 Joanna Dymecka
Joanna Dymecka Rafał Gerymski
Rafał Gerymski Anna Machnik-Czerwik
Anna Machnik-Czerwik Romuald Derbis2
Romuald Derbis2 Mariola Bidzan
Mariola Bidzan- 1Department of Health Psychology and Quality of Life, Institute of Psychology, Opole University, Opole, Poland
- 2Department of General and Work Psychology, Institute of Psychology, Opole University, Opole, Poland
- 3Department of Clinical and Health Psychology, Institute of Psychology, University of Gdańsk, Gdańsk, Poland
Introduction: The COVID-19 pandemic is contributing to increased fear and anxiety throughout society, which may affect life satisfaction. Health-related hardiness and sense of coherence (SOC) are personal resources that help people adapt to difficult circumstances. The purpose of this study was to investigate the relationship between fear of COVID-19, SOC, health-related hardiness, and life satisfaction.
Methods: A total of 907 Polish people (522 women and 385 men) participated in this study. The Fear of COVID-19 Scale (FOC-6), the Health-Related Hardiness Scale, the Sense of Coherence Scale (SOC-29), and the Satisfaction with Life Scale were used.
Results: Correlation showed that fear of COVID-19 was negatively related to health-related hardiness, SOC, and life satisfaction. Health-related hardiness and SOC were positively related to life satisfaction. Both SOC and hardiness were mediators between fear of COVID-19 and life satisfaction during the current pandemic.
Conclusion: SOC and health-related hardiness are personal resources that are important for dealing with the effects of the COVID-19 pandemic. According to our study, SOC and hardiness can mediate between fear of COVID-19 and life satisfaction. Presented cross-sectional results have to be verified in future longitudinal studies in order to strengthen the conclusions presented in this manuscript. This study verified the role of only two personal resources, so more research is needed on the role of other personal resources during COVID-19 pandemic.
Introduction
For over a year, the entire world has been struggling with a global pandemic caused by the spread of the SARS-CoV-2 coronavirus, which appeared in the city of Wuhan, Hubei province, China in late 2019. In early 2020, the disease caused by the virus was called COVID-19 and, on March 11, 2020, the WHO declared it a global pandemic. It is the largest pandemic to affect humans so far in the twenty first century. The clinical course of the disease varies from mild or even asymptomatic to severe respiratory failure and death. The prognosis is worse in the elderly and patients with comorbidities (1–3). According to the World Health Organization (4), more than 126 million people in the world have been infected and more than 2.8 million have died. The first case of COVID-19 in Poland was recorded on March 4, 2020, and by March 28, 2021, almost 2.2 million people were infected and more than 51,000 have died.
COVID-19, like other contagious diseases which cause epidemics, affects not only physical health but also mental functioning. The changes in everyday life caused by the pandemic were rapid and unprecedented. COVID-19, as a global threat to public health, requires drastic control measures and has disrupted almost every aspect of everyday life. The rapid increase in confirmed cases and deaths, isolation, reduced social contact, school and workplace closures, and significant restrictions on activity and freedoms can all be stressful for society as a whole (5, 6). Even if most people are not infected and remain physically well, they often suffer from the negative psychological effects of the epidemic.
An infectious disease pandemic can also affect life satisfaction, which is an individual's cognitive evaluation of their life (7). Many previous studies have shown that experiencing difficult life situations has a negative impact on human health and well-being (8). Several studies have shown that the pandemic affects well-being and life satisfaction (6, 9–11). A Turkish study showed that fear of COVID-19 decreases life satisfaction (12), while Harper et al. (10) indicated that fear of COVID-19 reduces individuals' well-being.
A contagious disease pandemic increases fear and anxiety throughout society, as can be observed in both the current and previous epidemics (13). During the current COVID-19 pandemic, people fear becoming infected, dying or losing loved ones, and contact with people who might be infected (6, 14, 15). Fear is an adaptive protective mechanism for animals and humans that is fundamental to survival and involves several biological processes related to preparing to respond to potentially dangerous events. However, when it is chronic or disproportionate, it can cause mental disorders (16). Ahorsu et al. (17) indicated that fear of COVID-19 increases levels of psychological distress and has a negative impact on mental health. Constant information about the many fatalities around the world and the growing number of cases lead to increased fear of COVID-19, causing people to experience stress, anxiety, and mood disorders, which have a negative impact on their psychological well-being (12, 18). Coronavirus threatens one's safety and desire to survive, which affects quality of life. Therefore, fear of COVID-19 reduces people's well-being and decreases their life satisfaction (19, 20). However, Özmen et al. (19) showed that fear of COVID-19 explains only a small percentage of the variation in life satisfaction.
Hardiness is usually defined as a generalized style of functioning characterized by a high level of commitment, control, and challenge, thanks to which the negative effects of stress are mitigated. People with a high level of hardiness believe that they have control over their life and that through their commitment to their goals they will achieve positive results. They treat everyday stressors as challenges (21). The research showed that people characterized by a high level of hardiness were protected against the negative impact of stress on their life and health (22, 23).
Sense of coherence (SOC) is defined as “a global orientation that expresses the extent to which one has a pervasive, enduring though dynamic feeling of confidence that (1) the stimuli deriving from one's internal and external environments in the course of living are structured, predictable and explicable; (2) the resources are available to one to meet the demands posed by these stimuli; and (3) these demands are challenges, worthy of investment and engagement” (24).
Antonovsky (24) in his works drew attention to the relationship between SOC and hardiness. Both postulate the existence of complex personality traits that act as personal resources in stressful situations (24, 25). Also, the mechanisms by which SOC and hardiness affect physical and mental health seem to be similar (26). Therefore, many studies conducted on various populations indicate a relationship between SOC and psychological hardiness (26–28).
SOC seems to be a particularly important resource for dealing with the pandemic. Many studies have shown that high levels of SOC make it easier to accept inevitable difficulties (29, 30). Also, SOC is particularly necessary when strong stressors affect an individual (31), as in the case in the ongoing pandemic. Studies have also shown that a strong SOC is negatively associated with anxiety, perceived stress, and its consequences (32). People with a strong SOC can more effectively deal with adverse circumstances (33). SOC and hardiness are also resources that affect quality of life. The role of SOC as a significant predictor of quality of life has been demonstrated in many previous studies and analyses that found that higher SOC is linked with better quality of life (34–36). Also, hardiness can improve individuals' well-being and increase life satisfaction (37). Many studies on different populations have shown that hardiness is positively related to quality of life (28, 38) and life satisfaction (39).
Several studies conducted during the COVID-19 pandemic have shown that hardiness is a very important resource for dealing with adverse events stemming from COVID-19 (40, 41). Hardiness enables us to perform and to stay focused during hard times. It helps people to adapt to new situations and withstand adversity (21). Hardiness plays a protective role by reducing the risk of dysfunctional stress reactions occurring in emergency workers during the current COVID-19 pandemic (42). Importantly, it has also been shown that hardiness is positively related to individuals' well-being during the current pandemic (43).
In addition, many studies on different populations have shown that SOC and hardiness act as mediators in the relationships between a variety of variables (29, 30, 44–48). SOC has been found to mediate the relationship between adverse experiences and psychological well-being (29), and to mediate between symptoms, stress, coping, and life satisfaction (49). Hardiness has been found to be a mediator between stress and illness (50). Hardiness has been found to act as a mediator of the relationship between traumatic experiences and post-traumatic adaptation (51). Therefore, it can be assumed that SOC and hardiness will be mediators of the relationship between fear of COVID-19 and life satisfaction during the global pandemic.
The Present Study
The purpose of this study was to investigate the relationship between fear of COVID-19, SOC, health-related hardiness, and life satisfaction. Based on the information presented in the introduction, we decided to investigate whether: (1) fear of COVID-19 is significantly and negatively associated with SOC and hardiness; (2) SOC and hardiness are significantly and positively associated with life satisfaction; and (3) SOC and hardiness are mediators in the relationship between fear of COVID-19 and life satisfaction.
Materials and Methods
Participants
A total of 907 Polish people (522 women and 385 men) participated in this study. The average age of all respondents was 39.28 years. Above half of the study participants had university level education. The second largest group were people with high school education. The smallest number of respondents had elementary and vocational education. About half of the studied sample represented people living in towns. The obtained number of people living in cities and villages was relatively equal. About 70% of the participants in this study were employed. We didn't verify the reasons of unemployment of the rest of the participants. The level of other sociodemographic variables has not been investigated. Detailed sociodemographic data of the studied sample were presented in Table 1.
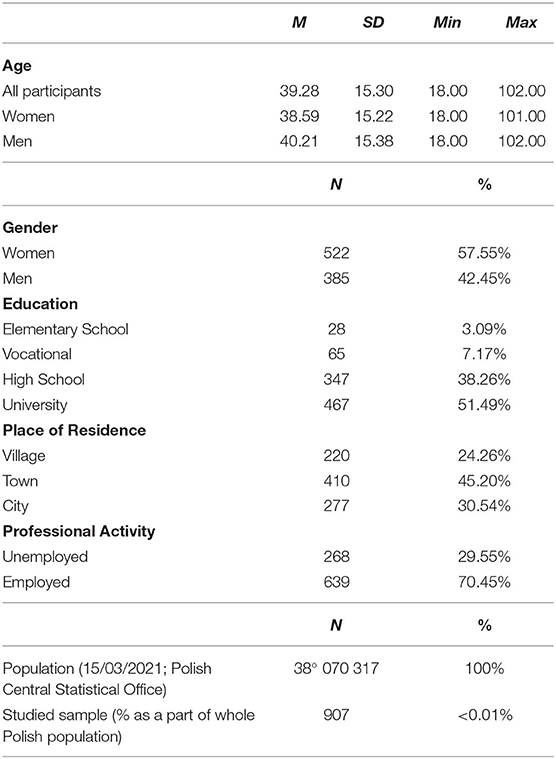
Table 1. Characteristics of the studied sample (N = 907).
Procedure
The recruitment of the study participants was carried out using the snowball method. Due to the pandemic, every effort was made to ensure that the study was completely safe for its participants. Therefore, we recruited respondents via the Internet. The recruitment of the participants took place between March and May of 2020. Study assistants were asked to share the survey on social media platforms. All people under 18 years of age were excluded from the analysis. Digitally excluded older adults were able to complete the survey by phone (n = 11). The study participants were informed about the anonymity of the study. They could stop filling out the survey at any time and without giving any reason. All respondents gave informed consent to participate in this study. The presented project adhered to the guidelines of the Bioethics Committee of the University of Opole.
Measures
Fear of the coronavirus was measured with the Fear of COVID-19 Scale (FOC-6) (6). Respondents answered the questions using a five-point scale (1— “definitely disagree”; 5— “completely agree”). Higher FOC-6 scores indicate higher fear of COVID-19. FOC-6 is a reliable questionnaire (Cronbach's alpha = 0.83; McDonald's total omega = 0.84). Confirmatory Factor Analysis indicates that the obtained model fit values are mostly acceptable (CFI = 0.957; TLI = 0.928; RMSEA = 0.111). After setting the error covariance between items 1 and 2 (which is theoretically justified due to the semantic similarity of those items), FOC-6 model fit coefficients improve (CFI = 0.984, TLI = 0.969, RMSEA = 0.072). Confirmatory Factor Analysis (CFA) results show acceptable model fit coefficient values for the tested 6-items one-factor model. Unfortunately, FOC-6 wasn't developed with the usage of the Exploratory Factor Analysis (EFA). Although the results of the post-hoc EFA based on Oblimin rotation with the usage of Maximum Likelihood extraction method confirm the results of the CFA analysis (one-factor model where all factor loadings exceed the value of 0.60), it cannot be certain that the structure would be the same as if EFA had been used during the questionnaire validation process. What is more, FOC-6 validity wasn't verified with relation to other fear of COVID-19 related scales, but it can be supported by the fact, that it's results are significantly related to other similar variables, such as stress or well-being measures (6).
The Sense of Coherence Scale (SOC-29) (52), adapted by Koniarek et al. (53), was also used in this study. The questionnaire consists of 29 items related to various aspects of human life. The study participants responded to them on a seven-point scale. The questionnaire is used to study global SOC and its three components: the senses of comprehensibility, manageability, and meaningfulness. Only the global score was used in this study. The scale shows good reliability (in this study Cronbach's α was 0.91). Higher SOC-29 scores indicate higher SOC.
Hardiness was measured with the short version of the Health-Related Hardiness Scale (HRHS) by Pollock (54), in its Polish adaptation by Dymecka et al. (28). It contains 12 items that participants assess on a six-point Likert scale, where 1 indicates complete disagreement and 6 indicates complete agreement. The scale shows good reliability (in this study Cronbach's α was 0.78). Higher HRHS scores indicate higher hardiness.
The Satisfaction with Life Scale (SWLS) (7), adapted by Juczyński (55), was also used. It consists of five questions on a seven-point scale (1— “definitely disagree”; 4— “neither agree nor disagree”; 7— “completely agree”). The scale shows good reliability (in this study Cronbach's α was 0.87). Higher SWLS scores indicate higher life satisfaction.
Statistical Analysis
In order to verify the formulated hypotheses, a number of statistical analyses were used. The significance of the relationship between fear of COVID-19, hardiness, SOC and life satisfaction was tested with Pearson's r correlation analysis. It allowed us to verify the two-sided relationships between tested variables. Before analyzing the mediational role of hardiness and SOC in the relationship between fear of COVID-19 and life satisfaction, we decided to verify if the residuals autocorrelation and multicollinearity between hardiness and SOC may have occurred. Therefore, Durbin-Watson test and Variable Inflation Factors analysis were used. One-sided relationships and indirect effects of the possible mediators were verified with mediation analysis using MODEL 4 of PROCESS v3.4 macro (56). Additionally, we decided to perform a post-hoc power analysis in order to check whether the obtained sample allows conclusions from the presented data. For that purpose, we used the Monte Carlo simulation (57) performed in the R environment (58). A significance level of α = 0.05 was adopted as the threshold value for statistical significance in all analyses, which is a standard practice in the presented field of research. Bootstrapping mediation using the PROCESS macro was performed with 5,000 samples (59).
Results
Correlation Analysis
In the first step of the statistical analysis, it was decided to check whether there were any significant relationships between the tested variables. In order to select an appropriate analysis, it was checked whether the distributions of the examined variables showed large asymmetry. Skewness and kurtosis statistics showed that the studied distributions did not show large asymmetry. On this basis, a parametric Pearson's r correlation analysis was performed. Pearson's r correlation showed significant relationship between fear of COVID-19, health-related hardiness, SOC, and life satisfaction. Relationship between fear of COVID-19 and other variables was negative and weak. What is more, health-related hardiness was positively and moderately related to SOC, and life satisfaction. More detailed data are shown in Table 2.

Table 2. Results of Pearson's r correlation analysis (N = 907).
Mediation Analysis
In the next step, it was decided to perform a mediation analyses due to the significant relationships found using the Pearson's r correlation analysis. Before calculating the mediation analyses, it was decided to verify if the tested residuals are correlated. Durbin-Watson test results showed, that the residuals were not correlated in the verified model. Based on the small asymmetry of the studied distributions and the lack of autocorrelation, it was decided to perform the mediation analysis as planned. Two separate MODEL 4 mediation analyses were performed, because the analysis of Variable Inflation Factors suggested that multicollinearity between hardiness and SOC may have occurred (VIF > 10).
First, it was examined whether hardness mediates the relationship between fear of COVID-19 and life satisfaction. The second model tested whether SOC was a mediator in the relationship between fear of COVID-19 and life satisfaction. The PROCESS macro results showed that all investigated mediation paths were statistically significant. Analysis of the confidence intervals of the indirect effects suggests, that health-related hardiness and SOC mediated the relationship between stress and life satisfaction. More detailed data is shown in Table 3.
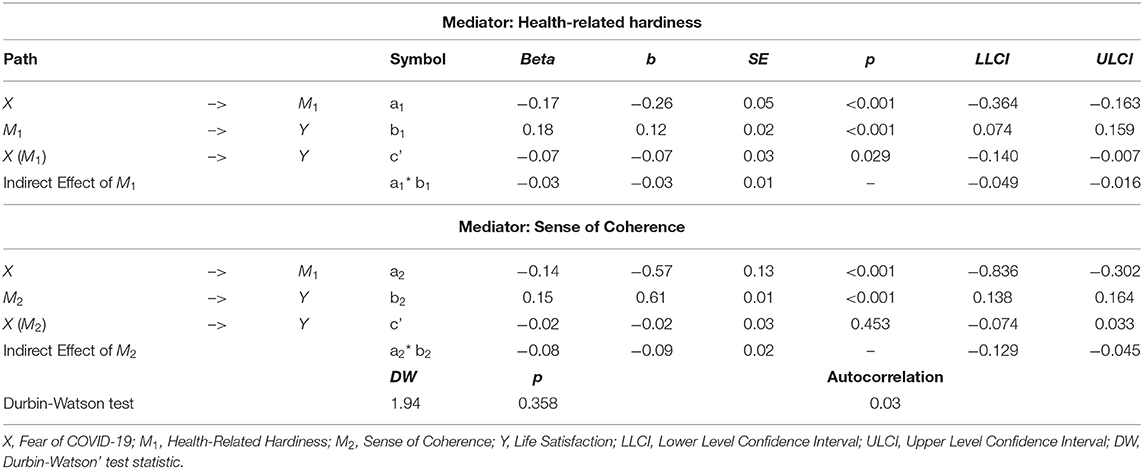
Table 3. Detailed data of the results of the PROCESS MODEL 4 analysis (N = 907).
Power Analysis
Monte Carlo simulation (57) with 5,000 replications and 20,000 Monte Carlo draws was performed at the confidence level of 95%. The simulation confirmed the power obtained at the level of at least 0.98 for both mediation models.
Discussion
This study aimed to determine the relationship between fear of COVID-19, SOC, health-related hardiness, and life satisfaction during the coronavirus pandemic. Presented results show that fear of coronavirus was negatively linked to life satisfaction of the studied sample. Our results are consistent with previous studies, which show that pandemic situation can negatively affect our life satisfaction (6, 9–11). There are multiple possible explanations of this significant result. In the COVID-19 pandemic, fear of infection, death, and loss of loved ones are common, which leads to increased distrust of others, avoidance, and withdrawal from everyday activities (60). At the beginning of the pandemic, we all had to adapt to new living conditions, which could produce a sense of uncertainty related to the development of the epidemiological situation. An increase of anxiety during a pandemic is a natural reaction. It can cause high levels of stress, which has a negative impact on our well-being. Even though our study did not verify the role of social support, it is possible that pandemic opportunities for interpersonal contact, resulting in disruption of social support networks at the time when they may be most needed (61), because, as is known, social support is crucial for adaptive functioning (15, 62).
The current study showed also a negative correlation between fear of COVID-19 and two personal resources: health-related hardiness and SOC. In line with theoretical assumptions, the present study found a correlation between SOC and psychological hardiness. Both SOC and hardiness were mediators between fear of COVID-19 and life satisfaction during the current pandemic. According to theory, hardiness can affect perceptions of stressful events (63). In the current pandemic situation, people with high levels of hardiness may be confident that they will be able to protect themselves from infection or, in the event of infection, be able to deal with it effectively (64). It can therefore be assumed that they will cope better with the fear of COVID-19. The tension caused by a pandemic may not turn into distress and they will be less likely to experience its negative consequences, such as anxiety or depression. Thanks to this, despite difficult circumstances, they might judge their life as satisfactory. It is possible because hardy people adapt more easily to difficult life situations such as the pandemic. Also, people with high levels of hardiness become engaged in what they do, don't feel alienated, usually believe that they can at least partially control what happens to them, do not feel powerless, and treat changes as challenges and opportunities for development, rather than as threats (65). Hardiness is related to the tendency to perceive stressful life events as less serious, less dangerous, and more manageable (21, 66).
SOC can play an equally important role in the process of dealing with the COVID-19 pandemic. SOC can, by effectively managing stress and reducing levels of anxiety, affect psychological well-being and quality of life (67, 68). In his salutogenic theory, Antonovsky (24) repeatedly emphasized the role of SOC in an individual's coping with difficult situations, because, in his opinion, SOC reduces the likelihood of strong tension turning into stress, which is extremely important during a pandemic. A person with a strong SOC sees the world as orderly and understandable, and finds order in the environment, helping them to better cope with chaotic stimuli. A strong SOC can allow a person to approach difficult situations as challenges rather than obstacles. A high SOC is also associated with an appropriate response to emotional stimuli, with low sensitivity to them and high emotional resilience. People with strong SOC seek information only when they need it to solve a problem, and not when it causes overload (24), which is particularly important during the current pandemic, as excessive focus on negative information provided in the media can lead to increased anxiety (69). In a situation where the problem cannot be solved, people with a high SOC can adapt better and thus suffer less. Another important role of SOC is to influence the emotions experienced in difficult situations. SOC may limit the experience of negative emotions in stressful situations, which is particularly important in dealing with fear of COVID-19. People with a strong SOC experience emotions consciously and they can provide a motivational basis for action (70). Therefore, the SOC's mediational role between fear of COVID-19 and life satisfaction seems theoretically justified and was empirically verified in the presented study.
The results obtained in the present study were also confirmed in previous studies. Research suggests that constant information about confirmed deaths and the growing number of cases increased levels of fear of COVID-19, which had a negative impact on life satisfaction (12). Health-related fear, decreased availability of social support, and the curtailment of typical recreational activities have diminished well-being and life satisfaction throughout society (71). The link between the fear of COVID-19 and hardiness was also confirmed in previous studies. In Russian research, it was shown that low levels of hardiness were associated with high levels of fear of COVID-19 (72). A negative relationship between hardiness and negative emotions such anxiety and depression has already been demonstrated in many previous studies (73–78). Studies conducted during the COVID-19 pandemic have shown that psychological hardiness is negatively correlated with anxiety, depression, and the general severity of psychopathological symptoms. Therefore, we believe that hardiness can be associated with changes in anxiety levels during the pandemic. People with lower hardiness show increased anxiety over time (71). Studies have shown that the lower the hardiness level, the greater the assessment of the negative aspects of COVID-19. For people with low levels of hardiness, the pandemic may be a source of stress that affects their quality of life (72), which is a possible explanation of the presented results.
In many studies on various populations, it has been found that SOC was negatively correlated with levels of fear, stress, and anxiety (67, 79). In previous studies, SOC was associated with lower emotional tension and lower levels of situational anxiety (70). The relationship between SOC and hardiness has also been documented in other empirical works (26–28, 80). Studies suggest that psychological hardiness is an important resource for coping with the COVID-19 threat (41). One Russian study found hardiness to be a personal adaptive resource in stressful situations related to the COVID-19 pandemic (71). We believe that people with high levels of hardiness might interpret stressful life events as being less difficult (21). Hardiness contributes to perceiving the pandemic as a challenge. High levels of hardiness can help a person control anxiety and irrational thoughts. This resource prevents unpleasant emotions and thoughts, which have a negative effect on various stress factors and secondary trauma (42).
Studies have shown that people with high hardiness have better quality of life and are more energetic and optimistic (81). In studies among elderly people, it has been shown that higher levels of psychological hardiness are associated with greater life satisfaction (39). Hardiness protects one's well-being in the face of negative life events (21). It prevents the deterioration of psychological well-being in stressful situations (71). This is why research has shown that psychological hardiness is positively related to well-being during the COVID-19 pandemic (43). This was also confirmed in our study, which showed a positive relationship between hardiness and life satisfaction during the COVID-19 pandemic.
The relationship between SOC and life satisfaction has been demonstrated in many empirical studies (82–85). Data from empirical studies confirm that SOC can affect life satisfaction, acceptance of inevitable difficulties, and sense of control of situations. Many empirical studies have confirmed the relationship between SOC and subjective well-being, quality of life, and satisfaction with life (83). SOC helps one perceive the disease as less threatening (86). A strong SOC is particularly important when an individual experiences very difficult situations (31, 87), and the pandemic is undoubtedly one such situation. Many studies have also confirmed the role of SOC as an important mediator of the relationship between a variety of variables, including life satisfaction, as demonstrated in the present study. SOC has been shown to be a mediator between stress and life satisfaction during the COVID-19 pandemic (82). Another study on found that the relationship between adversity—indicated by the occurrence of worry, anxiety, and stress—and life satisfaction can be explained by the significant mediation of SOC (29). SOC can act as a protective factor in the process of adaptation to difficult life events (49), and the mediation path found in this study can help us understand how it does so. Other study results indicate that SOC can explain more variance in many areas of quality of life than any other variable (88). Therefore, we believe that this might be a possible explanation why SOC played as a significant mediator in the relationship between fear of COVID-19 and life satisfaction.
Although our study produced important results, it is not free of limitations. Although our mediation model is tested as causal, it does not allow us to establish cause and effect relationships, since our data are cross-sectional. It would require longitudinal studies to confirm whether the proposed direction of the influence is correct. Additionally, recruiting study participants via social media is an example of convenience sampling. Such sample does not have sufficient power to detect sociodemographic group differences, which makes it limiting in the case of statistical analyses that can be used (89). Therefore, another study based on population-based sampling should be performed in order to confirm the proposed mediation model and possible group differences. Lastly, this study verified the role of fear of COVID-19 with a FOC-6 questionnaire. Although it is a reliable scale, its model fit coefficient values are acceptable at best. Additionally, FOC-6 was validated without the usage of Exploratory Factor Analysis. Next studies should be performed with a scale representing better psychometric properties, such as FCV-19S (17). FCV-19S wasn't used in the presented study due to the fact, that it started before FCV-19S was yet available. Also, the validity of FOC-6 should be verified by correlating its results with the results of the FCV-19S scale.
Previous studies have shown that SOC and health-related hardiness are personal resources that are important in the current COVID-19 pandemic. The increasing number of infections, the millions of people who have lost their lives, and the inefficiency of health care systems are leading to increased fear. Resources such as SOC and psychological hardiness can mediate the effects of fear on life satisfaction. That assumption was positively verified in the presented manuscript. Research on hardiness and SOC in COVID-19 pandemic is very important, because people with a high level of personal resources may experience greater satisfaction with life despite the duration of the pandemic. For these people, fear might be less paralyzing, and they may view the pandemic situation as a challenge rather than a burden. Both resources facilitate dealing with difficulties by changing the way one relates and reacts to events outside one's control. The idea is not to try to change or divert attention from the problem of the pandemic, because the virus is a real threat and there are objective reasons to be afraid of it, but fear does not have to dominate one's existence. People with strong SOC and hardiness can function with realistic fears and relate to them in an adaptive manner (62). Therefore, when working with people experiencing the psychological consequences of the pandemic, it is worth considering their personal resources and to work on developing these resources.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by University Research Ethics Committee at the University of Opole. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
JD: conceptualization, project administration, writing, and original draft preparation. RG: methodology, formal analysis, writing, and original draft preparation. AM-C: conceptualization, project administration, and writing. RD and MB: conceptualization, supervision, and investigation. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Deng SQ, Peng HJ. Characteristics of and public health responses to the coronavirus disease 2019 outbreak in China. J Clin Med. (2020) 9:575. doi: 10.3390/jcm9020575
2. Di Gennaro F, Pizzol D, Marotta C, Antunes M, Racalbuto V, Veronese N, et al. Coronavirus diseases (COVID-19) current status and future perspectives: a narrative review. Int J Environ Res Public Health. (2020) 17:2690. doi: 10.3390/ijerph17082690
3. Singhal TA. Review of coronavirus disease-2019 (COVID-19). Indian J Pediatr. (2020) 87:281–6. doi: 10.1007/s12098-020-03263-6
4. World Health Organization. Coronavirus Disease (COVID-19). (2020). Available online at: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports (accessed December 29, 2020).
5. Dymecka J. Psychospołeczne skutki pandemii COVID-19 [Psychosocial effects of the COVID-19 pandemic]. Neuropsychiatr Neuropsychol. (2021) 16:1–2, 1–10. doi: 10.5114/nan.2021.108030
6. Dymecka J, Gerymski R, Machnik-Czerwik A. Fear of COVID-19 as a buffer in the relationship between perceived stress and life satisfaction in the Polish population at the beginning of the global pandemic. Health Psychol Rep. (2021) 9:149–59. doi: 10.5114/hpr.2020.102136
7. Diener E, Emmons RA, Larsen RJ, Griffin S. The satisfaction with life scale. J Pers Assess. (1985) 49:71–5. doi: 10.1207/s15327752jpa4901_13
8. Mc Gee SL, Höltge J, Maercker A, Thoma MV. Sense of coherence and stress-related resilience: investigating the mediating and moderating mechanisms in the development of resilience following stress or adversity. Front Psychiatry. (2018) 21:378. doi: 10.3389/fpsyt.2018.00378
9. Gawrych M, Cichoń E, Kiejna A. COVID-19 pandemic fear, life satisfaction and mental health at the initial stage of the pandemic in the largest cities in Poland. Psychol Health Med. (2021) 26:107–13. doi: 10.1080/13548506.2020.1861314
10. Harper CA, Satchell LP, Fido D, Latzman RD. Functional fear predicts public health compliance in the COVID-19 pandemic. Int J Ment Health Addict. (2020) 27:1–14. doi: 10.1007/s11469-020-00281-5
11. Krok D, Zarzycka B, Telka E. Risk of contracting COVID-19, personal resources and subjective well-being among healthcare workers: the mediating role of stress and meaning-making. J Clin Med. (2021) 10:132. doi: 10.3390/jcm10010132
12. Satici B, Gocet-Tekin E, Deniz ME, Satici SA. Adaptation of the fear of COVID-19 scale: its association with psychological distress and life satisfaction in Turkey. Int J Ment Health Addict. (2020) 8:1–9. doi: 10.1007/s11469-020-00294-0
13. Su TP, Lien TC, Yang CY, Su YL, Wang JH, Tsai SL, et al. Prevalence of psychiatric morbidity and psychological adaptation of the nurses in a structured SARS caring unit during outbreak: a prospective and periodic assessment study in Taiwan. J Psychiatr Res. (2007) 41:119–30. doi: 10.1016/j.jpsychires.2005.12.006
14. Fardin MA. COVID-19 and anxiety: a review of psychological impacts of infectious disease outbreaks. Arch Clin Infect Dis. (2020) 15:e102779. doi: 10.5812/archcid.102779
15. Super S, Pijpker R, Polhuis K. The relationship between individual, social and national coping resources and mental health during the COVID-19 pandemic in the Netherlands. Health Psychol Rep. (2021) 9:186–92. doi: 10.5114/hpr.2020.99028
16. Garcia R. Neurobiology of fear and specific phobias. Learn Mem. (2017) 24:462–71. doi: 10.1101/lm.044115.116
17. Ahorsu DK, Lin CY, Imani V, Saffari M, Griffiths MD, Pakpour AH. The fear of COVID-19 scale: development and initial validation. Int J Ment Health Addict. (2020) 27:1–9. doi: 10.1007/s11469-020-00270-8
18. Bidzan-Bluma I, Bidzan M, Jurek P, Bidzan L, Knietzsch J, Stueck M, et al. A polish and German population study of quality of life, well-being, and life satisfaction in older adults during the COVID-19 pandemic. Front Psychiatry. (2020) 11:585813. doi: 10.3389/fpsyt.2020.585813
19. Özmen S, Özkan O, Özer Ö, Yanardag MZ. Investigation of COVID-19 fear, well-being and life satisfaction in Turkish Society. Soc Work Public Health. (2021) 36:164–77. doi: 10.1080/19371918.2021.1877589
20. Schou-Bredal I, Grimholt T, Bonsaksen T, Skogstad L, Heir T, Ekeberg Ø. Optimists' and pessimists' self-reported mental and global health during the COVID-19 pandemic in Norway. Health Psychol Rep. (2021) 9:160–8. doi: 10.5114/hpr.2021.102394
21. Kobasa SC. Stressful life events, personality, and health: an inquiry into hardiness. J Pers Soc Psychol. (1979) 37:1–11. doi: 10.1037/0022-3514.37.1.1
22. Kobasa SC, Maddi SR, Kahn S. Hardiness and health– a prospective study. J Pers Soc Psychol. (1982) 42:168–77. doi: 10.1037/0022-3514.42.1.168
23. Kobasa SC, Maddi SR, Puccetti M. Personality and exercise as buffers in the stress– illness relationship. J Behav Med. (1982) 4:391–404. doi: 10.1007/BF00845369
24. Antonovsky A. Unraveling The Mystery of Health - How People Manage Stress and Stay Well. New York, NY; New Jersey, NJ: Jossey-Bass Publishers (1987). p. 245–66.
25. Almedom AM. Resilience, hardiness, sense of coherence, and posttraumatic growth all paths leading to light at the end of the tunnel. J Loss Trauma. (2005) 10:253–65. doi: 10.1080/15325020590928216
26. Kravetz S, Drory Y, Florian V. Hardiness and sense of coherence and their relation to negative affect. Eur J Pers. (1993) 7:233–44. doi: 10.1002/per.2410070404
27. Skirka N. The relationship of hardiness, sense of coherence, sports participation, and gender to perceived stress and psychological symptoms among college students. J Sports Med Phys Fitness. (2000) 40:63–70.
28. Dymecka J, Bidzan-Bluma I, Bidzan M, Borucka-Kotwica A, Atroszko P, Bidzan M. Validity and reliability of the Polish adaptation of the Health-Related Hardiness Scale – the first confirmatory factor analysis results for a commonly used scale. Health Psychol Rep. (2020) 8:248–62. doi: 10.5114/hpr.2020.95746
29. Gana K. Is sense of coherence a mediator between adversity and psychological well-being in adults? Stress and Health. J Int Soc Investig Stress. (2001) 17:77–83. doi: 10.1002/smi.882
30. Hogh A, Mikkelson EG. Is sense of coherence a mediator or moderator of relationships between violence at work and stress reactions? Scand J Psychol. (2005) 46:429–37. doi: 10.1111/j.1467-9450.2005.00474.x
31. Dymecka J. Poczucie koherencji a style radzenia sobie ze stresem rodziców dzieci z choroba nowotworowa [Sense of coherence and coping styles in parents of children with cancer]. Psychoonkologia Psycho-oncology. (2018) 22:41–9. doi: 10.5114/pson.2018.82618
32. Eriksson M, Lindström B. Antonovsky's sense of coherence scale and the relation with health: a systematic review. J Epidemiol Commun Health. (2006) 60:376–81. doi: 10.1136/jech.2005.041616
33. Remes O, Wainwright NWJ, Surtees P, Lafortune L, Khaw KT, Brayne C. A strong sense of coherence associated with reduced risk of anxiety disorder among women in disadvantaged circumstances: British population study. BMJ Open. (2018) 8:e018501. doi: 10.1136/bmjopen-2017-018501
34. Eriksson M, Lindström B. Antonovsky's sense of coherence scale and its relation with quality of life: a systematic review. J Epidemiol Community Health. (2007) 61:938–44. doi: 10.1136/jech.2006.056028
35. Floyd A, Dedert E, Ghate S, Salmon P, Weissbecker I, Studts JL, et al. Depression may mediate the relationship between sense of coherence and quality of life in lung cancer patients. J Health Psychol. (2011) 16:249–57. doi: 10.1177/1359105310371856
36. Langius-Eklöf A, Lidman K, Wredling R. Health-related quality of life in relation to sense of coherence in a Swedish group of HIV-infected patients over a two-year follow-up. AIDS Patient Care STDS. (2009) 23:59–64. doi: 10.1089/apc.2008.0076
37. Robitschek C, Kashubeck S. A structural model of parental alcoholism, family functioning, and psychological health: the mediating effects of hardiness and personal growth orientation. J Counsel Psychol. (1999) 46:159–72. doi: 10.1037/0022-0167.46.2.159
38. Sunderlin CM. The relationship between risk, hardiness and social support on perceived quality of life among individuals diagnosed with fibromyalgia. Dissert Abst Int Sect B Sci Eng. (2007) 68:5900.
39. Wilder BF. The relationship of selected demographic characteristics, health conditions, and personality hardiness with quality of life in older adults. Dissert Abst Int Sect B Sci Eng. (1995) 56:5425.
40. Buheji M, Jahrami H. Analysing hardiness resilience in COVID-19 Pandemic-Using Factor Analysis. Int J Manag. (2020) 11:802–15.
41. Vagni M, Maiorano T, Giostra V, Pajardi D. Hardiness, stress and secondary trauma in Italian healthcare and emergency workers during the COVID-19 pandemic. Sustainability. (2020) 12:5592. doi: 10.3390/su12145592
42. Vagni M, Maiorano T, Giostra V, Pajardi D. Hardiness and coping strategies as mediators of stress and secondary trauma in emergency workers during the COVID-19 pandemic. Sustainability. (2020) 12:7561. doi: 10.3390/su12187561
43. Alsukah AI, Algadheeb NA, Almeqren MA, Alharbi FS, Alanazi RA, Alshehri AA, et al. Individuals' self-reactions toward COVID-19 pandemic in relation to the awareness of the disease, and psychological hardiness in Saudi Arabia. Front Psychol. (2020) 11:588293. doi: 10.3389/fpsyg.2020.588293
44. Braun-Lewensohn O, Sagy S, Roth G. Brief report: adolescence under missile attacks: sense of coherence as a mediator between exposure and stress-related reactions. J Adolesc. (2011) 34:195–97. doi: 10.1016/j.adolescence.2010.01.006
45. Tang ST, Cheng CC, Lee KC, Chen CH, Liu LN. Mediating effects of sense of coherence on family caregivers' depressive distress while caring for terminally ill cancer patients. Cancer Nurs. (2013) 36:25–33. doi: 10.1097/NCC.0b013e31826fc90d
46. Wiesmann U, Dezutter J, Hannich HJ. Sense of coherence and pain experience in older age. Int Psychogeriatr. (2014) 26:123–33. doi: 10.1017/S1041610213001695
47. Krok D. Sense of coherence mediates the relationship between the religious meaning system and coping styles in Polish older adults. Aging Ment Health. (2015) 19:1–8. doi: 10.1080/13607863.2015.1056772
48. Silarova B, Nagyova I, Rosenberger J, Studencan M, Ondusova D, Reijneveld SA, et al. Sense of coherence as an independent predictor of health-related quality of life among coronary heart disease patients. Qual Life Res. (2012) 21:1863–71. doi: 10.1007/s11136-011-0106-2
49. Rohani C, Abedi HA, Omranipour R, Langius-Eklöf A. Health-related quality of life and the predictive role of sense of coherence, spirituality and religious coping in a sample of Iranian women with breast cancer: a prospective study with comparative design. Health Qual Life Outcomes. (2015) 28:13–40. doi: 10.1186/s12955-015-0229-1
50. Wiebe DJ, McCallum DM. Health practices and hardiness as mediators in the stress-illness relationship. Health Psychol. (1986) 5:425–38. doi: 10.1037/0278-6133.5.5.425
51. Daniels JK, Hegadoren KM, Coupland NJ, Rowe BH, Densmore M, Neufeld RW, et al. Neural correlates and predictive power of trait resilience in an acutely traumatized sample: a pilot investigation. J Clin Psychiatry. (2012) 73:327–32. doi: 10.4088/JCP.10m06293
52. Antonovsky A. The structure and properties of the sense of coherence scale. Soc Sci Med. (1993) 36:725–33. doi: 10.1016/0277-9536(93)90033-Z
53. Koniarek J, Dudek B, Makowska Z. Kwestionariusz orientacji zyciowej. Adaptacja The Sense of Coherence Questionnaire (SOC) A. Antonovsky'ego. Przeglad Psychologiczny. (1993) 36:491–502.
54. Pollock SE. Human responses to chronic illness physiologic and psychosocial adaptation. Nurs Res. (1986) 35:90–5. doi: 10.1097/00006199-198603000-00008
56. Hayes AF. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach. New York, NY: Guilford Publications (2017).
57. Schoemann AM, Boulton AJ, Short SD. Determining power and sample size for simple and complex mediation models. Soc Psychol Pers Sci. (2017) 8:379–86. doi: 10.1177/1948550617715068
58. R Core Team R. A Language and Environment for Statistical Computing (version 3.6.3) [Computer Software]. (2020). Retrived from: https://www.r-project.org
59. Preacher KJ, Hayes AF. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav Res Methods. (2008) 40:879–91. doi: 10.3758/BRM.40.3.879
60. Polizzi C, Lynn SJ, Perry A. Stress and coping in the time of COVID-19: pathways to resilience and recovery. Clin Neuropsychiatry. (2020) 17:59–62. doi: 10.36131/CN20200204
61. Brooks SK, Webster RK, Smith LE, Woodland L, Wessely S, Greenberg N, et al. The psychological impact of quarantine and how to reduce it: rapid review of the evidence. Lancet. (2020) 14:912–20. doi: 10.1016/S0140-6736(20)30460-8
62. Dymecka J, Gerymski R. Niepełnosprawność a jakość zycia pacjentów ze stwardnieniem rozsianym. Mediacyjna rola zapotrzebowania na wsparcie społeczne [Disability and the quality of life of patients with multiple sclerosis. A mediating role of the need for social support]. Człowiek–Niepełnosprawność–Społeczeństwo/Man-Disabil Soc. (2019) 46:63–78. doi: 10.5604/01.3001.0013.7573
63. Harris SM. The effect of health value and ethnicity on the relationship between hardiness and health behaviors. J Pers. (2004) 72:379–411. doi: 10.1111/j.0022-3506.2004.00266.x
64. Maddi SR. Hardiness: an operationalization of existential courage. J Human Psychol. (2004) 44:279–98. doi: 10.1177/0022167804266101
65. Kobasa SC, Pucetti MC. Personality and social resources in stress resistance. J Pers Soc Psychol. (1983) 45:839–50. doi: 10.1037/0022-3514.45.4.839
66. Maddi SR, Harvey RH, Khoshaba DM, Lu JL, Persico M, Brow M. The personality construct of hardiness, iii: relationships with repression, innovativeness, authoritarianism, and performance. J Pers. (2006) 74:575–98. doi: 10.1111/j.1467-6494.2006.00385.x
67. Erim Y, Beckmann M, Kroencke S, Schulz KH, Tagay S, Valentin-Gamazo C, et al. Sense of coherence and social support predict living liver donors' emotional stress prior to living-donor liver transplantation. Clin Transplant. (2008) 22:273–80. doi: 10.1111/j.1399-0012.2007.00782.x
68. Posadzki P, Stockl A, Musonda P, Tsouroufli M. A mixed-method approach to sense of coherence, health behaviors, self-efficacy and optimism: towards the operationalization of positive health attitudes. Scand J Psychol. (2010) 51:246–52. doi: 10.1111/j.1467-9450.2009.00764.x
69. Ornell F, Schuch JB, Sordi AO, Kessler F. “Pandemic fear” and COVID-19: mental health burden and strategies. Braz J Psychiatry. (2020) 42:232–35. doi: 10.1590/1516-4446-2020-0008
70. Skokowski J, Szymczak J. Poczucie koherencji a lek u chorych na nowotwór płuca oczekujacych na operacje i u osób zdrowych [Sense of coherence and anxiety in patients with lung cancer awaiting surgery and in the healthy subjects]. Psychoonkologia/Psychooncology. (1999) 4:35–45.
71. Epishin VE, Salikhova AB, Bogacheva NV, Bogdanova MD, Kiseleva MG. Mental health and the COVID-19 pandemic: hardiness and meaningfulness reduce negative effects on psychological well-being. Psychology in Russia. State Art. (2020) 13:75–88. doi: 10.11621/pir.2020.0405
72. Odintsova MA, Radchikova NP, Stepanova LV. Assessment of the COVID-19 pandemic by Russian citizens with various levels of hardiness. Soc Psychol. (2020) 17:76–88. doi: 10.21702/rpj.2020.3.6
73. Allison P, Mnatsakanova A, McCanlies E, Fekedulegn D, Hartley TA, Andrew ME, et al. Police stress and depressive symptoms: role of coping and hardiness. Policing Int J. (2019) 43:247–61. doi: 10.1108/PIJPSM-04-2019-0055
74. Bartone PT, Homish GG. Influence of hardiness, avoidance coping, and combat exposure on depression in returning war veterans: a moderated-mediation study. J Affect Disord. (2020) 265:511–18. doi: 10.1016/j.jad.2020.01.127
75. van Servellen G, Topf M, Leake B. Personality hardiness, work-related stress, and health in hospital nurses. Hosp Topics. (1994) 72:34–9. doi: 10.1080/00185868.1994.9948484
76. Hashemi M, Darvizeh Z, Yazdi SM. Comparison of psychological hardiness and cognitive emotion regulation in students with social anxiety disorder and normal students. Psychol Stud. (2019) 15:41–56. doi: 10.22051/PSY.2019.20289.1641
77. Maddi SR, Brow M, Khoshaba DM, Vaitkus M. Relationship of hardiness and religiousness to depression and anger. Consult Psychol J. (2006) 58:148–61. doi: 10.1037/1065-9293.58.3.148
78. Maddi SR, Khoshaba DM. Hardiness and mental health. J Pers Assess. (1994) 63:265–74. doi: 10.1207/s15327752jpa6302_6
79. Gustavsson A, Bräänholm IB. Experienced health, life satisfaction, sense of coherence, and coping resources in individuals living with heart failure. Scand J Occup Ther. (2003) 10:138–43. doi: 10.1080/11038120310016120
80. Newton SE. Relationship of hardiness and sense of coherence to post-liver transplant return to work. Holist Nurs Pract. (1999) 13:71–9. doi: 10.1097/00004650-199904000-00011
81. Manning MR, Williams RF, Wolfe DM. Hardiness and the relationship between stressors and outcomes. Work Stress. (1988) 2:205–16. doi: 10.1080/02678378808259168
82. Dymecka J, Gerymski R, Machnik-Czerwik A. How does stress affect life satisfaction during the COVID-19 pandemic? Moderated mediation analysis of sense coherence and fear of coronavirus. Psychol Health Med. (2021) 31:1–9. doi: 10.1080/13548506.2021.1906436
83. Bruscia K, Shultis C, Dennery K, Dileo C. The sense of coherence in hospitalized cardiac and cancer patients. J Holist Nurs. (2008) 26:286–94. doi: 10.1177/0898010108317400
84. Moksnes UK, Løhre A, Espnes GA. The association between sense of coherence and life satisfaction in adolescents. Qual Life Res. (2013) 22:1331–38. doi: 10.1007/s11136-012-0249-9
85. Wiesmann U, Hannich HJ. The contribution of resistance resources and sense of coherence to life satisfaction in older age. J Happ Stud. (2013) 14:911–28. doi: 10.1007/s10902-012-9361-3
86. Gerasimčik-Pulko V, Pileckaite-Markoviene M, Bulotiene G, Ostapenko V. Relationship between sense of coherence and quality of life in early stage breast cancer patients. Acta Med Lituanica. (2009) 16:139–44. doi: 10.2478/v10140-009-0020-x
87. Dymecka J. Sense of coherence and health condition in parents of children with cancer. Psychoonkologia/Psychooncology. (2013) 17:16–22.
88. Norekvål TM, Fridlund B, Moons P, Nordrehaug JE, Sævareid HI, Wentzel-Larsen T, et al. Sense of coherence – a determinant of quality of life over time in older female acute myocardial infarction survivors. J Clin Nurs. (2010) 19:820–31. doi: 10.1111/j.1365-2702.2009.02858.x
Keywords: fear of COVID-19, life satisfaction, sense of coherence, hardiness, mediation
Citation: Dymecka J, Gerymski R, Machnik-Czerwik A, Derbis R and Bidzan M (2021) Fear of COVID-19 and Life Satisfaction: The Role of the Health-Related Hardiness and Sense of Coherence. Front. Psychiatry 12:712103. doi: 10.3389/fpsyt.2021.712103
Received: 19 May 2021; Accepted: 11 October 2021;
Published: 01 November 2021.
Edited by:
Nawar Shara, MedStar Health Research Institute (MHRI), United StatesReviewed by:
Qi Wang, The University of Hong Kong, Hong Kong SAR, ChinaGert Georg Wagner, Max Planck Institute for Human Development, Germany
Chung-Ying Lin, National Cheng Kung University, Taiwan
Evelyn Fernández-Castillo, Universidad Central Marta Abreu de Las Villas, Cuba
Yunier Broche-Pérez, Universidad Central Marta Abreu de Las Villas, Cuba
Copyright © 2021 Dymecka, Gerymski, Machnik-Czerwik, Derbis and Bidzan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rafał Gerymski, rafal.gerymski@uni.opole.pl