 Christian Theisen1*
Christian Theisen1* Marlene Rosen2Eva Meisenzahl1
Marlene Rosen2Eva Meisenzahl1 Nikolaos Koutsouleris3,4,5Theresa Lichtenstein2
Nikolaos Koutsouleris3,4,5Theresa Lichtenstein2 Stephan Ruhrmann2
Stephan Ruhrmann2 Joseph Kambeitz2,6
Joseph Kambeitz2,6 Lana Kambeitz-Ilankovic2
Lana Kambeitz-Ilankovic2 Anita Riecher-Rössler7
Anita Riecher-Rössler7 Katharine Chisholm8,9
Katharine Chisholm8,9 Rachel Upthegrove8
Rachel Upthegrove8 Linda A. Antonucci10
Linda A. Antonucci10 Alessandro Bertolino10
Alessandro Bertolino10 Alessandro Pigoni11,12
Alessandro Pigoni11,12 Raimo K. R. Salokangas13
Raimo K. R. Salokangas13 Christos Pantelis14
Christos Pantelis14 Stephen J. Wood8,15,16Rebekka Lencer17,18
Stephen J. Wood8,15,16Rebekka Lencer17,18 Peter Falkai3,4
Peter Falkai3,4 Jarmo Hietala13
Jarmo Hietala13 Paolo Brambilla11,19
Paolo Brambilla11,19 André Schmidt20
André Schmidt20 Christina Andreou18
Christina Andreou18 Stefan Borgwardt18
Stefan Borgwardt18 Naweed Osman1
Naweed Osman1 Frauke Schultze-Lutter1,21,22 for the PRONIA Consortium
Frauke Schultze-Lutter1,21,22 for the PRONIA Consortium- 1Department of Psychiatry and Psychotherapy, Medical Faculty, Heinrich-Heine University, Düsseldorf, Germany
- 2Department of Psychiatry and Psychotherapy, Faculty of Medicine and University Hospital Cologne, University of Cologne, Cologne, Germany
- 3Department of Psychiatry and Psychotherapy, Ludwig-Maximilian-University, Munich, Germany
- 4Max-Planck-Institute of Psychiatry, Munich, Germany
- 5Institute of Psychiatry, Psychology and Neuroscience, King's College London, London, United Kingdom
- 6Research Center Jülich, Institute for Cognitive Neuroscience (INM-3), Jülich, Germany
- 7Medical Faculty, University of Basel, Basel, Switzerland
- 8Institute for Mental Health, University of Birmingham, Birmingham, United Kingdom
- 9Department of Psychology, Aston University, Birmingham, United Kingdom
- 10Department of Basic Medical Science, Neuroscience, and Sense Organs, University of Bari Aldo Moro, Bari, Italy
- 11Department of Neurosciences and Mental Health, Fondazione IRCCS Ca' Granda Ospedale Maggiore Policlinico, Milan, Italy
- 12MoMiLab Research Unit, IMT School for Advanced Studies Lucca, Lucca, Italy
- 13Department of Psychiatry, Medical Faculty, University of Turku, Turku, Finland
- 14Melbourne Neuropsychiatry Centre, University of Melbourne, Melbourne, VIC, Australia
- 15Orygen, The National Centre of Excellence for Youth Mental Health, Melbourne, VIC, Australia
- 16Centre for Youth Mental Health, University of Melbourne, Melbourne, VIC, Australia
- 17Department of Psychiatry and Psychotherapy, Otto Creutzfeldt Center for Cognitive and Behavioral Neuroscience, University of Muenster, Muenster, Germany
- 18Department of Psychiatry and Psychotherapy, University of Lübeck, Lübeck, Germany
- 19Department of Pathophysiology and Mental Health, University of Milan, Milan, Italy
- 20Department of Psychiatry, University of Basel, Basel, Switzerland
- 21Department of Psychology, Faculty of Psychology, Airlangga University, Surabaya, Indonesia
- 22University Hospital of Child and Adolescent Psychiatry and Psychotherapy, University of Bern, Bern, Switzerland
Introduction: The Attenuated Psychosis Symptoms (APS) syndrome mostly represents the ultra-high-risk state of psychosis but, as does the Brief Intermittent Psychotic Symptoms (BIPS) syndrome, shows a large variance in conversion rates. This may be due to the heterogeneity of APS/BIPS that may be related to the effects of culture, sex, age, and other psychiatric morbidities. Thus, we investigated the different thematic contents of APS and their association with sex, age, country, religion, comorbidity, and functioning to gain a better understanding of the psychosis-risk syndrome.
Method: A sample of 232 clinical high-risk subjects according to the ultra-high risk and basic symptom criteria was recruited as part of a European study conducted in Germany, Italy, Switzerland, and Finland. Case vignettes, originally used for supervision of inclusion criteria, were investigated for APS/BIPS contents, which were compared for sex, age, country, religion, functioning, and comorbidities using chi-squared tests and regression analyses.
Result: We extracted 109 different contents, mainly of APS (96.8%): 63 delusional, 29 hallucinatory, and 17 speech-disorganized contents. Only 20 contents (18.3%) were present in at least 5% of the sample, with paranoid and referential ideas being the most frequent. Thirty-one (28.5%) contents, in particular, bizarre ideas and perceptual abnormalities, demonstrated an association with age, country, comorbidity, or functioning, with regression models of country and obsessive-compulsive disorders explaining most of the variance: 55.8 and 38.3%, respectively. Contents did not differ between religious groups.
Conclusion: Psychosis-risk patients report a wide range of different contents of APS/BIPS, underlining the psychopathological heterogeneity of this group but also revealing a potential core set of contents. Compared to earlier reports on North-American samples, our maximum prevalence rates of contents were considerably lower; this likely being related to a stricter rating of APS/BIPS and cultural influences, in particular, higher schizotypy reported in North-America. The various associations of some APS/BIPS contents with country, age, comorbidities, and functioning might moderate their clinical severity and, consequently, the related risk for psychosis and/or persistent functional disability.
1. Introduction
Psychotic disorders are associated with high cost and burden (1–3) and lead to a reduced life expectancy of almost 12 years (4). Only 13.5% of all schizophrenia patients met the criteria for recovery despite advances in treatment (5). Thus, there is an urgent need for prevention (6). Because the first episode of psychotic disorders is mostly preceded by a prodromal phase of several years on average during which functional deficits already develop, an indicated prevention targeting help-seeking persons with the first signs of the emerging disorder has been considered most feasible (7). To identify persons with an increased risk of going on to develop a first psychotic episode among the help-seekers, clinical high-risk criteria (CHR) were developed and validated within the past three decades (7). Thereby, two complementary approaches were followed: the Ultra-High-Risk (UHR) and the basic symptom criteria (8) (note: CHR is used as an umbrella term when referring to both the UHR and the basic symptom approach). UHR criteria consist of the Attenuated Psychotic Symptoms (APS) syndrome, the Brief Intermittent Psychotic Symptoms (BIPS) syndrome, and the Genetic Risk and Functional Deterioration (GRFD) syndrome (9). Basic symptom criteria comprise the COGnitive-PERceptive basic symptoms (COPER) and the COGnitive DISturbance (COGDIS) (10). Of these five single criteria, the APS and BIPS syndromes and COGDIS were recommended for CHR detection (8).
On average, 85% of persons recruited into UHR samples meet the APS syndrome (11) and showed significant heterogeneity in conversion rates (8, 11). Among others, this may be due to the heterogeneity of APS, which integrate a wide range of different symptoms (12), different recruitment strategies and, relatedly, epidemiological filters (13), cultural effects (14, 15), childhood adversities and trauma (16), as well as effects of age or sex on both clinical significance and psychosis-predictive value of APS (17–20). APS/BIPS is identified in semi-structured interviews that rate APS/BIPS syndromally (21). In doing so, the various unusual thought contents, perceptual abnormalities, and types of conceptual disorganization that constitute APS/BIPS are generally assessed in separate aggregated items that distinguish unusual thought contents either by their bizarreness or by their general content, i.e., paranoid, grandiose, or other ideas (22). Even without considering the frequency of the individual symptoms or APS/BIPS contents, which are summarized in the positive items of UHR assessments, severity and prevalence rates of the different positive items commonly greatly differ, with grandiose ideas and conceptual disorganization often reported as least frequent or pronounced (17, 23–25). This heterogeneity of positive items may be partly caused by age and sex. With regard to sex, in clinical samples, more conceptual disorganization (17, 26) and grandiose ideas (17) were found in male participants, whereas female participants showed more severe (27, 28) or more frequent perceptual aberrations (29). This was partly supported by a community study that reported more delusional and perceptual APS in female participants, and a trend significance toward more frequent conceptual disorganization in males participants. Other studies, however, did not show any sex differences in positive items of UHR assessments (30–34). Furthermore, both community and CHR studies reported age effects on the prevalence and clinical relevance—in terms of an association with non-psychotic mental disorders and/or functioning—of APS, with higher frequency and fluctuation of perceptual APS and lesser clinical relevance of delusional APS in younger age groups, in particular those below the age of 16 years (35–38).
First studies on the prevalence rates of APS/BIPS contents in UHR individuals of the North American Prodrome Longitudinal Study 2 (NAPLS-2) (39), conducted in several states of the United States of America (US) and Canada, and a US undergraduate sample (40) using categories predefined in the Content of Attenuated Positive Symptoms (CAPS) codebook (41) indicated that the heterogeneity of contents of APS/BIPS by far exceeds heterogeneity in positive items of UHR assessments. Yet, age and sex effects have not been studied so far with regard to detailed APS/BIPS contents, and neither has the impact of country, religion, functioning, and comorbidities on APS/BIPS contents been studied in UHR samples.
Therefore, our study aimed to detail the contents of APS and BIPS and their prevalence within a large CHR sample of the European Personalized Prognostic Tools for Early Psychosis Management (PRONIA) study (42); (https://www.pronia.eu). Furthermore, to detect what clinical or sociodemographic variable might be related most to the heterogeneity of contents, we examined the cross-sectional association of contents with sex, age, country, religion, psychiatric comorbidity, and functioning to gain a better understanding of the clinical presentation of UHR patients and, hereby, to better target intervention for current APS/BIPS. Based on the above studies, we expected that perceptual APS/BIPS contents would be more frequent in younger and/or female participants, and grandiose contents and signs of conceptual disorganization more frequent in male participants. Furthermore, for the consistent findings of age effects (36–39) and the inconsistent findings of sex effects on APS/BIPS (17, 26–35), we expected that age would be more related to contents than sex.
2. Materials and methods
2.1. Sample
The CHR sample (N = 232) was recruited as part of the PRONIA study, which was funded by a grant from the European Commission and carried out at ten early detection centers in Germany, Italy, England, Finland, and Switzerland between 02/2014 and 11/2018 (42, 43). CHR patients had to meet the following inclusion criteria: age between 15 and 40 years, meeting at least one of the three UHR criteria and/or the basic symptom criterion COGDIS, language skills sufficient for participation, and sufficient capacity to consent/assent.
Participants with a past or present diagnosis of a manifest psychotic disorder, an antipsychotic medication for more than 30 days (cumulative number of days) at or above minimum dosage of the “1st episode psychosis” range of the S3 Guidelines Schizophrenia of the Deutsche Gesellschaft für Psychiatrie und Psychotherapie, Psychosomatik und Nervenheilkunde (DGPPN; German Association for Psychiatry, Psychotherapy, and Psychosomatics) (44) (Supplementary Table 1), or any intake of antipsychotic medication (i.e., independent of the duration of intake) within the past 3 months before psychopathological baseline assessments at or above minimum dosage of the “1st episode psychosis” range of DGPPN S3 Guidelines (Supplementary Table 1) were excluded. Furthermore, an intelligence quotient below 70, not sufficient hearing for neurocognitive testing, current or past head trauma with loss of consciousness for more than 5 min, current or past known neurological disorder of the brain, current or past known somatic disorder potentially affecting the structure or functioning of the brain, current or past alcohol dependency, current polytoxicomania (poly-dependency) or polytoxicomania (poly-dependency) within the past 6 months, and the inability to undergo a magnetic resonance imaging for medical or personal reasons were exclusion criteria of the study.
Because APS/BIPS can also occur outside samples meeting the frequency and course requirements of the symptomatic UHR criteria (25, 45), all CHR patients were considered in analyses (Table 1).
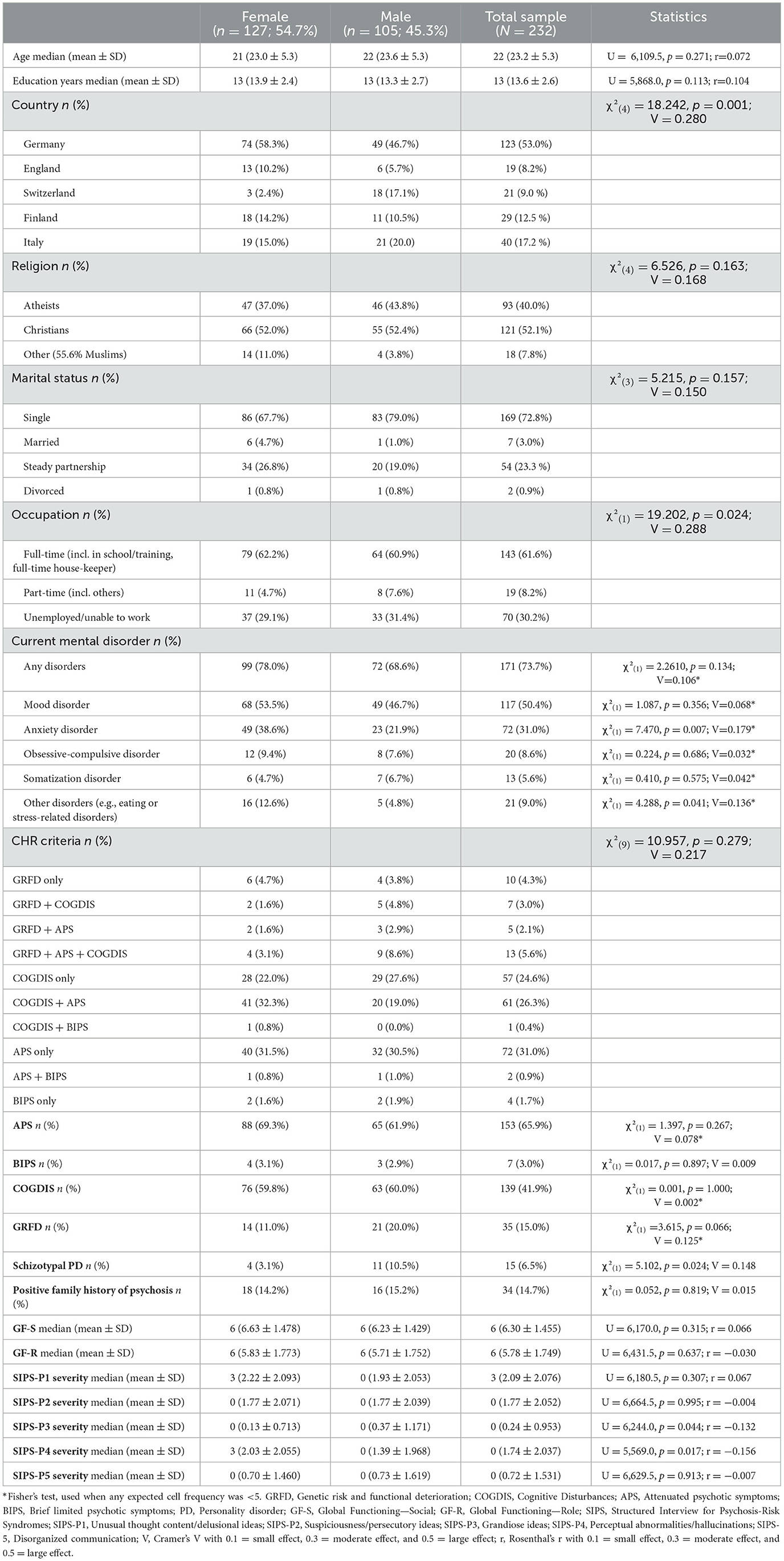
Table 1. Sociodemographic and clinical characteristics of the sample.
The study was approved by all local ethics committees, and all participants and, where required, the participants' parents/guardians gave written informed consent/assent.
2.2. Assessments
CHR criteria and symptoms were assessed using semi-structured clinical interview assessments: UHR criteria were assessed with the Structured Interview for Psychosis-Risk Syndromes (SIPS) (12) and COGDIS with the Schizophrenia Proneness Instrument—Adult version (SPI-A) (46). The five positive SIPS-items (SIPS-P1 “unusual thought content/delusional ideas”; SIPS-P2 “suspiciousness/persecutory ideas”; SIPS-P3 “grandiose ideas”; SIPS-P4 “perceptual abnormalities/hallucinations”; and SIPS-P5 “disorganized communication”) are each rated syndromally for severity based on anchor points ranging from 0 = “absent” to 6 = “severe and psychotic”. These anchors are intended to provide guidelines and examples of signs for every observed symptom but not exact definitions. For example, in P1 “unusual thought content/delusional ideas”, a score of 1 = “questionably present” is rated for symptoms that are perceived as puzzling mind tricks or a sense that something is different, such as déjà-vu experiences, mild changes in perception of time, or vague feelings of estrangement; while a score of 5 = “severe but not psychotic” is appointed to non-paranoid, non-grandiose delusional ideas (such as Ich-Störungen, unusual nihilistic, erotomane, religious, referential, or somatic ideas, or unusual ideas about guilt or jealousy) that have become familiar, appear distressingly real, and affect functioning but can still be doubted when contrary evidence or other opinions are presented. A score of 3–5 on a positive SIPS item signifies the presence of an APS, and a score of 6 indicates the presence of a BIPS.
A risk syndrome with APS requires that at least one APS (1) began within the past year or was rated one or more points higher on the severity scale compared to 12 months ago (2), occurred at an average frequency of at least once per week for at least several minutes per event in the past month, and (3) was not better explained by another mental disorder. A risk syndrome with BIPS (that was slightly modified in PRONIA) requires that at least one BIPS (1a) was present at a severity level of 6 within each of the past 3 months (irrespective of the time a severity of 6 was reached) for at least several minutes per day at a frequency of at least once per month or (1b) was present at a severity level of 6 within the past month (irrespective of the time a severity of 6 was reached) for at least several minutes at a mean frequency of at least once per week or in a cumulative frequency of at least 1 h, (2) spontaneously remitted to a severity level of < 6 within 1 week (i.e., without antipsychotic medication), and (3) was not better explained by another mental disorder. Next to these two symptomatic risk syndromes, the SIPS includes the GRFD syndrome that requires (1a) meeting SIPS criteria for a Schizotypal Personality Disorder and/or (1b) having a first-degree relative with a psychotic disorder, and (2) a drop in the global assessment of functioning (GAF) score within the past 12 months by at least 30%.
Contrary to the syndromal item rating of the SIPS, each SPI-A item represents exactly one clearly defined basic symptom, which is rated according to its maximum occurrence within the past 3 months from 0 = “absent” to 6 = “daily”. Basic symptoms are subtle, subjectively experienced disturbances in mental processes including thinking, speech, attention, perception, drive, stress tolerance, and affect that are immediately self-recognized as deviations from “normal” mental processes and commonly not directly observable by others (47). For their spontaneous, immediate self-recognition as disturbances of their own mental processes, basic symptoms are distinct from hallucinatory and delusional APS and BIPS, in which reality testing is disturbed at least to some degree and which are at least briefly perceived as real or realistic. In addition, for the intact immediate self-reflection, basic symptoms are also distinct from observed but often not self-perceived signs of disorganized communication. Because of their strict connection to mental processes, cognitive basic symptoms are therefore not differentiable by thought content like delusional APS and BIPS. The risk syndrome COGDIS requires the presence of at least 2 of the following 9 cognitive basic symptoms with at least weekly occurrence during the last 3 months, i.e., a score ≥3 in the SPI-A: inability to divide attention (B1); captivation of attention by details of the visual field (O7); disturbance of receptive (C4), expressive speech (C5), or abstract thinking (O3); thought interference (C2); blockages (C3) or pressure (D3); and unstable ideas of reference (D4).
To rule out lifetime psychosis and to evaluate other mental disorders, patients were assessed with the Structured Clinical Interview for the Diagnostic and Statistical Manual of mental disorders, fourth edition, Text Revision (DSM-IV-TR) (48). Moreover, the Global Functioning: Social (GF:S) (49) and the Global Functioning: Role (GF:R) (50) assessed social and role functioning. A score of 6 or lower in GF:R and GF:S signify the presence of a functional deficit.
In addition to training of all interviewers, weekly supervision was implemented within each center and monthly CHR case conferences on inclusion-relevant CHR symptoms by phone with the senior author (F.S.-L.), an expert in early detection of psychoses and qualified trainer of both SPI-A and SIPS, were performed to guarantee excellent and reliable data quality.
For supervision purposes, case vignettes of each patient possibly meeting CHR criteria were prepared, giving a synopsis of the patient's description of the content, course, and impact on the functioning of each reported potentially inclusion-relevant CHR symptom, i.e., the five positive SIPS items and the 9 COGDIS symptoms, when scored at least 3. These case vignettes formed the basis for the monthly case conferences, in which they were discussed in detail with F.S.-L. In case the assessment was insufficient, i.e., relevant questions of FS-L could not be answered, the patient was interviewed again for these open questions and the case was discussed again. From these case vignettes, i.e., symptom descriptions, the first author (CT) extracted phenomenological contents of all APS and/or BIPS. All extracted contents were discussed under regular supervision by FS-L (Supplementary Table 2 gives examples of symptom descriptions from case vignettes and the content extracted from these).
2.3. Data analyses
Using version 28.0.1.1 of the Statistical Package for the Social Sciences, the frequency of the contents was descriptively compared for sex, age, country, comorbid mental disorders, and GF:S and GF:R using χ2-test or Fisher's exact test for nominal and Kruskal–Wallis or Mann–Whitney tests for continuous data. Next, contents showing a cell with a significant Standardized Residual (SR>|1,96|) in χ-test2 test or trend significance (p < 0.10) were examined for their association with the above factors in regression analyses using logistic regression for binary data with k = 2, multinominal regression for categorical data with k ≥ 2, and ordinal or linear regression for continuous data. Because an external validation set was not available, we used bootstrapping validation of regression models to predict their fit to a hypothetical testing set.
3. Results
3.1. Sociodemographic characteristics
Table 1 shows the sample characteristics. Most patients were recruited in the four German centers (53.0%), followed by the three Italian centers (17.2%). Although sex was evenly distributed in the total sample [ = 2.086, p = 0.168), the distribution of sex differed between countries, with a dominance of female participants in Germany and England and a dominance of male participants in Switzerland. Not significantly different between sexes, the median age in the total sample was 22 years and the median education years were 13 years. The majority of the sample was single (72.8%) and in full-time occupation (61.6%).
The median values of GF-S and GF-R were 6 each, indicating moderate impairment in both functional domains. Most patients (73.7%) had a mental disorder next to their CHR status. Of these, mood disorders were the most frequent (50.4%), followed by anxiety disorders (31.0%) which were more frequent in female participants. Disorders of other main diagnostic categories were present in < 10% of the sample. Disorders of main diagnostic categories according to DSM-IV-TR with a presence of < 5% (n = 11), such as eating disorders, were summarized as “other disorders” in analyses for power reasons (Table 1).
Regarding CHR criteria, the symptomatic UHR criteria were met by 158 (68.1%) patients. The APS syndrome was the most frequent (65.9%), followed by COGDIS (41.9%). The APS syndrome occurred mainly by itself (31.0%) but also frequently in combination with COGDIS (31.9%). The BIPS syndrome was infrequently met (3.0%), in almost half of the instances in combination with the APS syndrome or COGDIS (Table 1).
3.2. Number and type of contents of attenuated and brief intermittent psychotic symptoms
We distinguished 109 different thematic contents of APS and BIPS (Tables 2–4): 63 delusional contents (40 included in SIPS-P1, 17 included in SIPS-P2, and six included in SIPS-P3), 29 perceptual aberrations (SIPS-P4), and 17 signs of disorganized communication (SIPS-P5). Only 20 contents (18.3%) were present in more than 5% of patients (Tables 2–4). Nine of these were rated at “unusual thought content/delusional ideas” (SIPS-P1; Table 2), four at “suspiciousness/persecutory ideas” (SIPS-P2; Table 2), five at “perceptual abnormalities/hallucinations” (SIPS-P4; Table 3), and two at “disorganized communication” (SIPS-P5; Table 4). Paranoid-referential ideas related to being the focus of negative attention (24.6%) and ideas that others intend to harm the patient in a non-physical way (12.5%) were the two most frequent contents (Table 2). The most frequent content of “grandiose ideas” (SIPS-P4), i.e., “grandiose ideas with respect to own (natural) abilities”, was present in only 4.3% of patients (Table 2). Fifty-one contents (46.7%) were present in < 1% of the sample (Tables 2–4).

Table 2. Frequency of attenuated and transient delusional ideas (SIPS-P1, SIPS-P2, and SIPS-P3) in CHR patients in descending order (N = 232).
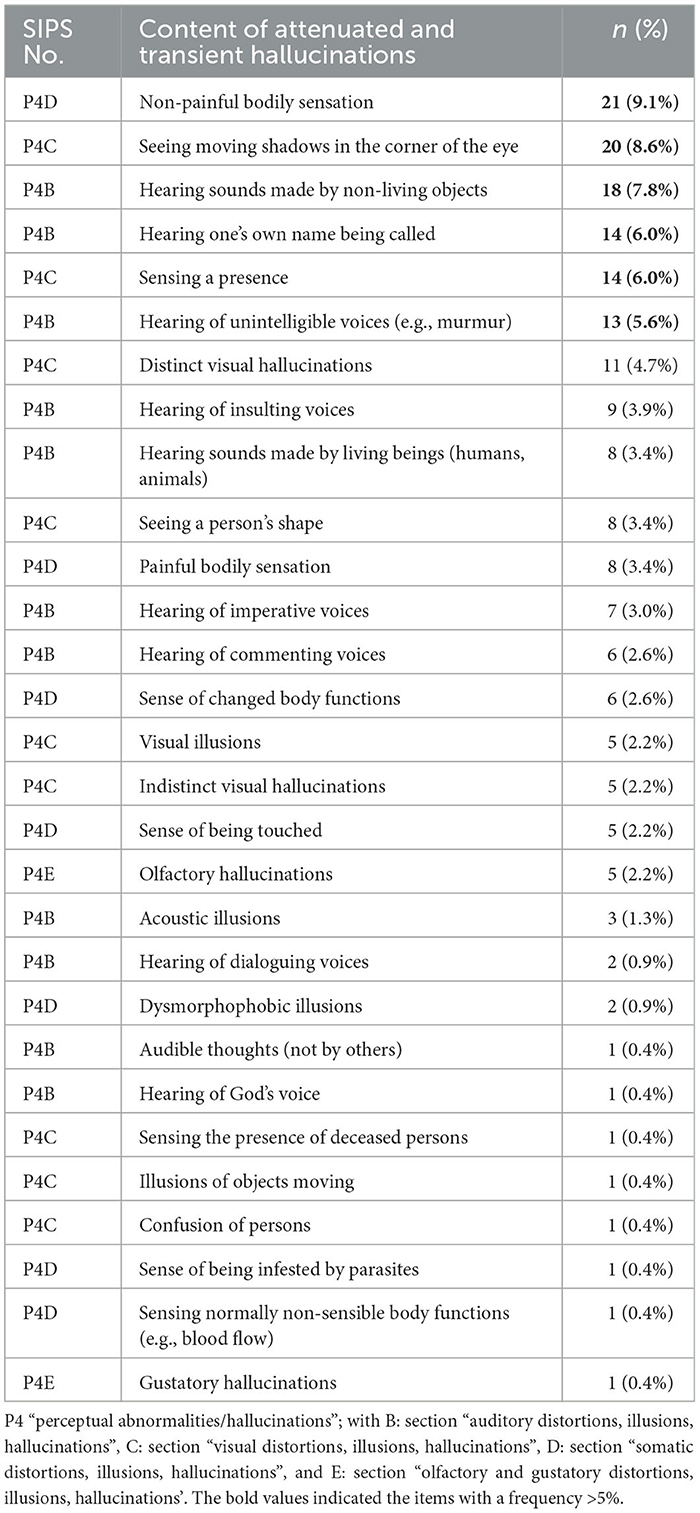
Table 3. Frequency of attenuated and transient hallucinations (SIPS-P4) in CHR patients in descending order (N = 232).
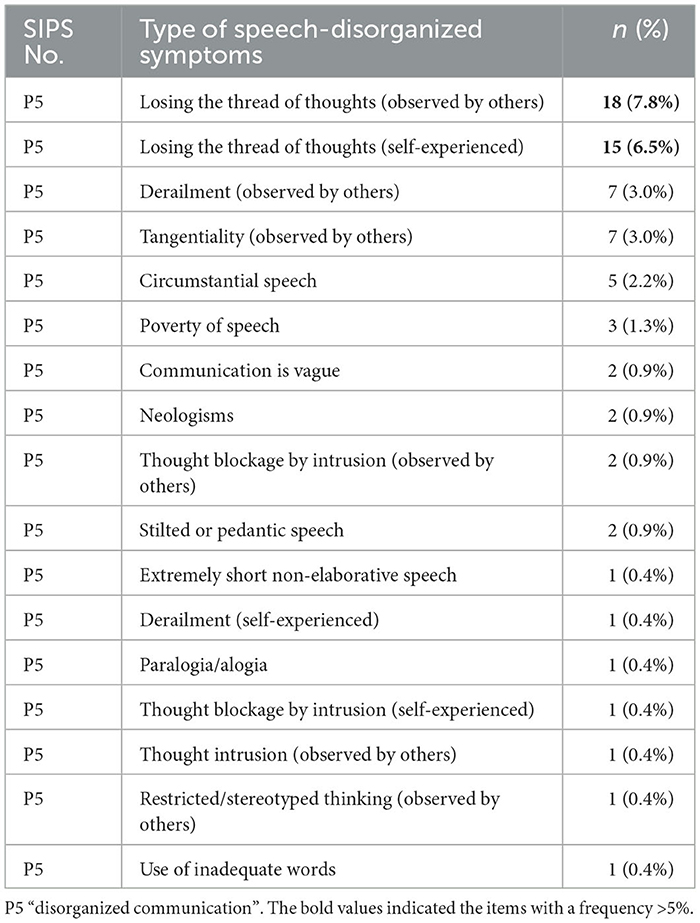
Table 4. Frequency of speech-disorganized symptoms (SIPS-P5) in CHR patients in descending order (N = 232).
3.3. Preselection of the contents of attenuated and brief intermittent psychotic symptoms with group differences
In group comparisons, a sex difference was found only for ideas of persecution (Supplementary Tables 3a–c). Thirty-three contents—20 delusional ideas, ten attenuated hallucinations, and three speech-disorganized symptoms—revealed any cell with SR>|1.96| or trend-level significance between countries (Supplementary Tables 4a–c), and five delusional contents and three speech-disorganized symptoms demonstrated any cell with SR>|1,96| or trend-level significance between religions (Supplementary Tables 5a–c). Furthermore, 32 contents, mainly delusional ideas, showed any cell with SR>|1,96| or trend-level significance in the group comparisons of the five main categories of mental disorders (Supplementary Tables 6–10). With respect to age, GF:S and GF:R, 38 contents, mainly delusional ideas, showed trend-level significance (Supplementary Tables 11–13).
3.4. Associations of the contents of attenuated and brief intermittent psychotic symptoms with psychosocial and clinical factors
3.4.1. Associations of the contents of attenuated and brief intermittent psychotic symptoms with age and sex
In the significant univariate regression model of sex [Wald(1) = 3.309, p = 0.041]; female participants as the reference group) that explained 2.9% of the variance, “ideas of persecution” was associated with male sex [Beta = −1.945; Exp(Beta) = 0.143, 95%CI: −21.283/−0.450).
For age, the regression analysis of the 18 items revealed negative associations with five items (“nihilistic ideas about the non-existence of others”, “demarcation experiences”, “paranoid ideas of reference (gazes of passers-by)”, “indistinct visual hallucinations”, and “sense of being touched”) and positive associations with three items (“identity confusion”, “acoustic illusions”, “extremely short, non-elaborative speech”), whereby 23.6% of the variance was explained (Table 5).
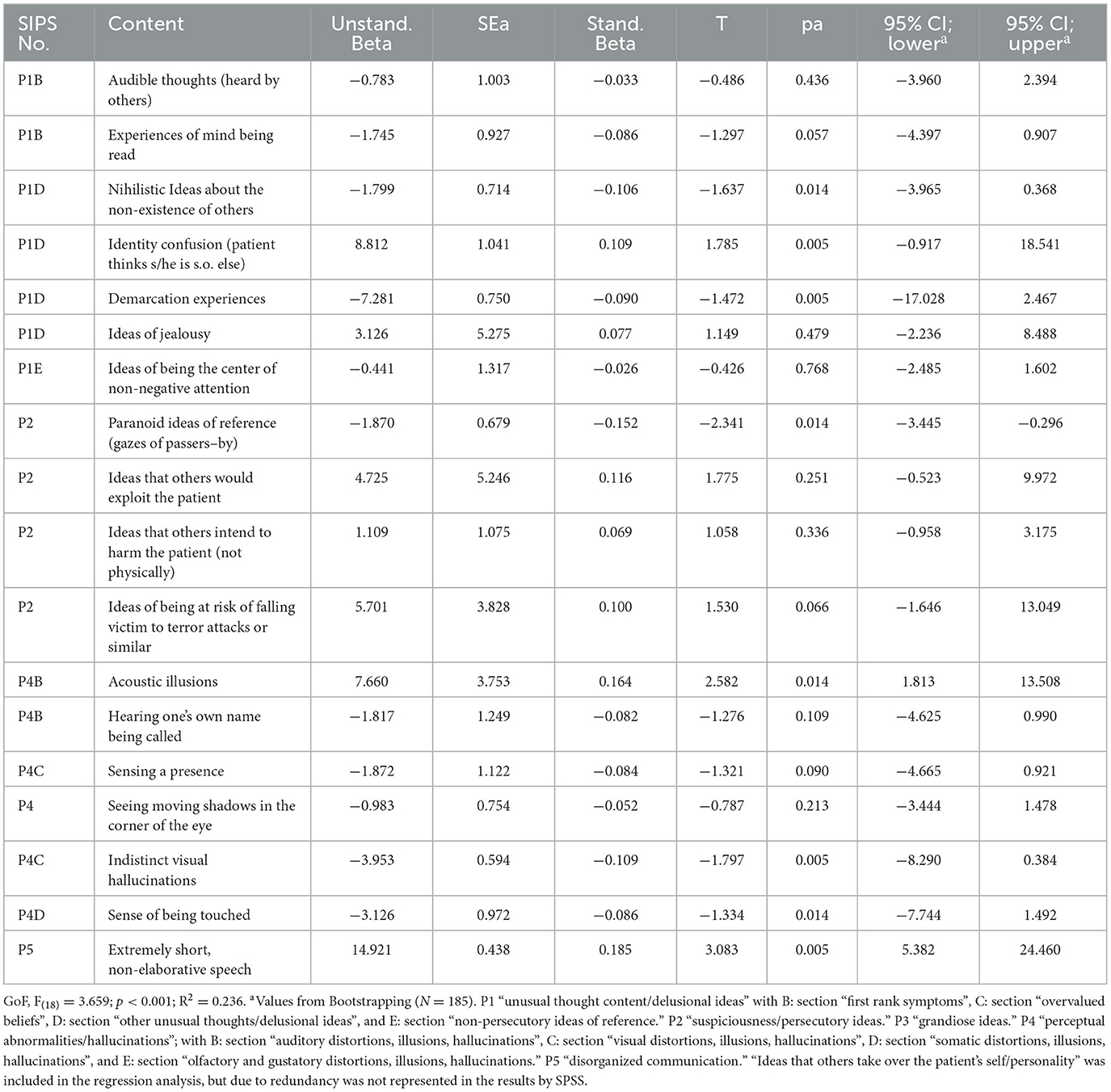
Table 5. Association of the contents of attenuated and brief intermittent psychotic symptoms with age, linear regression analysis (N = 232).
3.4.2. Associations of the contents of attenuated and brief intermittent psychotic symptoms with country and religion
Although the model of religion became significant and explained 16.4% of the variance, none of the eight contents was a significant predictor (Table 6), also because of the rarity of contents and, relatedly, absence of contents in some subgroups (Supplementary Tables 5a–c) led to 0% confidence levels, indicating that the result is likely unreliable, i.e., unlikely to be repeated in other samples.
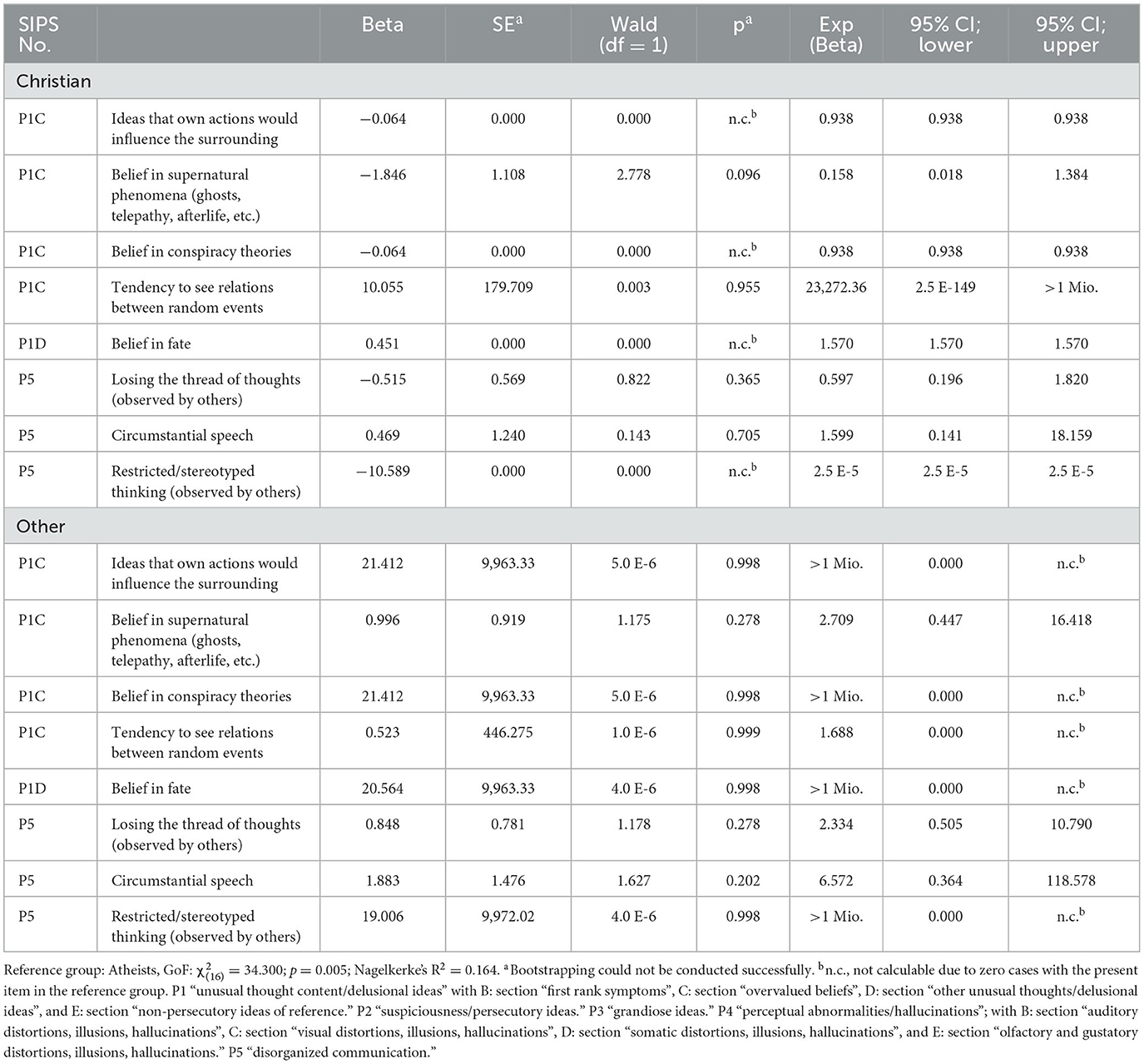
Table 6. Association of the contents of attenuated and brief intermittent psychotic symptoms with religion, multi-nominal regression analysis (N = 232).
The significant regression model of the country with Germany as a reference revealed that 55.8% explained variance (Table 7). Positive associations were found for “hypochondriac ideas” for Finland, and “numbers have a special meaning”, “hypochondriac ideas”, “mistrust against friends”, and “hearing one's own name being called” for Italy (Table 7). No content significantly distinguished England or Switzerland from the reference country Germany.

Table 7. Association of the contents of attenuated and brief intermittent psychotic symptoms with country, multi-nominal regression analysis (N = 232).
3.4.3. Associations of the contents of attenuated and brief intermittent psychotic symptoms with mental disorders and functioning
The regression analyses of mental disorders with the absence of a mental disorder as a reference group revealed significant models for all diagnostic categories that, increasing with the number of significant contents, showed explained variances between 13.7% for mood disorders and 38.3% for obsessive-compulsive disorders (OCD) (Tables 8–12).
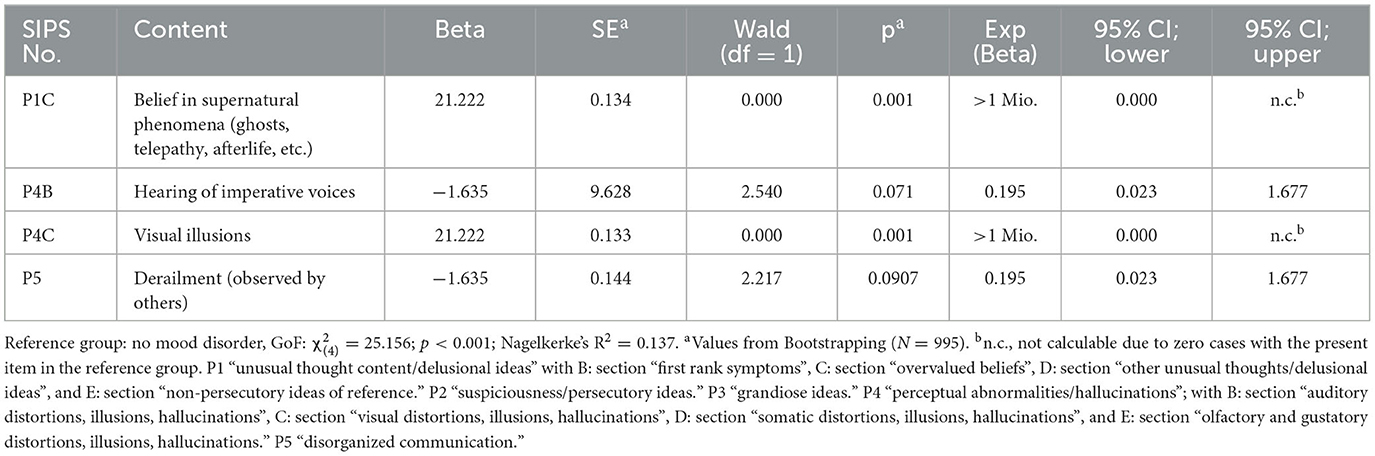
Table 8. Association of the contents of attenuated and brief intermittent psychotic symptoms with the presence of a mood disorder, logistic regression analysis (N = 232).
Mood disorders revealed two positive associations with “belief in supernatural phenomena” and “visual illusions” (Table 8). Yet, as with several other contents in the disorder models, the rarity of contents and, relatedly, absence of contents in some subgroups led to 0% confidence levels, indicating that the result is likely unreliable, i.e., unlikely to be repeated in other samples. The model of anxiety disorders that explained 16.4% of variance included one significant but unreliable positive association with “ideas that others intend to poison the patient”, one positive association with “ideas that others intend to harm the patient (not physically)”, one significant unreliable negative association with “grandiose ideas with respect to own abilities”, and one significant negative association with “ideas of being the center of non-negative attention” (Table 9). The model on other disorders included three significant positive associations (with “experience of being controlled by external forces”, “paranoid ideas of reference involving friends/family”, and “painful bodily sensation”) and one unreliable negative association with “unusual religious ideas”, and explained 17.9% of the variance (Table 10). For somatization disorders (Table 11), significant positive associations were found with “thought withdrawal”, “sense of changed body functions”, “neologisms”, and “poverty of speech”, and two unreliable positive associations with “ideas of being pregnant” and “ideas that supernatural beings intend to harm the patient”. The somatization disorder model explained 32.4% of the variance. The model on OCD revealed the second highest rate of explained variance in APS/BIPS contents (38.3%; Table 12). Significant positive associations occurred with “thought withdrawal”, “tendency to see relations between random events”, “nihilistic ideas of being dead/dying”, “ideas of observing oneself from a birds-eye perspective”, and “losing the thread of thoughts (self experienced)”. Additionally, “belief that everything is connected” and “ideas of being observed anonymously” showed positive but unreliable associations with OCD (Table 12).
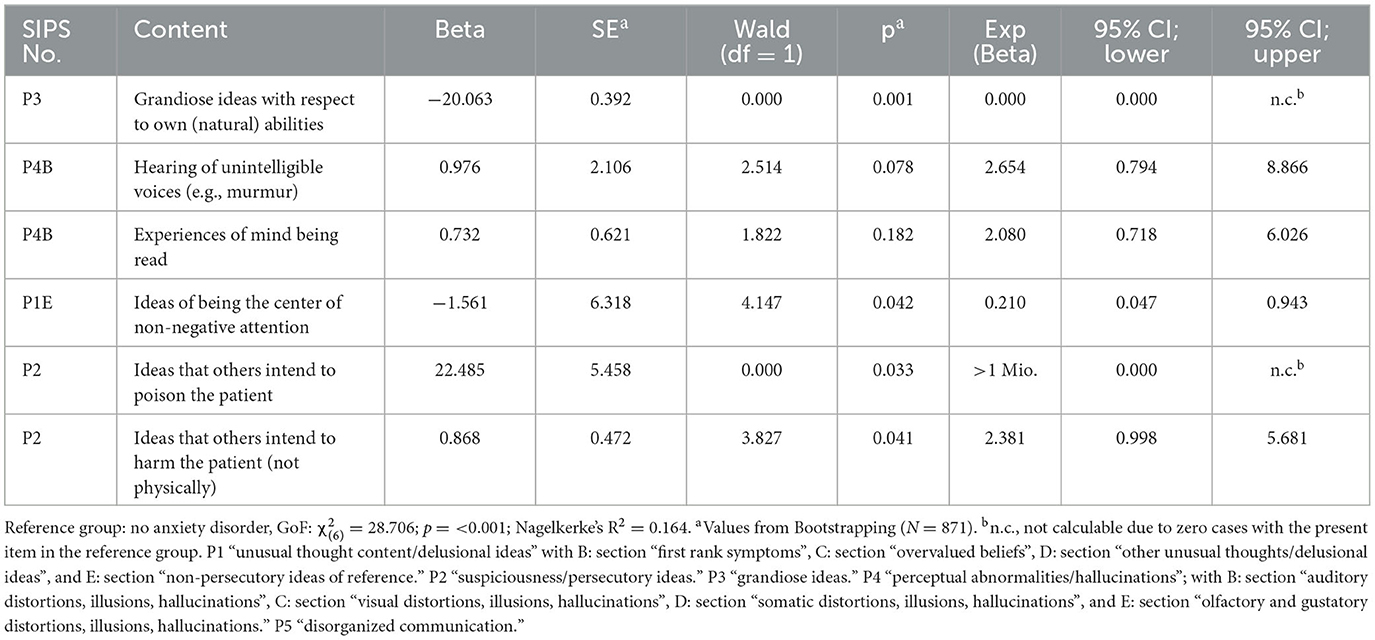
Table 9. Association of the contents of attenuated and brief intermittent psychotic symptoms with presence of an anxiety disorder, logistic regression analysis (N = 232).
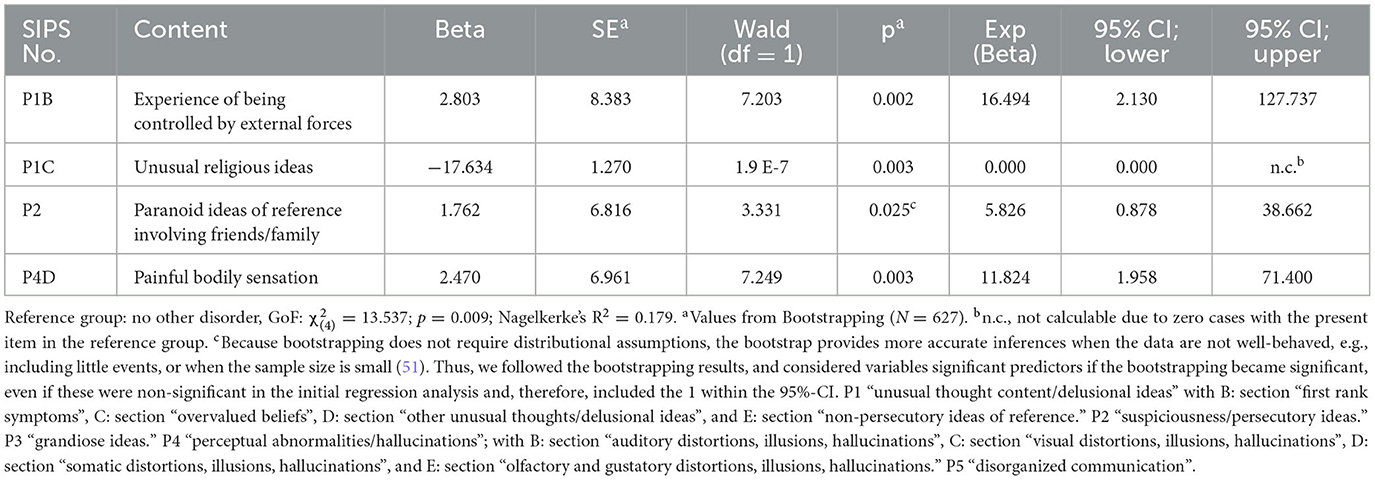
Table 10. Association of the contents of attenuated and brief intermittent psychotic symptoms with other disorders, logistic regression analysis (N = 232).
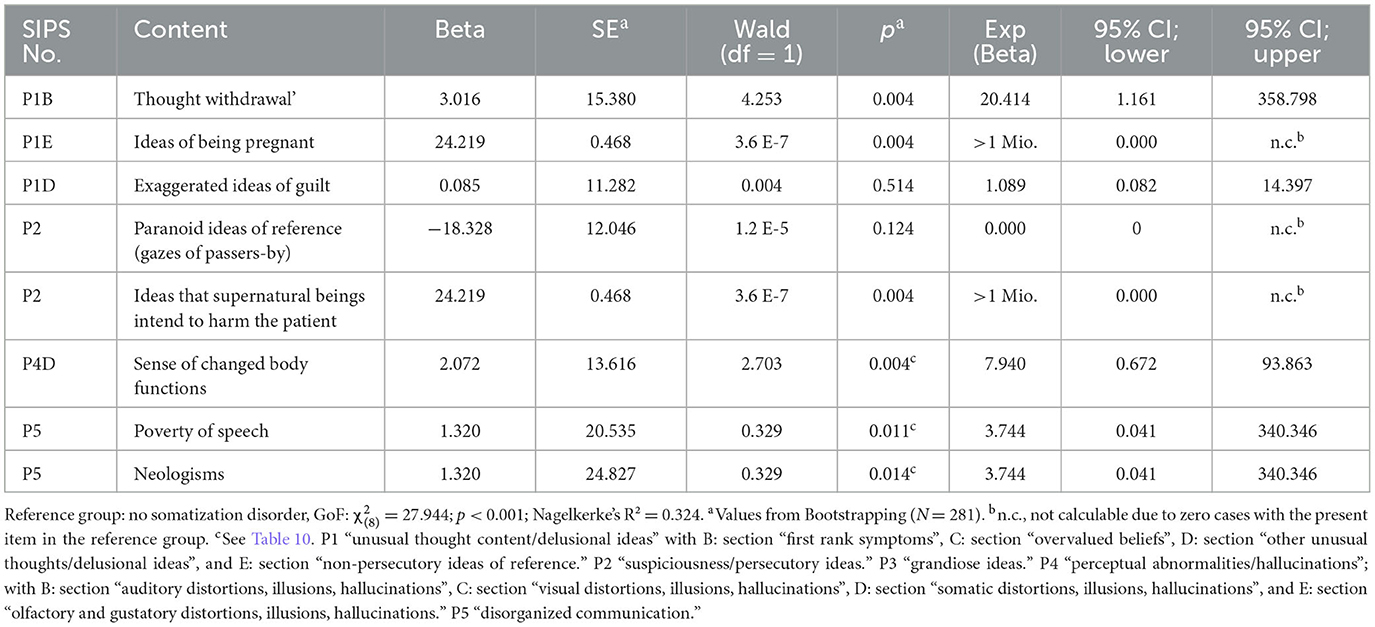
Table 11. Association of the contents of attenuated and brief intermittent psychotic symptoms with somatization disorder, logistic regression analysis (N = 232).
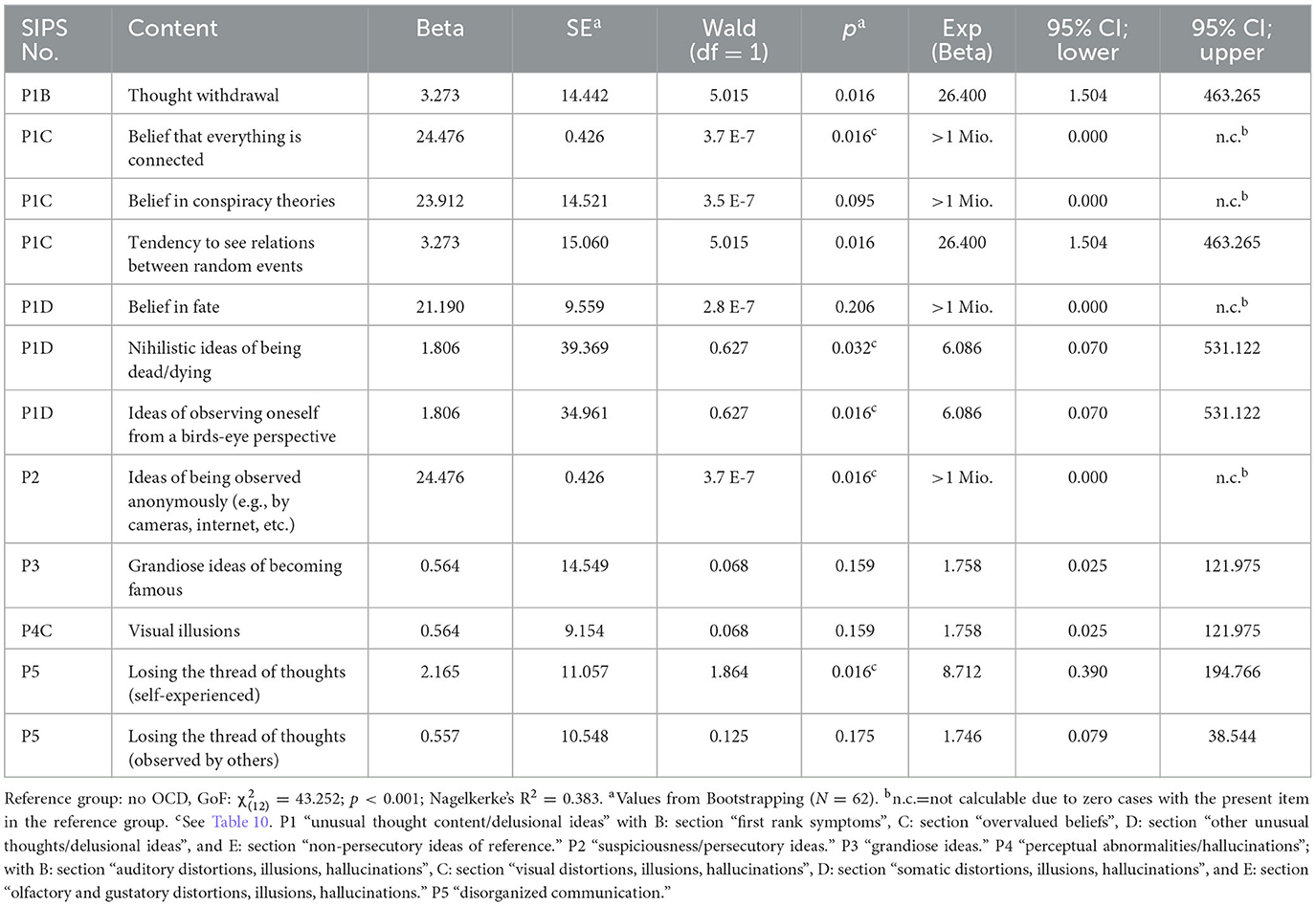
Table 12. Association of the contents of attenuated and brief intermittent psychotic symptoms with obsessive-compulsive disorder (OCD), logistic regression analysis (N = 232).
The model on social functioning (GF:S), which explained 20.9% of the variance, indicated that better social functioning was associated with “seeing moving shadows in the corner of the eye”, while poorer functioning was associated with “thought insertion” and “general mistrust” (Table 13). With regard to role functioning (GF:R), better functioning was associated with “ideas that others would exploit the patient”, while poorer functioning was associated with “neologisms” (Table 14). The GF:R model explained 15.8% of the variance.
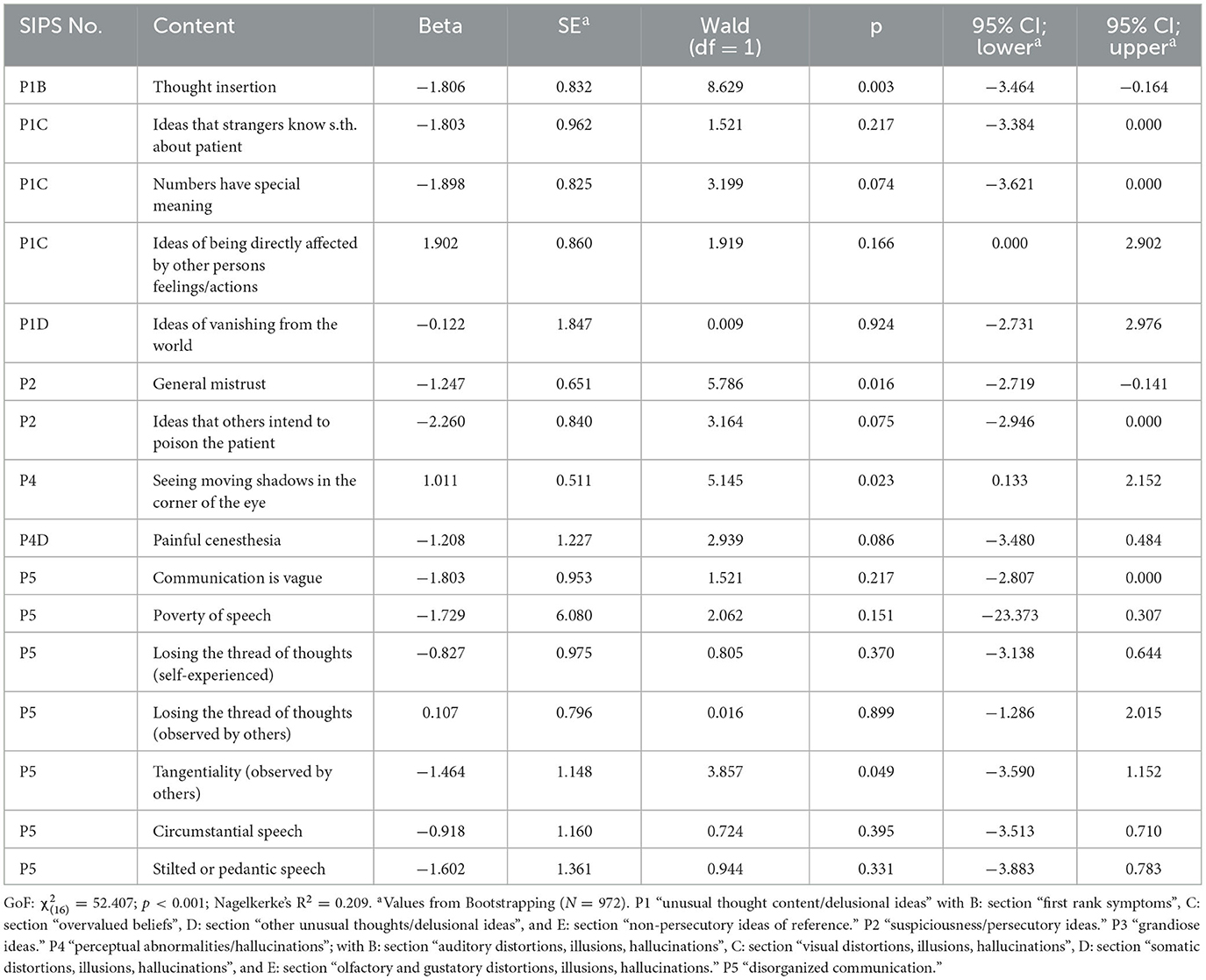
Table 13. Association of the contents of attenuated and brief intermittent psychotic symptoms with social functioning, ordinal regression analysis (N = 232).
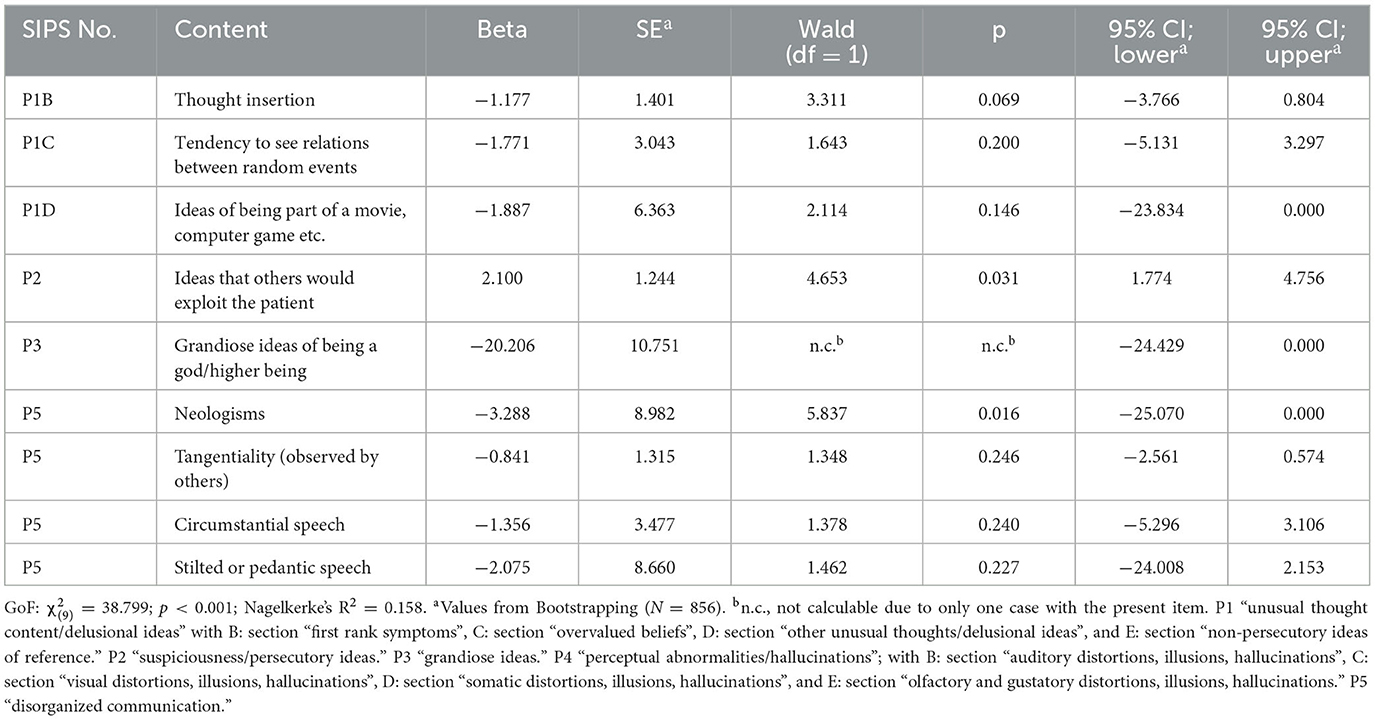
Table 14. Association of the contents of attenuated and brief intermittent psychotic symptoms with role functioning, ordinal regression analysis (N = 232).
4. Discussion
We detailed the contents of APS/BIPS and investigated their association with sex, age, country, religion, functioning, and comorbidities for the first time in a large European CHR sample to gain a better understanding of the clinical presentation of CHR and, in particular, UHR patients. Supporting notions of high heterogeneity of UHR states and the contents of their constituting symptoms (39), we found 109 discernible contents of mainly low prevalence, i.e., a presence in < 5% of patients. Thirty-one reliable contents (28.5%), including eight of the 20 contents with a prevalence of ≥5%, showed an association with either sex, age, country, functional deficits, and/or comorbid mental disorders, while none were associated with religion.
4.1. Prevalence rates of the contents of attenuated and brief intermittent psychotic symptoms
In the whole sample, the prevalence rates of the 109 contents, of which 58% (n = 63) were delusional, varied between 24.6% (n = 57) for “paranoid ideas of reference” (e.g., people watching the patient are thinking negatively about him/her) and 0.4% (n = 1); this latter low prevalence rate was found for 33 delusional, hallucinatory, and speech-disorganized contents. When only patients meeting symptomatic UHR criteria (n = 158, 68.1%) were considered (Supplementary Table 14), these numbers rose to 36.1 and 0.6%. When we compared our results to the earlier studies of APS contents that used the CAPS (40, 41), in both our whole sample and our APS/BIPS subsample, even the most frequent content in our sample was less frequent than the most frequent CAPS-rated contents (see Supplementary Table 14 for a comparison of contents and their frequencies between our sample and the samples reported by Marshall et al. (39) and Trask et al. (40). In the undergraduate control subsample and the negative schizotypy subsample of Trask et al. (40), “ideas of being thought about in a bad way” (present in 51.2% of controls and 61.9% of negative schizotypes) and “guardedness toward people” (present in 41.5% of controls and 57.1% of negative schizotypes) were most frequent. In positive schizotypes (40) and patients with APS (39), “perplexed by reality” (77.6% in positive schizotypes and 54.1% in APS patients) was the most frequent, with “guardedness toward people” being equally frequent in positive schizotypes (77.6%) but less frequent in APS patients (42.6%). The second most frequent content in the APS sample (39) was “overvalued ideas” (52.3%), which was also among the four most frequent contents in positive (67.3%) and negative schizotypes (38.1%) and controls (22.0%) (40).
The lower ratings of these contents in our sample are likely related to a stricter definition of delusional APS as distinct ideas. Thus, mere feelings, even strong ones, that something might be different, or a self-experienced confusion of memories of dreams with memories of real events as captured by “perplexed by reality” that did not involve distinct ideas about a changed reality were not rated as APS in our study. A stricter rating of APS in our study may also explain the much higher frequency of “guardedness toward people” in the two studies using CAPS (39, 40) as we only rated distinct ideas but not indistinct feelings, such as a vague sense of unease or hypervigilance without a clear source of danger. Our stricter rating is supported by the suggestion of Trask et al. (40) that these most frequent contents may represent mild psychotic-like experiences of below-APS-threshold severity rather than clinically significant APS. Similarly, contents of “overvalued ideas” of the CAPS were only rated at APS severity in our study when related to contents of magical thinking but not when related to assumptions and beliefs, which determine the patient's actions to a morbid degree but are shared by other members of the same culture (i.e., overvalued ideas in their original definition), because (attenuated) delusions are false ideas unique to their possessor and not shared by other members of the same culture, or understandable in the context of other abnormal phenomena, such as (attenuated) hallucinations (52).
However, when only the rates in the 158 PRONIA patients meeting symptomatic UHR criteria were considered and compared to the NAPLS-2 APS patient sample (39), Ich-Störungen in terms of “thought reading”, “thought broadcast”, or “audible thoughts”; non-paranoid referential, somatic, and persecutory ideas; ideas of guilt, jealousy, or possessing supernatural abilities; as well as “unusual somatic perceptions of pains and bodily functions” showed similar frequencies in both samples (Supplementary Table 14). Only nihilistic and observation ideas (incl. frequent paranoid-referential ideas) were more frequent in the PRONIA sample, while schizotypy-like features (“odd ideas concerning supernatural beings/forces”, “unusual religious ideas”, “magical thinking/overvalued ideas”, and “suspiciousness/paranoid ideation”), grandiose ideas, and perceptual aberrations were more frequent in the NAPLS-2 sample (39). Of note, no unusual thoughts (SIPS-P1) with violent contents involving others or the patient as the victim were reported in our sample, whereas Marshal et al. (39) found them in 19.1% of their sample. Because ratings of paranoid ideas (SIPS-P2) involving physical harm to the patient were also less frequent compared to the NAPLS-2 sample (39, 53), this difference is not explained by potential differences in scoring for violent contents (SIPS-P1 vs. SIPS-P2).
Reflecting cultural characteristics, the higher prevalence rates in the NAPLS-2 sample might be explained by the lower prevalence of schizotypal personality disorders and lesser severity of positive schizotypy reported for Europe and the two main countries of PRONIA, Germany and Italy, compared to the US (54–56). This would be in line with the fact that higher rates of these contents were also found in the positive schizotypy undergraduate sample (40).
4.2. Association of the contents of attenuated and brief intermittent psychotic symptoms with sex and age
For sex, we found only one association of male sex with “ìdeas of persecution” that explained little variance. This finding is mainly in line with earlier studies that reported no sex differences (30–34) and did not replicate findings of more disorganization (17, 26) or grandiose ideas (17) in male and more attenuated hallucinations in female patients (29). However, one study (17) reported that paranoid and also speech-disorganization APS predicted psychosis specifically in male patients. Yet, for its minor role in our study, sex likely played a minor role in the differences between the NAPLS-2 (40) and the positive schizotypy samples (40), and our PRONIA sample that comprised the same sex distribution as the positive schizotypy sample and a 12% higher rate of females compared to the NAPLS-2 sample. However, due to mostly low prevalence rates of grandiose contents (P3) and specifically attenuated hallucinations (P4), statistical power may not have been sufficient to replicate the reported sex differences for specific contents, which have not been investigated in other studies so far. Another reason for the frequently higher prevalence rates in the NAPLS-2 and positive schizotypy samples might be the younger age of these samples that were on average 5 years younger than the PRONIA sample. Higher rates of schizotypal features and APS/BIPS have been repeatedly related to younger age, especially an age below 16 years (36, 37, 57–59). Thus, unsurprisingly for the few adolescents included in PRONIA (n = 16; 6.9%), age explained only 23.6% of the variance.
Nevertheless, our results support calls for more consideration of age-related factors in CHR research (60). In line with reports from early-onset and adult-onset psychosis (59), multimodal and visual hallucinations were more frequent in younger patients and abnormal acoustic perceptions were more frequent in older patients. Furthermore, some nihilistic contents but the one-off “identity confusion” were more frequent in younger patients, this corresponding to reports of higher levels of bizarre positive symptoms in early-onset compared to adult-onset psychosis (59). Also, “paranoid referential ideas by passers-by” of all ages were more frequent in younger patients, likely reflecting younger patients' liability toward less elaborated and vaguer delusions that are more linked to real experiences (59) and/or the possibly transdiagnostic status of paranoid ideas in minors (45). Finally, the higher frequency of “extremely short, non-elaborative speech” in older patients is in agreement with speech-disorganized symptoms slightly increasing with age in 16–40-year-old community subjects and might reflect aberrations in neurodevelopmental maturation and trajectories in cognitive development (18, 61).
4.3. Association of the contents of attenuated and brief intermittent psychotic symptoms with religion and country
In our sample, APS/BIPS content did not predict religion (Supplementary Table 14), although associations between symptoms and religion were demonstrated in schizophrenia patients (62). Yet, we mainly compared Christians with atheists and did not evaluate religiosity, which may mediate differences in APS/BIPS (63).
Despite the many discussed differences between the two US-American samples (39, 40), in our European sample and using Germany as a reference country, we found only a few associations of APS/BIPS with Finland and Italy, and none with Switzerland and England (Table 5). However, the low number of single contents and, consequently, the high number of cells with zero frequency resulted in several non-interpretable findings. “Hypochondriac ideas” were more frequent in Finland and/or Italy. Additionally, “hearing one's name called” in the absence of other persons, magical thinking in terms of numbers having a special meaning, and “mistrust against friends” in terms of positive schizotypal experiences were also more frequent in Italy which had the lowest expression of positive schizotypy in a world-wide 12-country comparison that, however, did not include Germany, Finland, or Switzerland (58). Thus, while this might point toward Germany possibly being even lower in the expression of schizotypy than Italy, the fact that no difference was found between Germany and England, which had the second-highest expression of schizotypy (58), contradicts this explanation. Thus, APS/BIPS likely differ most clearly between countries of clearly different backgrounds, such as the US and Shanghai (64), but also between countries of presumed more similar cultural backgrounds such as European countries and the US. Yet, they also seem to differ between European countries as signified by the fact that, at 55.8%, the country explained most of the variance of APS/BIPS, although these differences may be more subtle and related to overall patterns of contents rather than to the prevalence rates of specific contents. Overall, the results indicate that local or national peculiarities likely shape the expression of APS/BIPS to different degrees and possibly influence the predictive power of additional second-step prediction algorithms, such as the NAPLS-2 risk calculator (65). Therefore, national peculiarities should be more prominently considered in future CHR studies.
4.4. Associations of the contents of attenuated and brief intermittent psychotic symptoms with functioning and comorbidities
The association of APS contents with functioning was so far only studied by Trask et al. (40) in undergraduate students. They used the Global Assessment of Functioning (GAF) that is incorporated in the SIPS and assesses social and occupational functioning but also psychological symptoms. Yet, a comparison of the GAF with the symptom-independent Social and Occupational Functioning Assessment Scale (SOFAS) (66), the source scale of GF:S and GF:R, found GAF and SOFAS total scores to be practically exchangeable (67). Despite this correspondence between scales, the selected predictors of functioning differed greatly between our study and the study by Trask et al. (40). Only the CAPE-item “vague figures or shadows” and our corresponding content “seeing moving shadows in the corner of the eye” were selected in both studies. But while, in concert with “being perplexed by reality”, “ideas of guilt”, and “supernatural beliefs”, it predicted lower functioning in the undergraduates (41) and better social functioning in our patient sample; thereby counterbalancing the significant negative impact of “thought insertion”, “general mistrust”, and “tangential speech”. Poor role functioning was only significantly predicted by “neologisms”; this impact was counterbalanced by “ideas that others would exploit the patient”. The concordant negative role of signs of disorganized communication in functioning is consistent with reports of formal thought disorder severity predicting poor social functioning, unemployment, relapses, and re-hospitalizations in early stages of psychosis (68) and of an association between the disorganized schizotypy domain and functional impairment (69). The potential protective role played by the schizotypal perceptual aberration “seeing shadows in the corner of the eye” is possibly reinforcing notions of benign positive schizotypy in the absence of paranoid ideations, including general mistrust and disorganization (70), thus counterbalancing their effects, in particular, in social interactions. Interestingly, in line with earlier notions of better functioning in paranoid compared to non-paranoid psychiatric patients (71), “ideas that others would exploit the patient” was linked to better role functioning, indicating that different paranoid ideas might differentially impact functioning. In doing so, paranoid ideas, specifically “general mistrust” but possibly also ideas that others intend to harm the patient in some ways, may impact negatively more on social than on role functioning (72, 73).
To our best knowledge, this is the first study on the association between non-psychotic comorbidities and contents of APS/BIPS in CHR. Although depressive and anxiety disorders were commonly most frequent in CHR samples, including ours, in line with previous reports that both disorders were associated with negative and disorganized but not positive symptoms (74), APS/BIPS contents hardly predicted either disorder. Rather, other less frequent disorders, especially OCD and somatization disorders, demonstrated differential associations with various bizarre contents, somatic perception abnormalities, some paranoid ideas, magical thinking, and some cognitive disorganization. Yet, again, low frequencies impaired the interpretation of results in some instances.
Although a phenomenological overlap of “thought insertion” and compulsive thoughts is commonly discussed (75), the rare “thought withdrawal” (0.9%) was related to both OCD and somatization disorders. Furthermore, supporting the assumed link between magical ideation and OCD (76), especially neutralizing behaviors (77), some forms of magical thinking (e.g., “tendency to see relations between random events”) were associated with OCD in our study. Reports on depersonalization and related nihilistic ideas in OCD are conflicting (78, 79). Yet, our results indicate some association between nihilistic content, specifically ideas of being dead or dying, and OCD.
Thus, many of the associations of APS/BIPS contents with mental disorders replicate earlier findings and, consequently, have unlikely evolved by chance due to multiple testing. However, future studies should examine if the links of some APS contents with certain non-psychotic mental disorders limit their psychosis-predictive power and if contents with links to reduce functioning show increased risks for psychosis and long-term functional disability that was frequently observed in CHR samples (80).
4.5. Strengths and limitations
This study has the following strengths and limitations. The main strengths are the large sample size and the differential extraction of contents that was not limited by predefined categories. Limitations are the cross-sectional nature of the study that does not allow causal relations to be examined, and the lack of an external validation sample. Furthermore, the fact that 83.1% of the contents were reported by < 5% of the sample led to some hardly interpretable results, and limited statistical power in comparisons and the ability to analyze interaction effects of both contents and sociodemographic and clinical variables. Finally, for our emphasis on single contents and not on clusters or syndromes of contents, we did not analyze if the co-occurrence of contents might be additionally influenced by age, sex, country, and/or comorbid disorders.
5. Conclusion
Our study highlights the heterogeneity of a set of APS/BIPS contents in CHR patients and their various links with age, country, functioning, and comorbid mental disorders but also the invariance of another set of APS/BIPS contents that might thus be regarded as a symptomatic core of the symptomatic UHR criteria. The symptomatic core in adults and older adolescents seems mainly characterized by Ich-Störungen related to others knowing the patient's thoughts and other bizarre delusional contents, more distinct paranoid ideas of being harmed, shaped visual hallucinations, verbal, gustatoric, and olfactoric hallucinations, as well as derailed, circumstantial, or vague speech. The more heterogeneous contents in this age group seem to involve Ich-Störungen related to others controlling the patient's thoughts or actions, and schizotypal features, i.e., ideas of reference, magical thinking suspiciousness and ideas of persecution and observation, and unusual perceptual experience, hypochondriac ideas, as well as tangential, associatively loosened, or impoverished speech. This latter set of contents might moderate the clinical relevance, including the psychosis-predictive value, of APS/BIPS syndromes, thus accounting for the large heterogeneity in outcomes, including transition rates, of UHR samples (8, 11). Thus, as already called for with regard to the effect of age in children and young adolescents (60), future studies should examine if the reported associations of certain contents with age, country of assessment, functioning, and/or comorbid mental disorders moderate their related risk for psychosis and, possibly, for social and role functional disability related to CHR states. Knowledge of the influence of age and country, in particular, might support the development of awareness programs and CHR screeners that either well reflect the developmental and local pattern of CHR symptoms, or focus on a core set of contents that are applicable across a greater range of groups and countries.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving human participants were reviewed and approved by Heinrich-Heine-Universität Düsseldorf. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
Author contributions
NK, EM, and FS-L made substantial contributions to the conception or design of the work. NK and EM acquired the funding. CT, NO, and FS-L performed the analyses and interpreted the data for the study. CT and FS-L drafted the manuscript. All authors revisited it critically for important intellectual content, provided approval for publication of the content, and agreed to be accountable for all aspects of the study in ensuring that questions related to the accuracy or integrity of any part of the manuscript are appropriately investigated and resolved.
The PRONIA consortium
The following members of the PRONIA Consortium performed the screening, recruitment, rating, examination, and follow-up of the study participants and were involved in implementing the examination protocols of the study, setting up its information technology infrastructure, and organizing the flow and quality control of the data analyzed in this study between the local study sites and the central study database: Shalaila Haas, Alkomiet Hasan, Claudius Hoff, Ifrah Khanyaree, Aylin Melo, Susanna Muckenhuber-Sternbauer, Yanis Köhler, Ömer Öztürk, Nora Penzel, David Popovic, Adrian Rangnick, Sebastian von Saldern, Rachele Sanfelici, Moritz Spangemacher, Ana Tupac, Maria Fernanda Urquijo-Castro, Johanna Weiske, Antonia Wosgien, Camilla Krämer, and Rachele Sanfilici (Department of Psychiatry and Psychotherapy, Ludwig-Maximilian-University, Munich, Germany); Karsten Blume, Dennis Hedderich, Dominika Julkowski, Nathalie Kaiser, Thorsten Lichtenstein, Ruth Milz, Alexandra Nikolaides, Tanja Pilgram, Mauro Seves, and Martina Wassen (Department of Psychiatry and Psychotherapy, University of Cologne, Cologne, Germany); Christina Andreou, Laura Egloff, Fabienne Harrisberger, Ulrike Heitz, Claudia Lenz, Letizia Leanza, Amatya Mackintosh, Renata Smieskova, Erich Studerus, Anna Walter, and Sonja Widmayer (Department of Psychiatry, Psychiatric University Hospital, University of Basel, Basel, Switzerland); Chris Day, Sian Lowri Griffiths, Mariam Iqbal, Mirabel Pelton, Pavan Mallikarjun, Alexandra Stainton, and Ashleigh Lin (Institute for Mental Health and School of Psychology, University of Birmingham, Birmingham, United Kingdom); Alexander Denissoff, Anu Ellilä, Tiina From, Markus Heinimaa, Tuula Ilonen, Päivi Jalo, Heikki Laurikainen, Antti Luutonen, Akseli Mäkela, Janina Paju, Henri Pesonen, Reetta-Liina Säilä, Anna Toivonen, and Otto Turtonen (Department of Psychiatry, University of Turku, Turku, Finland); Sonja Botterweck, Norman Kluthausen, Gerald Antoch, Julian Caspers, Hans-Jörg Wittsack, and Christian Schmidt-Kraepelin (Department of Psychiatry and Psychotherapy, Medical Faculty, Heinrich-Heine University Düsseldorf, Düsseldorf, Germany); Giuseppe Blasi, Giulio Pergola, Grazia Caforio, Leonardo Fazio, Tiziana Quarto, Barbara Gelao, Raffaella Romano, Ileana Andriola, Andrea Falsetti, Marina Barone, Roberta Passiatore, and Marina Sangiuliano (Department of Basic Medical Science, Neuroscience and Sense Organs, University of Bari Aldo Moro, Bari, Italy); Marian Surmann, Olga Bienek, Udo Dannlowski, and Georg Romer (Department of Psychiatry and Psychotherapy, University of Münster, Münster, Germany); Ana Beatriz Solana, Manuela Abraham, and Timo Schirmer (GE Global Research, Inc., Niskayuna, NY, United States); Carlo Altamura, Marika Belleri, Francesca Bottinelli, Adele Ferro, and Marta Re (Department of Neuroscience and Mental Health, Fondazione IRCCS Ca' Granda Ospedale Maggiore Policlinico, Workgroup of Paolo Brambilla, University of Milan, Milan, Italy); Emiliano Monzani and Maurizio Sberna (Programma 2000, Niguarda Hospital, Workgroup of Paolo Brambilla, University of Milan, Milan, Italy); Giampaolo Perna, Maria Nobile, and Alessandra Alciati (San Paolo Hospital, Workgroup of Paolo Brambilla, University of Milan, Milan, Italy); Armando D'Agostino and Lorenzo Del Fabro (Villa San Benedetto Menni, Albese con Cassano, Workgroup of Paolo Brambilla, University of Milan, Milan, Italy); Matteo Balestrieri, Carolina Bonivento, Giuseppe Cabras, and Franco Fabbro (Department of Medical Area, Workgroup of Paolo Brambilla, University of Udine, Udine, Italy); Marco Garzitto and Sara Piccin (IRCCS Scientific Institute E. Medea, Polo FVG, Workgroup of Paolo Brambilla, University of Udine, Udine, Italy); and Dr. Noethen and Dr. Degenhardt (Friedrich-Wilhelms-Universität Bonn, Bonn, Germany).
Funding
PRONIA (Personalized Prognostic Tools for Early Psychosis Management) is a Collaboration Project funded by the EU under the 7th Framework Programme and grant agreement No. 602152.
Conflict of interest
NK reported receiving grants from the European Union (EU) during the conduct of the study and having a patent to US20160192889A1 issued. SR reported receiving grants from the European Commission during the conduct of the study. AR-R reported receiving grants from the EU during the conduct of the study. CA reported receiving non-financial support from Sunovion Pharmaceuticals, Inc. and H. Lundbeck A/S outside the submitted manuscript. JH reported receiving personal fees from Orion Company, Ltd., Otsuka Pharmaceutical Co, Ltd., and H. Lundbeck A/S and European College of Neuropsychopharmacology Congress participation support from Takeda Pharmaceutical Company Limited during the conduct of the study. FS-L reported receiving grants from the Swiss National Foundation during the conduct of the study. CP reported receiving grants from Australian National Health and the Medical Research Council during the conduct of the study and personal fees from H. Lundbeck A/S and Australia Pty Ltd outside the submitted manuscript. RU reported receiving personal fees from Sunovion Pharmaceuticals, Inc, outside the submitted manuscript. EM reported having a patent to US20160192889A1 licensed. TL reported receiving funding from the Koeln Fortune Program/Faculty of Medicine, University of Cologne (No. 370/2020).
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2023.1209485/full#supplementary-material
References
1. Olesen J, Gustavsson A, Svensson M, Wittchen HU, Jonsson B, CDBE2010 study group. The economic cost of brain disorders in Europe. Eur J Neurol. (2012) 19:155–62. doi: 10.1111/j.1468-1331.2011.03590.x
2. Whiteford HA, Degenhardt L, Rehm J, Baxter AJ, Ferrari AJ, Erskine HE, et al. Global burden of disease attributable to mental and substance use disorders: findings from the Global Burden of Disease Study 2010. Lancet. (2013) 382:1575–86. doi: 10.1016/S0140-6736(13)61611-6
3. Charlson FJ, Ferrari AJ, Santomauro DF, Diminic S, Stockings E, Scott JG, et al. Global epidemiology and burden of schizophrenia: findings from the global burden of disease study 2016. Schizophr Bull. (2018) 44:1195–203. doi: 10.1093/schbul/sby058
4. Schneider F, Erhart M, Hewer W, Loeffler LA, Jacobi F. Mortality and medical comorbidity in the severely mentally ill. Dtsch Arztebl Int. (2019) 116:405–11. doi: 10.3238/arztebl.2019.0405
5. Jaaskelainen E, Juola P, Hirvonen N, McGrath JJ, Saha S, Isohanni M, et al. A systematic review and meta-analysis of recovery in schizophrenia. Schizophr Bull. (2013) 39:1296–306. doi: 10.1093/schbul/sbs130
6. Fusar-Poli P, McGorry PD, Kane JM. Improving outcomes of first-episode psychosis: an overview. World Psychiatry. (2017) 16:251–65. doi: 10.1002/wps.20446
7. Fusar-Poli P, Salazar de Pablo G, Correll CU, Meyer-Lindenberg A, Millan MJ, Borgwardt S, et al. Prevention of psychosis: advances in detection, prognosis, and intervention. JAMA Psychiatry. (2020) 77:755–65. doi: 10.1001/jamapsychiatry.2019.4779
8. Schultze-Lutter F, Michel C, Schmidt SJ, Schimmelmann BG, Maric NP, Salokangas RK, et al. EPA guidance on the early detection of clinical high risk states of psychoses. Eur Psychiatry. (2015) 30:405–16. doi: 10.1016/j.eurpsy.2015.01.010
9. Yung AR, Phillips LJ, McGorry PD, McFarlane CA, Francey S, Harrigan S, et al. Prediction of psychosis. A step towards indicated prevention of schizophrenia. Br J Psychiatry Suppl. (1998) 172:14–20. doi: 10.1192/S0007125000297602
10. Schultze-Lutter F, Klosterkötter J, Picker H, Steinmeyer E-M, Ruhrmann S. Predicting First-Episode Psychosis by Basic symptom criteria. Clin Neuropsychiat. (2007) 4:11–22. doi: 10.2174/138161212799316064
11. Fusar-Poli P, Cappucciati M, Borgwardt S, Woods SW, Addington J, Nelson B, et al. Heterogeneity of psychosis risk within individuals at clinical high risk: a meta-analytical stratification. JAMA Psychiatry. (2016) 73:113–20. doi: 10.1001/jamapsychiatry.2015.2324
12. McGlashan TH, Walsh BC, Woods SW. The Psychosis Risk Syndrome: Handbook for Diagnosis and Follow-up. New York, NY: Oxford University Press (2010). p. 256.
13. Fusar-Poli P, Schultze-Lutter F, Cappucciati M, Rutigliano G, Bonoldi I, Stahl D, et al. The dark side of the moon: meta-analytical impact of recruitment strategies on risk enrichment in the clinical high risk state for psychosis. Schizophr Bull. (2016) 42:732–43. doi: 10.1093/schbul/sbv162
14. McLean D, Thara R, John S, Barrett R, Loa P, McGrath J, et al. DSM-IV “criterion A” schizophrenia symptoms across ethnically different populations: evidence for differing psychotic symptom content or structural organization? Cult Med Psychiatry. (2014) 38:408–26. doi: 10.1007/s11013-014-9385-8
15. Larøi F, Luhrmann TM, Bell V, Christian WA, Deshpande S, Fernyhough C, et al. Culture and hallucinations: overview and future directions. Schizophr Bull. (2014) 40:213–20. doi: 10.1093/schbul/sbu012
16. Falukozi E, Addington J. Impact of Trauma on Attenuated Psychotic Symptoms. Psychosis. (2012) 4:203–12. doi: 10.1080/17522439.2011.626867
17. Rosen M, Haidl TK, Ruhrmann S, Vogeley K, Schultze-Lutter F. Sex differences in symptomatology of psychosis-risk patients and in prediction of psychosis. Arch Womens Ment Health. (2020) 23:339–49. doi: 10.1007/s00737-019-01000-3
18. Schultze-Lutter F, Ruhrmann S, Michel C, Kindler J, Schimmelmann BG, Schmidt SJ. Age effects on basic symptoms in the community: A route to gain new insight into the neurodevelopment of psychosis? Eur Arch Psychiatry Clin Neurosci. (2020) 270:311–24. doi: 10.1007/s00406-018-0949-4
19. Schultze-Lutter F, Schimmelmann BG, Flückiger R, Michel C. Effects of age and sex on clinical high-risk for psychosis in the community. World J Psychiatry. (2020) 10:101–24. doi: 10.5498/wjp.v10.i5.101
20. Walger H, Antonucci LA, Pigoni A, Upthegrove R, Salokangas RKR, Lencer R, et al. Basic symptoms are associated with age in patients with a clinical high-risk state for psychosis: results from the PRONIA study. Front Psychiatry. (2020) 11:552175. doi: 10.3389/fpsyt.2020.552175
21. Fusar-Poli P, Cappucciati M, Rutigliano G, Schultze-Lutter F, Bonoldi I, Borgwardt S, et al. At risk or not at risk? A meta-analysis of the prognostic accuracy of psychometric interviews for psychosis prediction. World Psychiatry. (2015) 14:322–32. doi: 10.1002/wps.20250
22. Schultze-Lutter F, Schimmelmann BG, Ruhrmann S, Michel C. “A rose is a rose is a rose”, but at-risk criteria differ. Psychopathology. (2013) 46:75–87. doi: 10.1159/000339208
23. Addington J, Liu L, Buchy L, Cadenhead KS, Cannon TD, Cornblatt BA, et al. North American prodrome longitudinal study (NAPLS 2): the prodromal symptoms. J Nerv Ment Dis. (2015) 203:328–35. doi: 10.1097/NMD.0000000000000290
24. Raballo A, Nelson B, Thompson A, Yung A. The comprehensive assessment of at-risk mental states: from mapping the onset to mapping the structure. Schizophr Res. (2011) 127:107–14. doi: 10.1016/j.schres.2010.12.021
25. Schultze-Lutter F, Michel C, Ruhrmann S, Schimmelmann BG. Prevalence and clinical relevance of interview-assessed psychosis-risk symptoms in the young adult community. Psychol Med. (2018) 48:1167–78. doi: 10.1017/S0033291717002586
26. Theodoridou A, Hengartner MP, Heekeren K, Dvorsky D, Schultze-Lutter F, Gerstenberg M, et al. Influence of demographic characteristics on attenuated positive psychotic symptoms in a young, help-seeking, at-risk population. Early Interv Psychiatry. (2019) 13:53–6. doi: 10.1111/eip.12444
27. Addington J, Schultze-Lutter F. Prodromal phase of psychosis in adolescent women. In Romans S, Seeman MV, editors. Women's Mental Health: A Life Cycle Approach. Philadelphia, PA: Lippincott William & Wilkins (2006). p. 123–132.
28. Waford RN, MacDonald A, Goines K, Novacek DM, Trotman HD, Elaine FW, et al. Demographic correlates of attenuated positive psychotic symptoms. Schizophr Res. (2015) 166:31–6. doi: 10.1016/j.schres.2015.04.035
29. Heitz U, Studerus E, Menghini-Muller S, Papmeyer M, Egloff L, Ittig S, et al. Gender differences in first self-perceived signs and symptoms in patients with an at-risk mental state and first-episode psychosis. Early Interv Psychiatry. (2017) 13:582–88. doi: 10.1111/eip.12528
30. Willhite RK, Niendam TA, Bearden CE, Zinberg J, O'Brien MP, Cannon TD. Gender differences in symptoms, functioning and social support in patients at ultra-high risk for developing a psychotic disorder. Schizophr Res. (2008) 104:237–45. doi: 10.1016/j.schres.2008.05.019
31. Lemos-Giráldez S, Vallina-Fernández O, Fernández-Iglesias P, Vallejo-Seco G, Fonseca-Pedrero E, Paíno-Piñeiro M, et al. Symptomatic and functional outcome in youth at ultra-high risk for psychosis: a longitudinal study. Schizophr Res. (2009) 115:121–9. doi: 10.1016/j.schres.2009.09.011
32. Kotlicka-Antczak M, Pawelczyk T, Podgorski M, Zurner N, Karbownik MS, Pawelczyk A. Polish individuals with an at-risk mental state: demographic and clinical characteristics. Early Interv Psychiatry. (2018) 12:391–99. doi: 10.1111/eip.12333
33. Walder DJ, Holtzman CW, Addington J, Cadenhead K, Tsuang M, Cornblatt B, et al. Sexual dimorphisms and prediction of conversion in the NAPLS psychosis prodrome. Schizophr Res. (2013) 144:43–50. doi: 10.1016/j.schres.2012.11.039
34. Rietschel L, Lambert M, Karow A, Zink M, Müller H, Heinz A, et al. Clinical high risk for psychosis: gender differences in symptoms and social functioning. Early Interv Psychiatry. (2017) 11:306–13. doi: 10.1111/eip.12240
35. Cornblatt BA, Carrión RE, Auther A, McLaughlin D, Olsen RH, John M, et al. Psychosis prevention: a modified clinical high risk perspective from the recognition and prevention (RAP) program. Am J Psychiatry. (2015) 172:986–94. doi: 10.1176/appi.ajp.2015.13121686
36. Schultze-Lutter F, Hubl D, Schimmelmann BG, Michel C. Age effect on prevalence of ultra-high risk for psychosis symptoms: replication in a clinical sample of an early detection of psychosis service. Eur Child Adolesc Psychiatry. (2017) 26:1401–05. doi: 10.1007/s00787-017-0994-y
37. Schimmelmann BG, Michel C, Martz-Irngartinger A, Linder C, Schultze-Lutter F. Age matters in the prevalence and clinical significance of ultra-high-risk for psychosis symptoms and criteria in the general population: Findings from the BEAR and BEARS-kid studies. World Psychiatry. (2015) 14:189–97. doi: 10.1002/wps.20216
38. Michel C, Lerch S, Büetiger JR, Flückiger R, Cavelti M, Koenig J, et al. An ecological momentary assessment study of age effects on perceptive and non-perceptive clinical high-risk symptoms of psychosis. Eur Child Adolesc Psychiatry. (2022) 18:1–12. doi: 10.1007/s00787-022-02003-9
39. Marshall C, Denny E, Cadenhead KS, Cannon TD, Cornblatt BA, McGlashan TH, et al. The content of attenuated psychotic symptoms in those at clinical high risk for psychosis. Psychiatry Res. (2014) 219:506–12. doi: 10.1016/j.psychres.2014.06.023
40. Trask CL, Cohn JR, Paxson AM, Hansen GS, Cicero DC. Form and content of attenuated psychotic symptoms in psychometrically assessed positive and negative schizotypy. Early Interv Psychiatry. (2020) 14:321–29. doi: 10.1111/eip.12856
41. Marshall C, Falukozi E, Albertin M, Zhu H, Addington J. The development of the Content of Attenuated Positive Symptoms Codebook for those at clinical high risk of psychosis. Psychosis. (2011) 4:191–202. doi: 10.1080/17522439.2011.626070
42. Koutsouleris N, Dwyer DB, Degenhardt F, Maj C, Urquijo-Castro MF, Sanfelici R, et al. Multimodal machine learning workflows for prediction of psychosis in patients with clinical high-risk syndromes and recent-onset depression. JAMA Psychiatry. (2021) 78:195–209. doi: 10.1001/jamapsychiatry.2020.3604
43. Koutsouleris N, Kambeitz-Ilankovic L, Ruhrmann S, Rosen M, Ruef A, Dwyer DB, et al. Prediction models of functional outcomes for individuals in the clinical high-risk state for psychosis or with recent-onset depression: a multimodal, multisite machine learning analysis. JAMA Psychiatry. (2018) 75:1156–72. doi: 10.1001/jamapsychiatry.2018.2165
44. Deutsche Gesellschaft für Psychitrie. Psychotherapie und Nervenheilkunde (DGPPN). S3 Praxisleitlinien in Psychiatrie und Psychotherapie. Band 1: Behandlungsleitlinie Schizophrenie. Heidelberg: Steinkopff (2006). p. 288.
45. Schultze-Lutter F, Walger P, Franscini M, Traber-Walker N, Osman N, Walger H, et al. Clinical high-risk criteria of psychosis in 8-17-year-old community subjects and inpatients not suspected of developing psychosis. World J Psychiatry. (2022) 12:425–49. doi: 10.5498/wjp.v12.i3.425
46. Schultze-Lutter F, Addington J, Ruhrmann S, Klosterkötter J. Schizophrenia Proneness Instrument, Adult version (SPI-A). Rome, Italy: Giovanni Fioriti Editore SRl (2007). p. 97.
47. Schultze-Lutter F, Theodoridou A. The concept of basic symptoms: its scientific and clinical relevance. World Psychiatry. (2017) 16:104–05. doi: 10.1002/wps.20404
48. First MB, Spitzer RL, Gibbon M, William JBW. Structured Clinical Interview DSM-IV-TR Axis I Disorders, Research Version, Patient Edition. (SCID-I/P). New York: Biometrics Research, New York State Psychiatric Institute (2002). p. 84.
49. Auther AM, Smith CW, Cornblatt BA. Global Functioning: Social Scale (GF: Social). Glen Oaks, NY: Zucker Hillside Hospital. (2006).
50. Niendam TA, Bearden CE, Johnson JK. & Cannon TD. Global Functioning: Role Scale (GF: Role). Los Angeles, CA: University of California, Los Angeles. (2006).
51. Fox F. Applied Regression Analysis and Generalized Linear Models, 3rd Ed. London: Sage Publications. (2016). p. 816.
52. Cri?an C, Androne B, Barbulescu LD, Suciu BD. Nexus of delusions and overvalued ideas: a case of comorbid schizophrenia and anorexia in the view of the new ICD-11 classification system. Am J Case Rep. (2022) 23:933759. doi: 10.12659/AJCR.933759
53. Marshall C, Deighton S, Cadenhead KS, Cannon TD, Cornblatt BA, McGlashan TH, et al. The violent content in attenuated psychotic symptoms. Psychiatry Res. (2016) 242:61–6. doi: 10.1016/j.psychres.2016.05.005
54. Torgersen S, Kringlen E, Cramer V. The prevalence of personality disorders in a community sample. Arch Gen Psychiatry. (2001) 58:590–6. doi: 10.1001/archpsyc.58.6.590
55. Coid J, Yang M, Tyrer P, Roberts A, Ullrich S. Prevalence and correlates of personality disorder in Great Britain. Br J Psychiatry. (2006) 188:423–31. doi: 10.1192/bjp.188.5.423
56. Pulay AJ, Stinson FS, Dawson DA, Goldstein RB, Chou SP, Huang B, et al. Prevalence, correlates, disability, and comorbidity of DSM-IV schizotypal personality disorder: results from the wave 2 national epidemiologic survey on alcohol and related conditions. Prim Care Companion J Clin Psychiatry. (2009) 11:53–67. doi: 10.4088/PCC.08m00679
57. Armando M, Nelson B, Yung AR, Ross M, Birchwood M, Girardi P, et al. Psychotic-like experiences and correlation with distress and depressive symptoms in a community sample of adolescents and young adults. Schizophr Res. (2010) 119:258–65. doi: 10.1016/j.schres.2010.03.001
58. Fonseca-Pedrero E, Chan RCK, Debbané M, Cicero D, Zhang LC, Brenner C, et al. Comparisons of schizotypal traits across 12 countries: results from the international consortium for schizotypy research. Schizophr Res. (2018) 199:128–34. doi: 10.1016/j.schres.2018.03.021
59. Schultze-Lutter F, Kindler J, Ambarini TK, Michel C. Positive psychotic symptoms in childhood and adolescence. Curr Opin Psychol. (2022) 45:101287. doi: 10.1016/j.copsyc.2021.11.007
60. Schimmelmann BG, Schultze-Lutter F. Early detection and intervention of psychosis in children and adolescents: urgent need for studies. Eur Child Adolesc Psychiatry. (2012) 21:239–41. doi: 10.1007/s00787-012-0271-z
61. Fagerlund B, Pantelis C, Jepsen JRM, Raghava JM, Rostrup E, Thomas MB, et al. Differential effects of age at illness onset on verbal memory functions in antipsychotic-naïve schizophrenia patients aged 12-43 years. Psychol Med. (2021) 51:1570–80. doi: 10.1017/S0033291720000409
62. Grover S, Davuluri T, Chakrabarti S. Religion, spirituality, and schizophrenia: a review. Indian J Psychol Med. (2014) 36:119–24. doi: 10.4103/0253-7176.130962
63. Huang CL, Shang CY, Shieh MS, Lin HN, Su JC. The interactions between religion, religiosity, religious delusion/hallucination, and treatment-seeking behavior among schizophrenic patients in Taiwan. Psychiatry Res. (2011) 187:347–53. doi: 10.1016/j.psychres.2010.07.014
64. Zhang T, Yang S, Xu L, Tang X, Wei Y, Cui H, et al. Poor functional recovery is better predicted than conversion in studies of outcomes of clinical high risk of psychosis: insight from SHARP. Psychol Med. (2020) 50:1578–84. doi: 10.1017/S0033291719002174
65. Cannon TD, Yu C, Addington J, Bearden CE, Cadenhead KS, Cornblatt BA, et al. An individualized risk calculator for research in prodromal psychosis. Am J Psychiatry. (2016) 173:980–88. doi: 10.1176/appi.ajp.2016.15070890
66. Goldman HH, Skodol AE, Lave TR. Revising axis V for DSM-IV: a review of measures of social functioning. Am J Psychiatry. (1992) 149:1148–56. doi: 10.1176/ajp.149.9.1148
67. Samara MT, Engel RR, Millier A, Kandenwein J, Toumi M, Leucht S. Equipercentile linking of scales measuring functioning and symptoms: examining the GAF, SOFAS, CGI-S, and PANSS. Eur Neuropsychopharmacol. (2014) 24:1767–72. doi: 10.1016/j.euroneuro.2014.08.009
68. Oeztuerk OF, Pigoni A, Antonucci LA, Koutsouleris N. Association between formal thought disorders, neurocognition and functioning in the early stages of psychosis: a systematic review of the last half-century studies. Eur Arch Psychiatry Clin Neurosci. (2022) 272:381–93. doi: 10.1007/s00406-021-01295-3
69. Hernández LM, Kemp KC, Barrantes-Vidal N, Kwapil TR. Replication of the associations of positive, negative, and disorganized schizotypy with interview-assessed symptoms and impairment: Convergence with previous studies. Personal Disord. (2023) 2:11. doi: 10.1037/per0000611
70. Mohr C, Claridge G. Schizotypy – do not worry, it is not all worrisome. Schizophr Bull. (2015) 41:436–43. doi: 10.1093/schbul/sbu185
71. Sorensen DJ, Paul GL, Mariotto MJ. Inconsistencies in paranoid functioning, premorbid adjustment, and chronicity: question of diagnostic criteria. Schizophr Bull. (1988) 14:323–36. doi: 10.1093/schbul/14.2.323
72. Fett AJ, Hanssen E, Eemers M, Peters E, Shergill SS. Social isolation and psychosis: an investigation of social interactions and paranoia in daily life. Eur Arch Psychiatry Clin Neurosci. (2022) 272:119–27. doi: 10.1007/s00406-021-01278-4
73. Rakhshan Rouhakhtar P, Roemer C, Reeves G, Schiffman J. The associations between attenuated psychosis symptoms and functioning in Black and White youth at clinical high-risk for psychosis. Schizophr Res. (2023) 253:40–7. doi: 10.1016/j.schres.2021.11.032
74. Fusar-Poli P, Nelson B, Valmaggia L, Yung AR, McGuire PK. Comorbid depressive and anxiety disorders in 509 individuals with an at-risk mental state: impact on psychopathology and transition to psychosis. Schizophr Bull. (2014) 40:120–31. doi: 10.1093/schbul/sbs136
75. Rasmussen AR, Parnas J. What is obsession? Differentiating obsessive-compulsive disorder and the schizophrenia spectrum. Schizophr Res. (2022) 243:1–8. doi: 10.1016/j.schres.2022.02.014
76. West B, Willner P. Magical thinking in obsessive-compulsive disorder and generalized anxiety disorder. Behav Cogn Psychother. (2011) 39:399–411. doi: 10.1017/S1352465810000883
77. Bocci L, Gordon PK. Does magical thinking produce neutralising behaviour? An experimental investigation. Behav Res Ther. (2007) 45:1823–33. doi: 10.1016/j.brat.2007.02.003
78. Pozza A, Dèttore D. “Was it real or did I imagine it?” Perfectionistic beliefs are associated with dissociative absorption and imaginative involvement in obsessive-compulsive disorder. Psychol Res Behav Manag. (2019) 12:603–07. doi: 10.2147/PRBM.S212983
79. Soffer-Dudek N. Daily elevations in dissociative absorption and depersonalization in a nonclinical sample are related to daily stress and psychopathological symptoms. Psychiatry. (2017) 80:265–78. doi: 10.1080/00332747.2016.1247622
Keywords: Attenuated Psychotic Symptoms, delusional ideas, hallucinatory experiences, disorganized communication, clinical-high risk for psychosis
Citation: Theisen C, Rosen M, Meisenzahl E, Koutsouleris N, Lichtenstein T, Ruhrmann S, Kambeitz J, Kambeitz-Ilankovic L, Riecher-Rössler A, Chisholm K, Upthegrove R, Antonucci LA, Bertolino A, Pigoni A, Salokangas RKR, Pantelis C, Wood SJ, Lencer R, Falkai P, Hietala J, Brambilla P, Schmidt A, Andreou C, Borgwardt S, Osman N and Schultze-Lutter F (2023) The heterogeneity of attenuated and brief limited psychotic symptoms: association of contents with age, sex, country, religion, comorbidities, and functioning. Front. Psychiatry 14:1209485. doi: 10.3389/fpsyt.2023.1209485
Received: 20 April 2023; Accepted: 13 June 2023;
Published: 07 July 2023.
Edited by:
Stefano Barlati, University of Brescia, ItalyReviewed by:
Pasquale Pezzella, University of Campania Luigi Vanvitelli, ItalyLex Wunderink, University Medical Center Groningen, Netherlands
Marta Bosia, Vita-Salute San Raffaele University, Italy
Vishal Girishkumar Bhavsar, King's College London, United Kingdom
Copyright © 2023 Theisen, Rosen, Meisenzahl, Koutsouleris, Lichtenstein, Ruhrmann, Kambeitz, Kambeitz-Ilankovic, Riecher-Rössler, Chisholm, Upthegrove, Antonucci, Bertolino, Pigoni, Salokangas, Pantelis, Wood, Lencer, Falkai, Hietala, Brambilla, Schmidt, Andreou, Borgwardt, Osman and Schultze-Lutter. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Christian Theisen, Christian.theisen@hhu.de