, Margulies, D, Gutkovich, Z, and Basile, J. Rages—what are they and who has them? J Child Adolesc Psychopharmacol. (2009) 19:281–8. doi: 10.1089/cap.2008.0108
60. Vidal-Ribas, P, Brotman, MA, Salum, GA, Kaiser, A, Meffert, L, Pine, DS, et al. Deficits in emotion recognition are associated with depressive symptoms in youth with disruptive mood dysregulation disorder depress. Anxiety. (2018) 35:1207–17. doi: 10.1002/da.22810
61. Benarous, X, Cohen, D, Ferrafiat, V, and Guilé, JM. Navigating in troubled waters: the developmental roots of disruptive mood dysregulation disorder. J Am Acad Child Adolesc Psychiatry. (2021) 60:320–1. doi: 10.1016/j.jaac.2020.08.469
62. Sesso, G, Milone, A, Drago, F, Viglione, V, Berloffa, S, Boldrini, S, et al. A novel multidimensional questionnaire for the assessment of emotional dysregulation in adolescents: reactivity, intensity, polarity and stability questionnaire–youth version (RIPoSt–Y). J Affect Disord. (2021) 291:359–67. doi: 10.1016/j.jad.2021.05.037
63. Vidal-Ribas, P, Brotman, MA, Valdivieso, I, Leibenluft, E, and Stringaris, A. The status of irritability in psychiatry: a conceptual and quantitative review. J Am Acad Child Adolesc Psychiatry. (2016) 55:556–70. doi: 10.1016/j.jaac.2016.04.014
64. Grant, MM, Thase, ME, and Sweeney, JA. Cognitive disturbance in outpatient depressed younger adults: evidence of modest impairment. Biol Psychiatry. (2001) 50:35–43. doi: 10.1016/s0006-3223(00)01072-6
65. Keilp, JG, Sackeim, HA, Brodsky, BS, Oquendo, MA, Malone, KM, and Mann, JJ. Neuropsychological dysfunction in depressed suicide attempters. Am J Psychiatry. (2001) 158:735–41. doi: 10.1176/appi.ajp.158.5.735
66. Roivainen, E, Suokas, F, and Saari, A. An examination of factors that may contribute to gender differences in psychomotor processing speed. BMC Psychol. (2021) 9:190. doi: 10.1186/s40359-021-00698-0
67. Kail, R. Speed of information processing: developmental change and links to intelligence. J Sch Psychol. (2000) 38:51–61. doi: 10.1016/S0022-4405(99)00036-9
68. Fry, AF, and Hale, S. Processing speed, working memory, and fluid intelligence: evidence for a developmental Cascade. Psychol Sci. (1996) 7:237–41. doi: 10.1111/j.1467-9280.1996.tb00366.x
69. Hitch, GJ, Towse, JN, and Hutton, U. What limits children's working memory span? Theoretical accounts and applications for scholastic development. J Exp Psychol Gen. (2001) 130:184–98. doi: 10.1037//0096-3445.130.2.184
70. Anderson, M, Nettelbeck, T, and Barlow, J. Reaction time measures of speed of processing: speed of response selection increases with age but speed of stimulus categorization does not. Br J Dev Psychol. (1997) 15:145–57. doi: 10.1111/j.2044-835X.1997.tb00731.x
71. Menghini, D, Finzi, A, Benassi, M, Bolzani, R, Facoetti, A, Giovagnoli, S, et al. Different underlying neurocognitive deficits in developmental dyslexia: a comparative study. Neuropsychologia. (2010) 48:863–72. doi: 10.1016/j.neuropsychologia.2009.11.003
Keywords: disruptive mood dysregulation disorder, depression, adolescent, neurodevelopment, irritability, adaptive abilities, intelligence, neuropsychology
Citation: Apicella M, Pisa MC, Averna R, Labonia M, Pontillo M and Vicari S (2023) Neurocognitive and adaptive phenotypes in adolescent inpatients with mood disorders: an exploratory study on disruptive mood dysregulation disorder in the framework of depressive disorders. Front. Psychiatry. 14:1253589. doi: 10.3389/fpsyt.2023.1253589
Edited by:
Xavier Benarous, Hôpital Armand Trousseau, APHP. Sorbonne-Université, FranceReviewed by:
Vilas Sawrikar, University of Edinburgh, United KingdomGonca Özyurt, Izmir Katip Celebi University, Türkiye
Jean Marc Guile, University of Picardie Jules Verne, France
Copyright © 2023 Apicella, Pisa, Averna, Labonia, Pontillo and Vicari. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Massimo Apicella, massimo.apicella@opbg.net