What is needed by parents of constipated infants and toddlers: A cross-sectional study in China
 Yuanyuan Wang
Yuanyuan Wang Jinjin Cao2
Jinjin Cao2  Hongyu Chen
Hongyu Chen- 1Department of Nursing, Children's Hospital of Nanjing Medical University, Nanjing, China
- 2Department of Gastroenterology, Children's Hospital of Nanjing Medical University, Nanjing, China
- 3Department of Emergency, Children's Hospital of Nanjing Medical University, Nanjing, China
- 4Department of Neurosurgery, The First Hospital of China Medical University, Shenyang, China
Background: Childhood functional constipation is a worldwide problem that affects the intestinal function of children and the quality of life of their families. Treatment and management of the disease need to be carried out at home by parents. Assessment of caregiving needs is an important link in planning and implementing the intervention. This study aimed to assess the caregiving needs of parents of FC infants and toddlers.
Methods: The researchers recruited convenience samples of parents from an outpatient pediatric constipation clinic of a children's medical center. Totally 211 fathers/mothers were recruited. Nursing needs were measured by a questionnaire, and associations between nursing needs and potential factors were examined using multiple regression analysis.
Results: The vast majority of participants (88.7%) expressed the need of receiving support from professionals, and only 44 (20.85%) had obtained help from medical staff. The needs of parents mainly include information needs, health needs, psychological needs, and social needs. Of all the needs, the highest score was for information needs (3.87 ± 0.69), followed by the dimension of health needs (3.74 ± 0.82). Results showed statistically significant differences in parental education, place of residence, age of children, duration of FC, defecation frequency, difficulty of defecation, and stool traits in nursing needs (p < 0.05). The regression model explained 64.2% of the variance of nursing needs.
Conclusions: Information needs were the major concern for parents, and the unmet needs of parents should be addressed during treatment and care. When developing care plans and providing health education, it should be adjusted according to the specific conditions of the child and parents to improve the compliance of the parents with treatment and care.
1. Introduction
Functional constipation (FC) is defined as constipation without an organic etiology and is diagnosed according to the Rome criteria (1). It is one of the most frequent reasons for visits to pediatric clinics of all ages, accounting for 95% of constipation in children (2, 3). In a recent review by Koppen (4), the pooled prevalence of childhood FC was 9.5%, with no gender differences.
Except for the high prevalence, FC poses a significant burden on health budgets, a report from England showed that FC cost the English National Health Service (NHS) £168 million in 2020–21 (5). Compared with other globally common, frustrating, and long-lasting disorders such as childhood asthma and migraine, children with constipation require seven times as much medical attention as asthma and three times as much as migraines (6, 7). According to research, functional constipation persists into adulthood and becomes a chronic condition in about one-third of affected children (8), thus having a continuous impact on health-related quality of life (9), and leading to a series of behavioral and emotional problems (10, 11). The etiology and pathophysiology of functional constipation are multi-factorial, and all causes are not mutually exclusive and may exist simultaneously. The initial symptoms are often painful defecation which leads to stool withholding. When more water was absorbed from the retained stool, the rectal sensation will be weakened and the child will lose the normal defecation impulse, which is further affecting gastrointestinal function (12, 13). Besides, Children with functional constipation often have a family history of constipation, and parental factors such as socioeconomic level, educational level, and parental rearing attitudes are closely related to childhood FC. In addition, toilet training issues, dietary causes, and stressful life events such as psychological or physical trauma are also important causes of FC (14).
To date, the recommended standard treatment for childhood FC includes diet therapy, constipation family education, toilet training, drug use, and behavior change (8). These treatments often need to be done at home by parents. The disease and the struggle to treat it at home can be challenging for parents (15, 16). The complexity of disease etiology and the burdensome and long-term treatment make parents feel overwhelmed, and various needs exist from diagnosis to the end of treatment. To provide an appropriate education for parents, it is necessary to determine what needs exist and the corresponding level of needs. Focusing on parents' care needs is an important first step in providing them with matched professional guidance, which is essential for successful disease management. Previous study have shown that gaps exist between the strategies offered by healthcare professionals and the caregiving needs of parents leading to poor communication and understanding gaps between them (17). If the health guidance cannot cover the caregiving needs, the incorrect behavior of parents harms the benign outcome of the disease. For example, previous studies have shown that failure to conduct defecation training in time or wrong defecation training are risk factors for FC (18). Therefore, it is necessary to understand caregiving needs to provide continuous and scientific care for children, maintain the physical and mental health of the main caregivers, reduce the psychological burden, and improve the clinical outcome of children (19). In general, childhood constipation tends to be rooted in infancy and early childhood. Therefore, it is very important to pay attention to the needs of parents of infants and toddlers and to provide help as early as possible. Previous studies have mostly used qualitative methods to explore parental needs (15, 20, 21), however, compared with qualitative research, quantitative research can not only investigate the content of parents' needs but also clarify the degree of various needs, so that our interventions can be more targeted.
In summary, our purpose was to investigate the caregiving needs of parents of FC infants and toddlers using a quantitative study. Besides, influencing factors were analyzed to better understand parental needs, promote effective communication between medical staff and parents, and ensure the effectiveness of health education implementation.
2. Methods
2.1. Design
A quantitative, cross-sectional, questionnaire-based design was used in this study to (a) investigate the caregiving needs of parents of infants and toddlers with FC and (b) the influencing factors of their needs. The study was conducted and reported according to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist (Supplementary File S1).
2.2. Participants and settings
Parents of infants and toddlers who visited the outpatient department of the Children's Medical Center of Jiangsu Province were recruited. Convenience sampling was performed, with the following criteria: inclusion criteria for children (a) Were of Chinese nationality; (b) Age ranged from 28 days to 3 years old; (c) Met the Rome IV criteria of FC; Inclusion criteria for parents: (a) Were able to speak Mandarin, understood the contents of the questionnaire, and clearly expressed personal opinions; (b) Undertook the main task of taking care of the children, and took care of the children for the longest time per day; (c) Aged between 18 and 55; (d) Were willing to participate and signed consent.
2.3. Measures
2.3.1. General information
Self-compiled, including two parts: (1) general data of children, including sex, age, defecation interval, defecation time and stool trait, constipation duration, and medical payment methods. Stool traits were classified according to the Bristol stool scale, type I = separate hard lumps, type II = lumpy and sausage-like, type III = a sausage shape with cracks in the surface, type IV = like a smooth, soft sausage or snake, type V = soft blobs with clear-cut edges, type VI = mushy consistency with ragged edges, type VII = liquid consistency with no solid pieces; (2) general data of parents, including age, education, place of residence, occupation, family average monthly income.
2.3.2. Development of the questionnaire
The development of the Caregiving needs questionnaire of parents of FC children mainly comprised two stages:
Stage 1: The construction of core components of the questionnaire
Firstly, we built the conceptual framework and dimensions of the scale based on the literature review. We searched the following databases of Web of Science, PubMed databases, China National Knowledge Infrastructure (CNKI), Wanfang Database, and VIP database with the keywords “caregiving needs” “nursing needs” “infant” “children” “parents” “caregiver” from the establishment of the database to May 2021. In addition, identified other publications by manually searching references in included publications. Finally, we divided the caregiving needs of parents into dimensions and items from four aspects through literature review and relevant scale (20–24): information needs, health needs, psychological needs, and social needs. Besides, we have set up a WeChat follow-up group of parents in June 2021 to collect the problems and needs of the parents in the process of caring for FC children. We collect information mainly through the following questions in the WeChat group: ① Can you talk about the needs and feelings of caring for a constipated child? ② What are the physical and psychological changes involved in caring for a constipated child? ③ What support or assistance you would like to receive in caring for a constipated child? The contents were analyzed and extracted according to the results, the initial items of the scale constructed in the previous stage were adjusted and supplemented, and a 35-item questionnaire was developed.
Stage 2: Questionnaire development.
Based on the 35-item questionnaire, an expert group meeting was conducted. Ten gastroenterologists and clinical nursing specialists were invited to the meeting (all with bachelor's degree or above with ten year working period). The person in charge of this project chaired the meeting and invited experts to read the content of the questionnaire. The experts put forward suggestions and modifications to the specific content, scientificity, and feasibility of the questionnaire. The researcher modifies the questionnaire according to the experts' opinions and reviewed it again with all experts to form the final version of the questionnaire. After the meeting, the researcher collects the experts' information questionnaire in time. After redundant components were eliminated, a 4-dimensional 19-item questionnaire was formed (Table 1). The questions included 5-point Likert-type questions (1 for not needed at all, 5 for very much needed) The higher the score, the higher the caregiving needs of the parents.

Table 1. Caregiving needs questionnaire of parents of FC children.
In August 2021, a preliminary survey was conducted to assess surface validity among the parents of 30 FC children who met the inclusion criteria. Parents were invited to make suggestions on the time required to fill in the questionnaire, legibility, and relevant content. The time to complete the questionnaire was 5–10 min. The content validity of the scale was evaluated by expert consultation. Six experts (2 clinical nursing experts, 2 nursing research experts, and 2 senior gastroenterologists, all with bachelor's degree or above with ten year working period) were selected to evaluate the questionnaire. The item level content validity (I-CVI) of the questionnaire was 0.83–1.00, and S-CVI/Ave was 0.98 > 0.90, indicating that the content validity was good. The Cronbach's α coefficients of the four parts were 0.747, 0.738, 0.744, and 0.793, and the Cronbach's α coefficient of the total questionnaire was 0.947, indicating good reliability.
2.4. Data analysis
According to Kendall's (25) experience and method of multivariate linear regression sample content estimation, the sample size should be 10–20 times the number of independent variables. There were 19 independent variables in this study, combined with the effective recovery rate of a presurvey questionnaire, and considering 10% sample loss, the sample size was finally determined to be 237 cases.
Entered the raw data into Microsoft Excel (2010 version) and SPSS 26.0, and double-checked the accuracy of the data. After screening for eligibility and completeness of responses as described earlier, the numerical variables’ normality distribution was established using descriptive statistics, graphic analysis, and the P–P test. Quantitative data were described with means, standard deviations, medians, and ranges; frequencies and percentages were used to describe categorical variables. Independent-sample t-tests or one-way analysis of variance were used to explore the differences between groups. All statistical analyses were performed with SPSS. Statistical significance was defined as a p < 0.05.
3. Results
3.1. Description of the samples
Two hundred and thirty-seven participants were invited to participate and 235 responded. After additional screening for the usability of data described earlier, responses from 211 participants were included in the final analysis, yielding a response rate of 89.03%. Their demographic characteristics were summarized in Table 2. Among 211 families, 150 (71.09%) had others to help take care of their children, helpers ranging from one to four. There were 142 families with only one child, while the other 69 had two or more children.
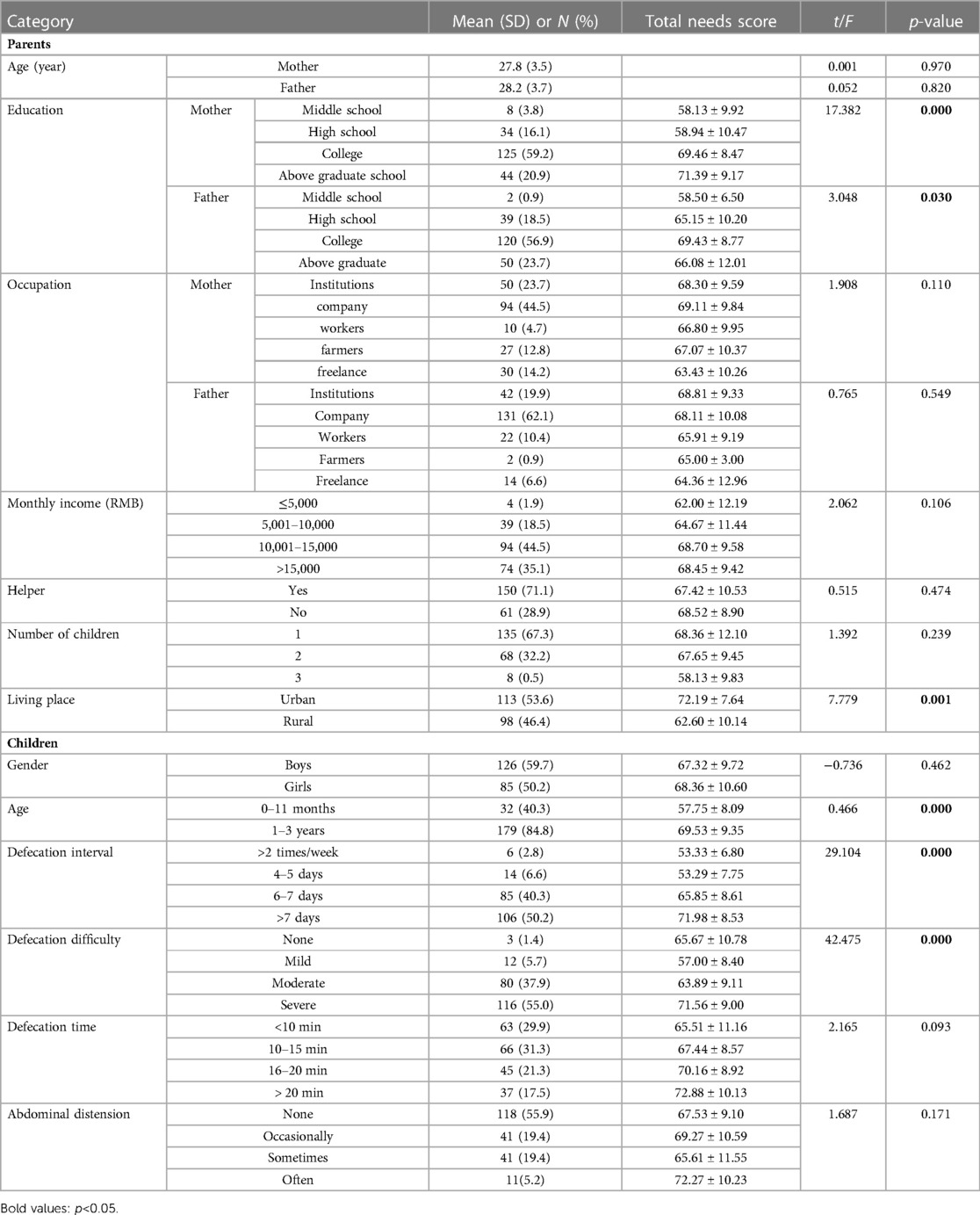
Table 2. Demographic information and single-factor analysis in nursing needs (N = 211).
3.2. Results of caregiving needs
For 211 groups of parents, the vast majority (n = 187, 88.7%) expressed need or great need of help from the professionals, and a small number (n = 24, 11.3%) indicated that they don't care or don't want help. Almost all parents said they had received help from family members previously, while 112 groups (53.08%) had received help from friends, colleagues, or neighbors, and only 44 (20.85%) said they had received help from medical staff. Analysis via the p–p indicated the total score and scores for each item were close to normally distributed, so we chose parameter test to analyze the data. The average total score for caregiving needs was 67.86 ± 9.96 (range, 19–95 points). Generally, parents had a moderate level of needs.
As shown in Table 3, the dimension with the highest score was information needs with 3.87 (SD: 0.69), followed by the dimension of health needs with 3.74 (SD: 0.82), and the lowest score is the dimension of psychological needs with 3.15 (SD: 0.87). The five items with the highest score were mainly distributed in the dimension of information needs and health needs. The information needs included constipation cause introduction, self-assessment method guidance, and diet and nutrition guidance, and health needs included defecation difficulty management and intestinal movement promotion guidance, with an average score from 4.01 to 4.43 (Table 4).

Table 3. Mean and standard deviations of variables of nursing needs (N = 211).
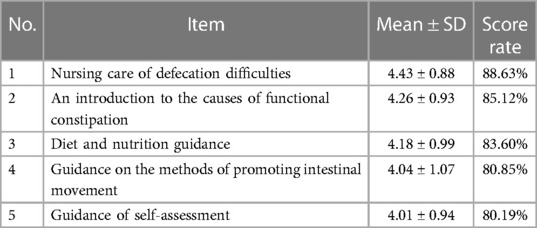
Table 4. The five items with the highest scores.
3.3. Factors associated with needs
The linear regression results among nursing needs and socio-demographic variables.
Demographic and disease-related data were used as independent variables, and questionnaire scores were used as dependent variables, independent sample T-test, and one-way ANOVA. The results showed that there were statistically significant differences in parental education, place of residence, age of children, duration, frequency, the difficulty of defecation, and fecal traits in nursing needs (p < 0.05). LSD multiple tests was used to further pally compare the multiple classification variables.
It was found that the mothers with college or undergraduate education, postgraduate education or above had higher scores than those with high school education or below (p < 0.05). Those fathers who had a college education or undergraduate education had higher scores than those who had high school or technical secondary education (p = 0.021), and higher than fathers with graduate education or above (p = 0.048). The scores of parental nursing needs of children with defecation intervals of 6–7 days were higher than those with 4–5 days per time (p = 0.000). At the same time, it was higher than those over 2 times/week (p = 0.004), and those beyond 7 days had the highest score of parental nursing needs, and the difference was statistically significant compared with other groups (p < 0.05). In terms of defecation difficulty, the score of severe defecation difficulty was the highest, and the difference was statistically significant (p < 0.05). Meanwhile, the score of moderate defecation difficulty was higher than that of mild (p < 0.05). AS for stool trait, parents of children with type I had the highest score, there was statistically significant compared with other groups (p < 0.001), and scores of type II were higher than those of type III, the difference was statistically significant (p < 0.001), but there was no statistically significant between type II and IV.
When analyzed by parental nursing needs score as the dependent variable, parental education level, place of residence, age of children, defecation interval, defecation difficulty, and stool traits were statistically significant (p < 0.05), by contrast, no significant differences were found in the age of parents, occupation, monthly income, helper, number of children, gender of children, defecation time, abdominal distension (p > 0.05). Taking total score as the dependent variable, area, parental education level, place of residence, age of children, defecation interval, defecation difficulty, and stool traits as an independent variable. Dummy variables were set for the above variables, with education status as middle school, defecation interval >2 times/week, stool trait as type IV or above, and no defecation difficulty as the reference variables (Table 5). The results showed that residence and stool traits were the main influencing factors for care needs (Table 6).
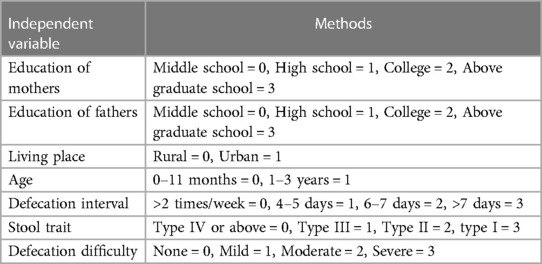
Table 5. Independent variable assignment methods.
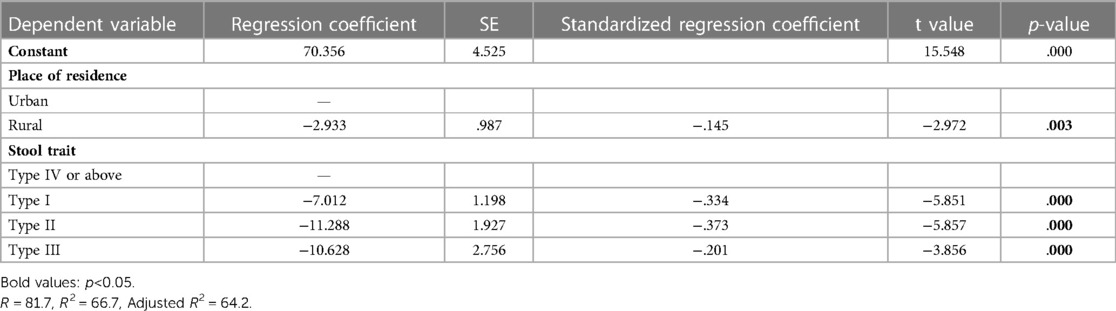
Table 6. Regression analysis of multiple factors in nursing needs (N = 211).
4. Discussion
4.1. Current status of caregiving needs
Totally 88.7% of the parents hoped or very much hoped to receive support, but only 20.85% said they had received help from medical personnel, indicating the existence of unmet care needs, and parents urgently needed the support from medical personnel. Research by Thompson (25) also showed that parents of children with FC had unmet needs for information, validation, and support, which is consistent with our study. In all dimensions, the score of information needs was the highest, mainly including disease-related knowledge and medication management. The reason may be that although clinicians can easily obtain reliable and high-quality evidence about childhood constipation, parents lack the same access, thus health care providers have become a reliable source of information. Besides, a study has pointed out that parents typically seek help from the healthcare system after living with their child's symptoms for months or years (26). Even after receiving an FC diagnosis, there is persistent parental ambiguity about the cause of the child's symptoms (27). Therefore, professional guidance is urgently needed after obtaining a diagnosis of the disease. In recent years, social media has become a source of health information for parents (28). However, confusion and misunderstanding among parents appeared with the application of professional vocabulary and the complexity of information (29, 30), in consequence, healthcare professionals were asked to verify the information on social media (31). Usually, Parents regard meeting their support and information needs as a turning point to rekindle hope and enhance confidence (23). Then, exploring multiple channels to meet the information needs of family members will never be outdated.
Our research demonstrated that psychological needs were lower than other needs, but previous studies (23, 32) noted that shame, embarrassment, and guilt were common obstacles faced by parents when providing medical care to children with FC. Probably due to the popularity of modern health perceptions, parents are more concerned about disease progression, symptom control, and complication prevention. In addition, the lack of awareness of the relationship between illness and negative emotions may be another reason for parents' neglect of psychological needs. Except for the parents themselves, a previous study (33) found that parents' experiences with FC children were often misunderstood by healthcare professionals. The study of Borowitz (34) also showed the same results. The low psychological needs of parents and the underestimation of the psychological needs of medical staff are both reminding us that this is a phenomenon worth thinking about. On the one hand, the positive emotions of parents are very important for the management of constipation in children (35). On the other hand, double neglect of psychological problems is bad for communication between parents and healthcare providers. This reminds us that it is worthwhile to devote attention to their psychological state and emotional changes, whether parents are aware of it or not. We, therefore, recommend the use of tools to monitor parents' psychological state, if necessary, to provide professional psychological guidance to those who need it.
4.2. Factors associated with caregiving needs
Our study demonstrated that the place of residence was an important influencing factor of parental care needs, that was, the score of living in rural areas was lower than that of children living in urban areas (p = 0.003), which is similar to the results of other studies (19). In our study, 46.4% of the respondents lived in rural areas. A previous study has shown that the health literacy level of urban residents was higher than that of rural residents (36). Most of the parents from rural areas lack basic awareness of the disease or had difficulty understanding the outcome of the disease. In other words, rural residents have insufficient knowledge of the disease and lack the initiative to acquire disease-related content.
In addition, quality medical resources are more accessible in cities, but not in rural areas making it impossible to form a reasonable medical orientation, resulting in a lag in the development of medical security and accessibility in rural areas (37). There are still some problems in the equalization of basic medical and health services in urban and rural areas in China, such as insufficient aggregate and unbalanced supply structure. Therefore, the public health resources obtained by rural residents are relatively limited compared to urban residents (38). Accordingly, parents' confidence in local medical care may be affected by those reasons. Simultaneously, rural residents often need to seek medical treatment in different places, so they were less dependent on the medical treatment place, which affects their caregiving needs. Hence, when we carry out nursing health education and nursing intervention, we should take the patient's residence as an important factor to formulate a scientific and standardized individual family nursing model, thereby improving treatment compliance, and improving the clinical symptoms of children.
In addition to the place of residence, children's stool traits were also the factors affecting the parents' nursing needs (p < 0.001), that is, the stool traits were assessed according to the Bristol stool scale, and the harder the stool trait, the higher the parental needs score. This is consistent with the findings of the same type of research (39, 40). A previous study showed that large and hard stool was the most frequent symptom among children with functional constipation, hard stool consistency was found in about 93.7% of cases (41). In the diagnosis of FC and identification of early warning symptoms (42), parental perception of constipation depends primarily on stool traits and frequency of defecation, which is also the most common reason for seeking medical attention. This suggested that parents were more likely to ignore other symptoms, leading to delays in seeking medical treatment. This was also proved by a study in Sri Lanka which showed that only 24% of young children with FC were seen by a medical doctor (43). On the other hand, ignorance of signs and symptoms indicated insufficient awareness of the disease and could affect treatment adherence (33). To achieve consensus on child care, new policies should be mindful of the long period required to guarantee interaction and counseling between parents and healthcare professionals. In addition, parents should be assisted to identify the symptoms and signs associated with the disease and improve their understanding of the disease during consultations and care planning.
In summary, our findings highlighted the caregiving needs of parents caring for a child with FC. The strength of this study lies in the large sample of parents of children with constipation and the large response rate we achieved due to patient pre-survey explanatory instructions and the preparation of small gifts. In addition, our study quantified the different needs of parents in various domains, giving us an intuitive understanding of the needs of parents of FC children. In future clinical practice, clinicians should consider the needs of parents of children, especially the information needs, when communicating with their families about constipation, and conduct personalized communication according to the specific situation of children and parents. According to the information provided by the questionnaire, it is very helpful to organize health education lectures regularly to meet the nursing needs of parents. Create a communication platform to provide opportunities for parents to share information and exchange experiences. The construction of an information-oriented hospital also provides a new communication method for parents who live in rural areas. Medical staff should pay attention to publicizing and using the information facilities of the hospital.
4.3. Limitations
Several limitations of this study should be taken into consideration. Firstly, A cross-sectional design does not explain causality. Secondly, the results are not necessarily representative because of convenience sampling. Thirdly, the study sample was drawn from only one hospital, which may limit the generalization of the findings. A multicenter study with a wider geographic range of selection is recommended. Future studies should employ longitudinal research methods to observe dynamic changes in caregiving needs.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by Institutional Research Ethics Committee of Children's Hospital of Nanjing Medical University. Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
Author contributions
YW and JC conceived and designed this study. YW and JW were responsible for data acquisition and analysis of the data. HC revised the grammar of the article. WZ was responsible for revising the article and supplementing the article's framework and content. ZL supported the study and provided comments on statistical methods. YW drafted the preliminary version of the manuscript. JC and ML critically revised the work for important intellectual content. ML and ZL obtained funding sources. All authors approved the final manuscript and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. ML obtained the research funds through which this research was conducted. All authors contributed to the article and approved the submitted version.
Funding
This study was supported by the Scientific Research Project of the Jiangsu Province Association of Maternal and Child Health (FYX202120).
Acknowledgments
The authors would like to acknowledge Jianling Bai for providing valuable advice for data statistics, and we thank the director of the nursing department for recruiting.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2023.1066355/full#supplementary-material.
References
1. Benninga MA, Faure C, Hyman PE, St James Roberts I, Schechter NL, Nurko S. Childhood functional gastrointestinal disorders: neonate/toddler. Gastroenterology. (2016) 150(6):1443–5. doi: 10.1053/j.gastro.2016.02.016
2. Vriesman MH, Koppen IJN, Camilleri M, Di Lorenzo C, Benninga MA. Management of functional constipation in children and adults. Nat Rev Gastroenterol Hepatol. (2020) 17(1):21–39. doi: 10.1038/s41575-019-0222-y
3. Rouster A, Karpinski A, Silver D, Monagas J, Hyman P. Functional gastrointestinal disorders dominate pediatric gastroenterology outpatient practice. J Pediatr Gastroenterol Nutr. (2016) 62(6):847–51. doi: 10.1097/mpg.0000000000001023
4. Koppen IJN, Vriesman MH, Saps M, Rajindrajith S, Shi X, van Etten-Jamaludin FS, et al. Prevalence of functional defecation disorders in children: a systematic review and meta-analysis. J Pediatr. (2018) 198:121–30. doi: 10.1016/j.jpeds.2018.02.029
5. The Lancet Gastroenterology Hepatology. The cost of constipation. Lancet Gastroenterol Hepatol. (2019) 4(11):811. eng. doi: 10.1016/s2468-1253(19)30297-3
6. Han D, Iragorri N, Clement F, Lorenzetti D, Spackman E. Cost effectiveness of treatments for chronic constipation: a systematic review. PharmacoEconomics. (2018) 36(4):435–49. doi: 10.1007/s40273-018-0609-6
7. Liem O, Harman J, Benninga M, Kelleher K, Mousa H, Di Lorenzo C. Health utilization and cost impact of childhood constipation in the United States. J Pediatr. (2009) 154(2):258–62. doi: 10.1016/j.jpeds.2008.07.060
8. Southwell BR. Treatment of childhood constipation: a synthesis of systematic reviews and meta-analyses. Expert Rev Gastroenterol Hepatol. (2020) 14(3):163–74. doi: 10.1080/17474124.2020.1733974
9. Vriesman MH, Rajindrajith S, Koppen IJN, van Etten-Jamaludin FS, van Dijk M, Devanarayana NM, et al. Quality of life in children with functional constipation: a systematic review and meta-analysis. J Pediatr. (2019) 214:141–50. doi: 10.1016/j.jpeds.2019.06.059
10. Rajindrajith S, Ranathunga N, Jayawickrama N, van Dijk M, Benninga MA, Devanarayana NM. Behavioral and emotional problems in adolescents with constipation and their association with quality of life. PLoS One. (2020) 15(10):e0239092. doi: 10.1371/journal.pone.0239092
11. Wang C, Shang L, Zhang Y, Tian J, Wang B, Yang X, et al. Impact of functional constipation on health-related quality of life in preschool children and their families in Xi’an, China. PLoS One. (2013) 8(10):e77273. doi: 10.1371/journal.pone.0077273
12. Zeevenhooven J, Koppen IJN, Benninga MA. The new Rome IV criteria for functional gastrointestinal disorders in infants and toddlers. Pediatr Gastroenterol Hepatol Nutr. (2017) 20(1):1. doi: 10.5223/pghn.2017.20.1.1
13. Waterham M, Kaufman J, Gibb S. Childhood constipation. Aust Fam Physician. (2017) 46(12):908–12. Available from: https://www.racgp.org.au/afp/2017/december/childhood-constipation/29464227
14. Leung AK, Hon KL. Pediatrics: how to manage functional constipation. Drugs Context. (2021) 10:020-11-2. doi: 10.7573/dic.2020-11-2
15. Flankegård G, Mörelius E, Duchen K, Rytterström P. Experiences of parents who give pharmacological treatment to children with functional constipation at home. J Adv Nurs. (2020) 76(12):3519–27. doi: 10.1111/jan.14539
16. Kaugars AS, Silverman A, Kinservik M, Heinze S, Reinemann L, Sander M, et al. Families’ perspectives on the effect of constipation and fecal incontinence on quality of life. J Pediatr Gastroenterol Nutr. (2010) 51(6):747–52. doi: 10.1097/MPG.0b013e3181de0651
17. Hoover CG, Coller RJ, Houtrow A, Harris D, Agrawal R, Turchi R. Understanding caregiving and caregivers: supporting children and youth with special health care needs at home. Acad Pediatr. (2022) 22(2S):S14–21. doi: 10.1016/j.acap.2021.10.007
18. Ho JMD, How CH. Chronic constipation in infants and children. Singapore Med J. (2020) 61(2):63–8. doi: 10.11622/smedj.2020014
19. Tu H, Long X, Millie D, Shen Q. Status quo of nursing needs during home rehabilitation in main caregivers of children with congenital heart disease after surgery and its influence factors: a 148-case study(in Chinese). J Nurs. (2021) 28(1):45–50. Available from: https://kns.cnki.net/kns8/defaultresult/index
20. Thompson AP, MacDonald SE, Wine E, Scott SD. Understanding Parents’ experiences when caring for a child with functional constipation: interpretive description study. JMIR Pediatr Parent. (2021) 4(1):e24851. doi: 10.2196/24851
21. Thompson AP, Wine E, MacDonald SE, Campbell A, Scott SD. Parents’ experiences and information needs while caring for a child with functional constipation: a systematic review. Clin Pediatr (Phila). (2021) 60(3):154–69. doi: 10.1177/0009922820964457
22. Yang M. The analysis of needs and influential factors of care nursing service in hospitalized children's families based on the KANO model (in Chinese). Yanbian Korean Autonomous Prefecture, Jilin; Yanbian University (2018).
23. Li Y. Home care service demand of elderly with chronic diseases based on “internet +” and nursing service plan formulation (in Chinese). Nanchang, Jiangxi: Nan Chang University (2021).
24. Li S, Zhang P, Luo Y LIUY, Hu L. Demands of transitional care for children with chronic disease and their families (in Chinese). Nurs J Chin People's Lib Army. (2018) 35(24):46–50. Available from: https://kns.cnki.net/kns8/defaultresult/index
25. Ni P, Chen J, Liu N. Sample size estimation of quantitative research in nursing research (in Chinese). Chin J Nurs. (2010) 45(4):378–9. Available from: https://kns.cnki.net/kns8/defaultresult/index
26. Klages KL, Berlin KS, Silverman AH, Mugie S, Di Lorenzo C, Nurko S, et al. Empirically derived patterns of pain, stooling, and incontinence and their relations to health-related quality of life among youth with chronic constipation. J Pediatr Psychol. (2017) 42(3):325–34. doi: 10.1093/jpepsy/jsw068
27. van Tilburg MAL, Squires M, Blois-Martin N, Williams C, Benninga MA, Peeters B, et al. Parental knowledge of fecal incontinence in children. J Pediatr Gastroenterol Nutr. (2012) 55(3):283–7. doi: 10.1097/MPG.0b013e31824cf555
28. Frey E, Bonfiglioli C, Brunner M, Frawley J. Parents’ use of social Media as a health information source for their children: a scoping review. Acad Pediatr. (2022) 22(4):526–39. doi: 10.1016/j.acap.2021.12.006
29. Price SL, Aston M, Monaghan J, Sim M, Tomblin Murphy G, Etowa J, et al. Maternal knowing and social networks: understanding first-time Mothers’ search for information and support through online and offline social networks. Qual Health Res. (2018) 28(10):1552–63. doi: 10.1177/1049732317748314
30. Thorpe M, Taylor J, Cole R. Parents’ use of information accessed through social media to make immunisation decisions for their young children. Health Promot J Austr. (2021) 32(2):189–96. doi: 10.1002/hpja.336
31. Nicholl H, Tracey C, Begley T, King C, Lynch AM. Internet use by parents of children with rare conditions: findings from a study on Parents’ web information needs. J Med Internet Res. (2017) 19(2):e51. doi: 10.2196/jmir.5834
32. Yıldırım A, Biçer Ş, Hacıhasanoğlu-Aşılar R, Özdamar MY, Şahin H, Gül V. The effect of education given to children with functional constipation and fecal incontinence and their mothers on anxiety and constipation management. Florence Nightingale J Nurs. (2020) 28(3):321–32. doi: 10.5152/FNJN.2020.19134
33. Farrell M, Holmes G, Coldicutt P, Peak M. Management of childhood constipation: parents’ experiences. J Adv Nurs. (2003) 44(5):479–89. doi: 10.1046/j.0309-2402.2003.02831.x
34. Borowitz SM, Cox DJ, Kovatchev B, Ritterband LM, Sheen J, Sutphen J. Treatment of childhood constipation by primary care physicians: efficacy and predictors of outcome. Pediatrics. (2005) 115(4):873–7. doi: 10.1542/peds.2004-0537
35. Koppen IJN, van Wassenaer EA, Barendsen RW, Brand PL, Benninga MA. Adherence to polyethylene glycol treatment in children with functional constipation is associated with parental illness perceptions, satisfaction with treatment, and perceived treatment convenience. J Pediatr. (2018):199:132-139.e1. doi: 10.1016/j.jpeds.2018.03.066
36. Tang W, Wang W. Analysis on the status of health literacy among residents in ningxia province (in Chinese). Chin J Health Educ. (2021) 37(7):593–6+601. Available from: https://kns.cnki.net/kns8/defaultresult/index
37. Huang CF, Tang XB, Yang YS. Analysis of the impact of urban and rural residents per capita disposable income on health care expenditure and regional difference (in Chinese). Soft Sci Health. (2017) 31(12):23–7. Available from: https://kns.cnki.net/kns8/defaultresult/index
38. Liu YO. Realization of equalization of basic medical and health services from the perspective of urban-rural integrated development (in Chinese). China Econ Trade Herald. (2021) M(08):86–7. Available from: https://kns.cnki.net/kns8/defaultresult/index
39. Park M, Suh EE, Yu S-Y. Uncertainty and nursing needs of parents with pediatric cancer patients in different treatment phases: a cross-sectional study. Int J Environ Res Public Health. (2021) 18(8):4253. doi: 10.3390/ijerph18084253
40. Aziza YDA, Wang S-T, Huang M-C. Unmet supportive care needs and psychological distress among parents of children with cancer in Indonesia. Psychooncology. (2019) 28(1):92–8. doi: 10.1002/pon.4914
41. Dehghani SM, Kulouee N, Honar N, Imanieh M-H, Haghighat M, Javaherizadeh H. Clinical manifestations among children with chronic functional constipation. Middle East J Dig Dis. (2015) 7(1):31–5. doi: 10.15171/mejdd.2017.87
42. Bolia R, Safe M, Southwell BR, King SK, Oliver MR. Pediatric constipation for general paediatricians: review using a case-based and evidence-based approach. J Paediatr Child Health. (2020) 56(11):1708–18. doi: 10.1111/jpc.14720
Keywords: functional constipation, infant, need assessment, caregiving, parents
Citation: Wang Y, Cao J, Zhang W, Chen H, Li M, Liu Z and Wang J (2023) What is needed by parents of constipated infants and toddlers: A cross-sectional study in China. Front. Pediatr. 11:1066355. doi: 10.3389/fped.2023.1066355
Received: 11 October 2022; Accepted: 27 March 2023;
Published: 12 April 2023.
Edited by:
Licia Pensabene, Magna Græcia University, ItalyReviewed by:
Monika Trzpis, University of Groningen, NetherlandsValentina Giorgio, Agostino Gemelli University Polyclinic (IRCCS), Italy
Nilton Machado, Hospital das Clínicas, Faculdade de Medicina de Botucatu, Brazil
© 2023 Wang, Cao, Zhang, Chen, Li, Liu and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mei Li limeilimei8686@163.com Zhifeng Liu zfliu@njmu.edu.cn
†These authors have contributed equally to this work and share first authorship
Specialty Section: This article was submitted to Pediatric Gastroenterology, Hepatology and Nutrition, a section of the journal Frontiers in Pediatrics