 Wesam Kooti1
Wesam Kooti1 Hadi Esmaeili Gouvarchin Ghaleh1*Mahdieh Farzanehpour1Ruhollah Dorostkar1Bahman Jalali Kondori2,3Masoumeh Bolandian1
Hadi Esmaeili Gouvarchin Ghaleh1*Mahdieh Farzanehpour1Ruhollah Dorostkar1Bahman Jalali Kondori2,3Masoumeh Bolandian1- 1Applied Virology Research Center, Baqiyatallah University of Medical Sciences, Tehran, Iran
- 2Department of Anatomical Sciences, Faculty of Medicine, Baqiyatallah University of Medical Sciences, Tehran, Iran
- 3Baqiyatallah Research Center for Gastroenterology and Liver Diseases (BRCGL), Baqiyatallah University of Medical Sciences, Tehran, Iran
The global rate of cancer has increased in recent years, and cancer is still a threat to human health. Recent developments in cancer treatment have yielded the understanding that viruses have a high potential in cancer treatment. Using oncolytic viruses (OVs) is a promising approach in the treatment of malignant tumors. OVs can achieve their targeted treatment effects through selective cell death and induction of specific antitumor immunity. Targeting tumors and the mechanism for killing cancer cells are among the critical roles of OVs. Therefore, evaluating OVs and understanding their precise mechanisms of action can be beneficial in cancer therapy. This review study aimed to evaluate OVs and the mechanisms of their effects on cancer cells.
Background
Millions of individuals are affected by cancer annually. Cancer is considered the leading cause of death and the most important barrier to the increase in life expectancy in the twenty-first century. In 2018, 18.1 million new cancer cases (17.0 million cancer cases excluding non-melanoma skin cancers) were reported. The mortality due to cancer in 2018 was 9.6 million (9.5 million, excluding non-melanoma skin cancers) (1). Significant developments in cancer treatment started in 1900. The achievements of this progress include the development of diagnostic, surgery, chemotherapy, hormone therapy, gene therapy, and cell therapy methods. Regardless of these advancements, human is still incapable of combating cancer, as none of the identified treatment methods could be used in all stages of cancer (2). Many of cancer patients experience a relapse of disease progression regardless of the primary response to treatment.
Furthermore, complete resection of the tumor is difficult or impossible in many cases (3). Immunotherapy has evolved as a practical treatment choice against malignant diseases during the past decades. Studies in oncolytic virotherapy (OVT) developed in the early twentieth century as an observational science for the cases of spontaneous regression of tumors were reported due to infection with specific viruses (4).
Oncolytic viruses (OVs) include a group of viruses that selectively affect and kill malignant cells, leaving the surrounding healthy cells unaffected. OVs have direct cytotoxic effects on cancer cells and augment host immune reactions and result in the destruction of the remaining tumoral tissue and establish a sustained immunity (5). Indeed, OVs function in four ways against tumor cells, including oncolysis, antitumor immunity, transgene expression, and vascular collapse (6). Regarding the fact that cancer cells are developed to avoid detection and destruction by the host immune system and also to resist apoptosis, which are the critical responses of normal cells in limiting viral infections, OVs can kill cancer cells through a spectrum of actions ranging from direct cytotoxicity to induction of immune-mediated cytotoxicity. OVs can also indirectly destroy cancer cells by destroying tumor vasculature and mediating antitumor responses (7). Furthermore, in order to augment the therapeutic characteristics, modifications in OVs by genetic engineering such as insertions and deletions in the genome have been employed in many investigations; thus, additional antitumor molecules can be delivered to cancer cells and effectively bypass the widespread resistance of single-target anticancer drugs (8)
It should be noted that the use of OVs in cancer therapy was limited due to the pathogenicity and toxicity of these viruses in human cases. Recent advancements in genetic engineering have optimized the function of OVs through genetic modifications and therefore have become the issue of interest in OVT (9). Each virus tends to a specific tissue, and this tendency determines which host cells are affected by the virus and what type of disease will be generated. For instance, rabies, hepatitis B, human immunodeficiency virus (HIV), and influenza viruses affect neurons, hepatocytes, T lymphocytes, and respiratory tract epithelium, respectively. Several naturally occurring viruses have a preferential but not exclusive tendency towards cancer cells. This issue is more attributed to tumor cell biology compared to the biology of the virus.
OVs are generally categorized into two groups. One group is preferentially replicated in cancer cells and is not pathogenic for normal cells due to the increased sensitivity to the innate immune system’s antiviral signaling or dependence on the oncogenic signaling pathways. Autonomous parvovirus, myxoma virus (MYXV; poxvirus), Newcastle disease virus (NDV; paramyxovirus), reovirus, and Seneca valley virus (SVV; picornavirus) are categorized in this group. The second group of OVs includes viruses that are either genetically modified for purposes including vaccine vectors such as mumps virus (MV; paramyxovirus), poliovirus (PV; picornavirus), and vaccinia virus (VV; poxvirus), or genetically engineered through mutation/deletion of genes required for replication in normal cells, including adenovirus (Ad), Herpes simplex virus (HSV), VV, and vesicular stomatitis virus (VSV; rhabdovirus) (10).
Furthermore, the mutation in cancer cells, drug adaptation, resistance, and cell immortality were effective in the initiation and speed of viral dissemination. Today, researchers are trying to discover and identify a new generation of OVs to save more patients’ lives from cancer. Evaluation of OVs and identification of the exact mechanism of action of these viruses can be helpful in this way (11). This review study aimed to evaluate OVs and their mechanism of action against cancer cells.
Methodology
The key terms in the literature search included oncolytic virus, cancer, immunotherapy, innate immunity, adaptive immunity, virotherapy, viral therapy, oncolytic, and virus were searched in international databases, namely, Web of Science, PubMed, and Scopus from 2004 to 2021. The inclusion criterion was the evaluation of viruses using standard in vivo and in vitro laboratory methods. Exclusion criteria were lack of access to full text articles and incomplete description or assessment of diseases other than cancers.
Results
The primary search yielded 1,450 articles. Finally, 47 articles were included in the review after eliminating irrelevant and duplicate studies. The characteristics of the 47 included articles are presented in Table 1, performed from 2004 to 2021. The OV families assessed in the studies included Ad, MV, PV, NDV, SFV, HSV, VV Reovirus, and bovine herpesvirus (BHV). The most commonly assessed virus was adenovirus (Ad) (n = 15), followed by the herpesvirus (HSV) (n = 12) and measles virus (MV) (n = 7). The least assessed viruses were BHV, SFV, and Reovirus (n = 1).
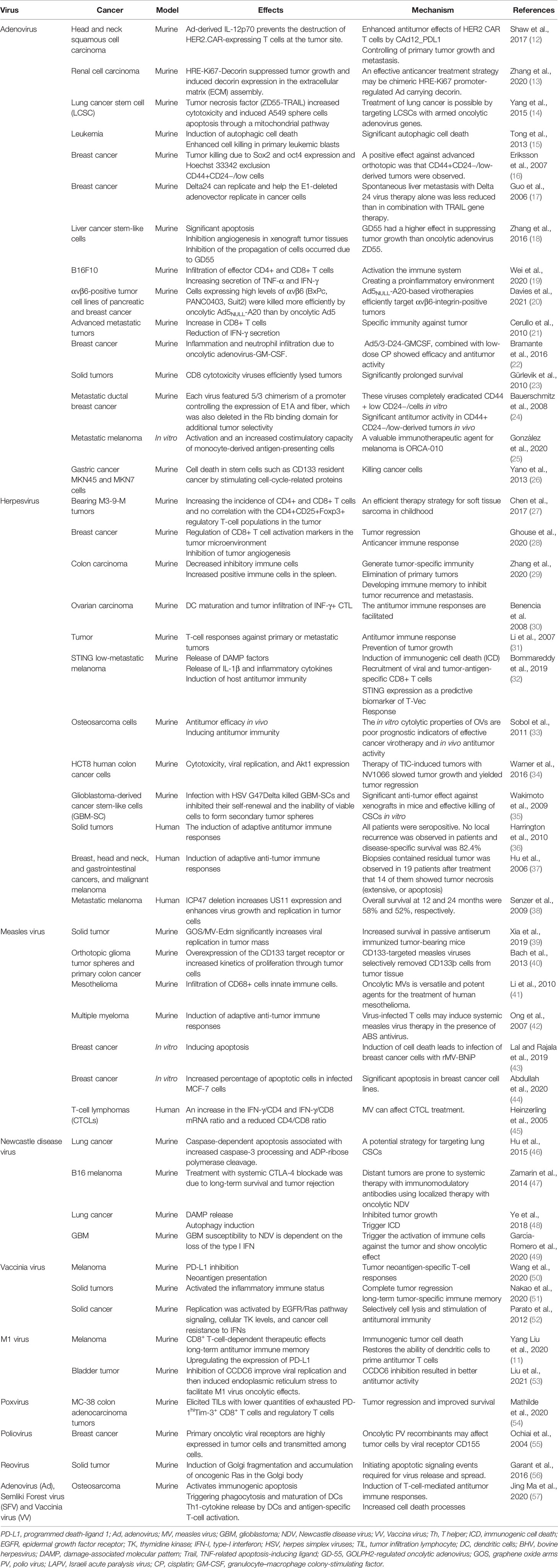
Table 1 The collective studies on OVs.
According to Table 1, OVs may employ multifunction against tumor cells; however, the most antitumor actions of OVs were related to cytolysis activity and inducing antitumor immunity (n = 26) in which adenovirus (n = 11) and HSV (n = 9) were the most responsible OVs in their categories, respectively. However, the last action was associated with vascular collapse. The collective data in Table 2 exhibited a summary of clinical trials of OVs implicated in malignancies highlighting the most considerable focus on engineered VV by TKdel GMCSF exp (JX-594) on solid tumors supported by Jennerex Biotherapeutics Company. The majority of studies under clinical trials involve a transgene virus encoding an immune-stimulatory or proapoptic gene to boost the oncolytic features of the virus. As Table 2 reveals, granulocyte–macrophage colony-stimulating factor (GM-CSF) and pro-drug-converting enzymes are the most popular transgenes, although many OVs encoding novel therapeutic cargos are in clinical development. Streby et al., in phase I clinical trial, examined the effects of HSV1716 on relapsed/refractory solid tumors. Despite the fact that none of the patients exhibited objective responses, virus replication and inflammatory reactions were seen in patients (58). In another clinical trial, Desjardins et al. reported a higher survival rate in grade IV malignant glioma patients who received recombinant nonpathogenic polio–rhinovirus chimera (59). In a phase I clinical trial, Rocio Garcia-Carbonero et al. discovered that enadenotucirev IV infusion was associated with high local CD8+ cell infiltration in 80% of tumor samples evaluated, indicating a possible enadenotucirev-driven immune response (60). TG4023, a modified vaccinia Ankara viral vector carrying the FCU1 suicide gene, was used in a phase I trial to convert the non-cytotoxic prodrug flucytosine (5-FC) into 5-fluorouracil (5-FU) in the intratumor. Finally, 16 patients with liver tumors were successfully injected; the MTD was not achieved, and a high therapeutic index was demonstrated (61). Dispenzieri et al. examined MV-NIS effects in patients with relapsed, refractory myeloma and reported satisfactory primary results (62).
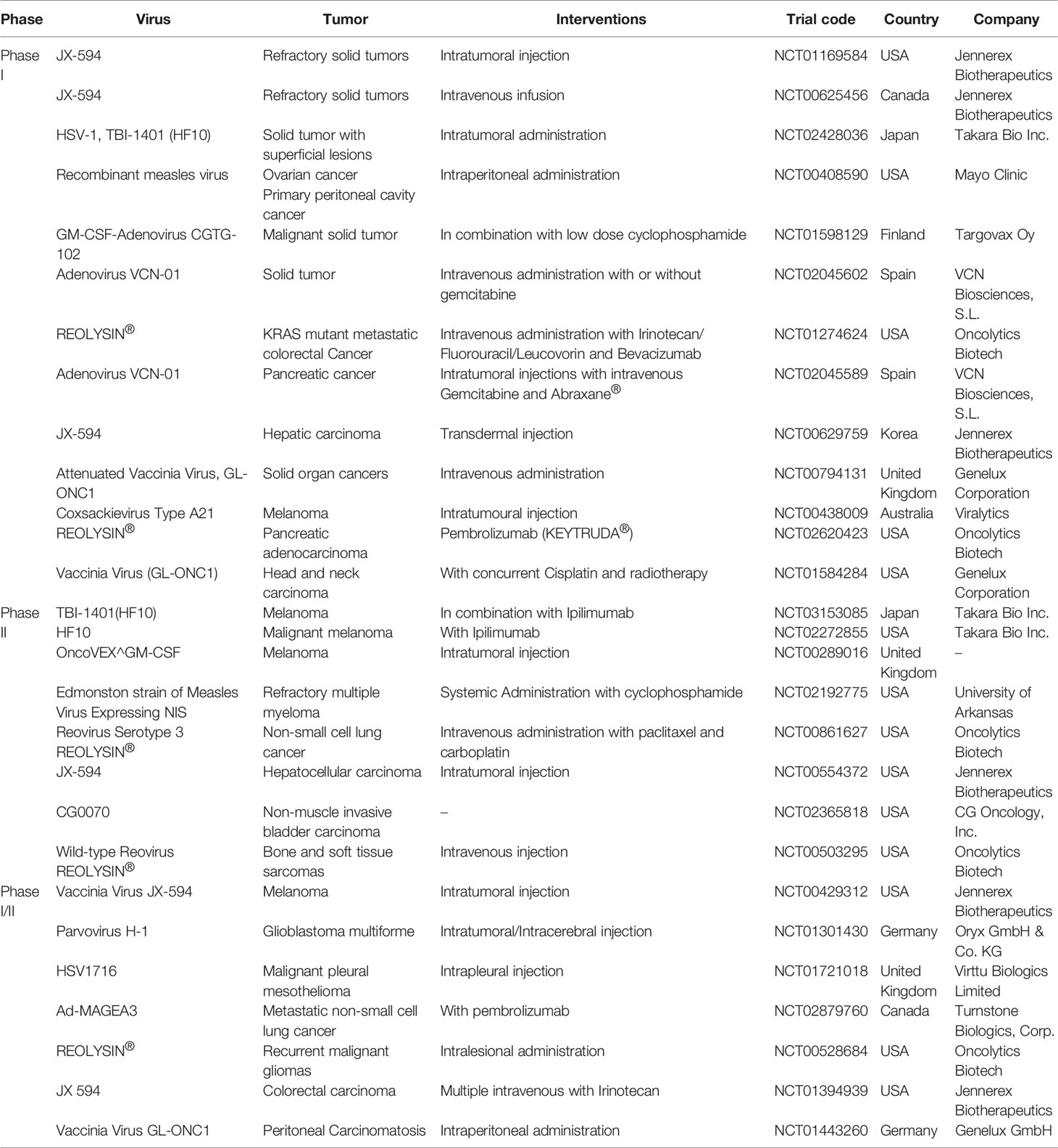
Table 2 The summary of clinical trials for oncolytic viruses.
Cohn et al., in phase II clinical trial, evaluated the effects of oncolytic reovirus (Reolysin®) plus weekly paclitaxel in women with recurrent or persistent ovarian, tubal, or primary peritoneal cancer. The results did not show any improvement in the patient status (63), although Mahalingam et al. showed that REOLYSIN®, plus carboplatin and paclitaxel, is an effective treatment in advanced malignant melanoma (64). Packiam et al. showed that CG0070 (GM-CSF expressing adenovirus) has a 47% CR rate at 6 months for all patients and 50% for patients with carcinoma-in situ (65).
Geletneky et al. evaluated H-1 parvovirus (H-1PV) effects in recurrent glioblastoma patients and reported microglia/macrophage activation and cytotoxic T-cell infiltration in the infected tumors, proposing initiation of the immunogenic response (66).
Andtbacka et al., in a phase III study, evaluated Talimogene laherparepvec (T-VEC) in stage IIIc and stage IV malignant melanoma. T-VEC was the first approved OVs against melanoma in a phase III clinical trial. This virus compared with GM-CSF showed a higher durable response rate and overall survival (67). In another newest phase III study, Talimogene laherparepvec was approved by the Food and Drug Administration (FDA) in the USA, European Union, and Australia (68).
Discussion
As a challenge in cancer therapy approaches (1), the exclusive features of oncolytic viruses have attracted plenty of researchers in recent years. OVs have the dramatic capability to selectively infect tumor cells leading to direct or indirect cancer cell death without harming normal cells (7). This study focused on some mechanisms employed by OVs against tumor cells, which are exactly various from virus to virus (Figure 1).

Figure 1 The main mechanism involved by oncolytic viruses.
According to most studies, OVs can target cancer cells and benefit from tumor conditions in favor of replication in infected cells, eventually leading to oncolysis. Indeed, tumor cells tend to resist apoptosis and translational suppression, which are both compatible with the growth of several viruses (7). One of the main actions of OVs is to take advantage of immune-evading properties of cancer cells to escape from recognition and destruction by the immune system. Antiviral processes in normal cells are associated with the interferon pathway in which the secretion of type I interferon (IFN) cytokine can trigger an antiviral response and induce ISGs to block viral replication (69). This subsequently leads to cell apoptosis, as it is known that the IFN-I signaling regulates the expression of proapoptotic genes such as tumor necrosis factor alpha (TNF-α), FAS ligand, and tumor necrosis factor-related apoptosis-inducing ligand (TRAIL) (70).
Regarding the IFN-I signaling is defective in most tumor cells, it makes tumor cells susceptible to being infected by some OVs including NDV, VSV, MYXV, and raccoon pox virus (71–73). García-Romero et al. showed that NDV was able to replicate in glioblastoma (GBM) cancer stem cells (CSCs) due to type I IFN gene loss occurring in more than 50% of patients. Infection of GBM with NDV represents oncolytic and immunostimulatory properties through the production of type I IFN in non-tumor cells such as tumor infiltrated macrophages and DC or other cells present at the tumor microenvironment (49). NDV therapy also declines CSCs self-renewing capacity to improve their differentiation ability and facilitate cancer therapy (49, 74). OVs can also benefit from the abnormal expression of the proto-oncogene RAS which generally occurs in normal cells but actives in tumor cells (75). OV infection outcomes can be affected by up-regulation of RAS in tumoral cells and further down-regulation of interferon-inducible genes due to activation of RAS/MEK signaling pathway that reduces viral response in tumoral cells (76). On the contrary with this attempt, Garant et al. demonstrated that reovirus could translocate and accumulate RAS into Golgi apparatus to increase apoptotic signaling events required for virus release (56). This highlighted that the outcomes of OVT are exclusively associated with the characteristics and type of OVs.
High expression of some viral receptors by cancer cells permits higher viral uptake in cancer cells than in normal ones. Some receptors such as CAR (77), laminin (78), CD155 (79), and CD46 (80) are overexpressed in various cancer cells which result in increased uptake of Ad (81), Sindbis virus (82), PV (83), and MV (84) respectively. Interestingly, some viral proteins are poisonous for neoplastic cells and can directly kill cells before viral replication. This was evidenced by the E3 death protein and E4orf4 proteins encoded by Ads and are toxic for cells that end in cytolysis at the time of virus exposure (3). However, deletion in specific viral genes can be another mechanism for the action of the OVs. These genes are necessary for the longevity of viruses in normal cells but not essential for viral activity in cancer cells. Thymidine kinase (TK) is an indispensable enzyme for nucleic acid metabolism encoded in infection with wild type vaccinia virus and enables the replicating of the virus in normal cells. Lister strain virus with TK gene deletion as a type of VV has shown a beneficial antitumor potency and cancer-selective replication in vivo since tumoral cells have a high TK content, which enables the virus to replicate in cancer cells regardless of the deletion in viral TK gene (85). In parallel with this study, Parato et al. analyzed the mechanism of cancer-selectivity by an engineered vaccina virus with TK deletion and epidermal growth factor (EGFR) and lac-Z transgenes observing the replication in tumor cells was related to activation of EGFR/RAS signaling, high cellular TK level and tumor cell resistance to IFN-I (52). These results displayed noticeably the beneficial implication of OVs with inherent and engineered mechanistic properties in cancer therapy approaches.
Oncolytic viruses may interfere with normal physiological process of tumor cells to induce the secretion of pro-inflammatory mediators or even lead to the exposure of tumor-associated antigens (TAA), pathogen-associated molecular patterns (PAMPs) and damage-associated molecular patterns (DAMPs) following apoptosis or oncolysis. These responses can also result in a change in tumor status from immune desert to inflamed status and further recruit a collection of immune cells such as cytotoxic T lymphocytes, dendritic cells, natural killer cells and phagocytic cells to induce immune cell death along with antiviral responses (86, 87).
Remarkably, most viruses continue their infection by expressing genes responsible for escaping the immune system and disseminating in host cells (88). Mutation in these genes can probably improve immune induction and thus increase the anti-tumoral responses regardless these mutations may reduce virus replication further (10). Thus, oncolytic viruses are often engineered to express various genes aided in the overall anti-tumor efficacy of the virus. Transgenes mostly include ranging from immune-stimulatory (IL-2, IL-4, IL-12 and GM-CSF) to pro-apoptotic (tumor necrosis factor alpha, p53 and TRAIL genes inserted into oncolytic viruses (87, 89–94). Interestingly, bystander effects of OVs through local release of cytokines can potentially cause immune response against nearby tumor cells even without direct antigen expression (95).
Furthermore, OVs can destroy tumor vasculature and impede sufficient intratumoral blood reserve, which is essential for tumor progression and metastasis (96). Breitbach et al. demonstrated that intravenous injection of JX-594, an engineered vaccine virus with TK deletion and overexpression of human granulocyte-monocyte colony-stimulating factor (hGM-CSF), led to replication of the virus in endothelial cells of the nearby tumor and disrupted tumor blood flow, which ultimately ended in intensive tumor necrosis within 5 days. Consistently, patients with advanced hepatocellular carcinoma, hypervascular and VEGFhigh tumor type, treated by JX-594 in phase II clinical trials confirmed the efficiency of the JX-594 OV in tumor vasculature disruption without toxicity to normal blood vessels in which inhibition of angiogenesis can passively result in tumor regression (97). This evidence may open promising technologies toward cancer therapy in a way tumor cells are targeted selectively and bypass the side effects of conventional approaches.
Recently, conditionally replication-competent adenoviruses (CRCAs) have been introduced as a successful method for cancer therapy. Sarkar et al. showed that Ad.PEG-E1A-mda-7, a cancer terminator virus (CTV), selectively replicated in cancer cells, inhibits their growth and induces apoptosis (98).
Qian et al. showed that ZD55 expressing melanoma differentiation-associated gene-7/interleukin-24 (ZD55-IL-24) affects B-lymphoblastic leukemia/lymphoma through upregulation of RNA-dependent protein kinase R, enhance phosphorylation of p38 mitogen-activated protein kinase, and induce of endoplasmic reticulum (ER) stress (99).
Azab et al. showed that Ad.5/3-CTV potently suppressed in vivo tumor growth in mouse (100).
Bhoopathi showed that Ad.5/3-CTV induces apoptosis through apoptosis-inducing factor (AIF) translocation into the nucleus, independent of the caspase-3/caspase-9 pathway (101).
In an interesting study, Bhoopathi et al. introduced a novel tripartite CTV “theranostic” adenovirus (TCTV) that targets virus replication, cytokine production, and imaging capabilities uniquely in cancer cells. This TCTV permits targeted treatment of tumors while monitoring tumor regression, with the potential to simultaneously detect metastasis due to the cancer-selective activity of reporter gene expression (102).
Greco et al. showed that ultrasound (US) contrast agents guided MB/Ad.mda-7 complexes to DU-145 cells successfully and eradicated not only targeted DU-145/Bcl-xL-therapy-resistant tumors but also nontargeted distant tumors (103).
T-VEC, adenovirus, and vaccinia virus are the most popular OVs in clinical trials. Approving T-VEC by FDA for the first time could pave the way for other OVs in the clinic. Oncolytic viruses have a broad therapeutic method; hence, their clinical development requires a multidisciplinary view. It is necessary to understand viral generation and viability in infected cells. To improve clinical trials, important factors such as viral entrance, replication, dissemination, oncolysis, and immune activation should be controlled. These factors can vary between tumor types and OVs. It is also critical to understand the immune composition of diverse cancers and the immunological repercussions of viro-immunotherapy.
Conclusion and Future Direction
Cancer is among the most important causes of mortality worldwide, and many chemotherapies and radiotherapy approaches do not have a specific effect on cancer cells and are sometimes accompanied by side effects. Today, a biological war has evolved against cancer by genetically modifying natural pathogens to activate them against neoplastic cells. OVT is a promising therapeutic option in cancer therapy. The mechanisms of action of OVs differ entirely from the mechanism of action of chemotherapy, radiotherapy, surgery, and embolization. They can result in success in the treatment of cancers that are resistant to other therapeutic modalities. Better understanding and acquiring comprehensive information regarding OV therapy and the biology of cancer is an essential step in assessing and controlling cancer programs.
Author Contributions
Conceptualization, WK and HE. Methodology, MF and RD. Validation, BJ. Data curation, MB. Writing—original draft preparation, HE and WK. Writing—review and editing, all. All authors have read and agreed to the published version of the manuscript.
Funding
This study was fully sponsored by Applied Virology Research Center; Baqiyatallah University of Medical Science; Tehran; Iran.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
Authors wish to thank all the staff of Applied Virology Research Center; Baqiyatallah University of Medical Science; Tehran, Iran, for their cooperation in implementing procedures.
References
1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global Cancer Statistics 2018: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA: Cancer J Clin (2018) 68(6):394–424. doi: 10.3322/caac.21492
2. Davis J, Fang B. Oncolytic Virotherapy for Cancer Treatment: Challenges and Solutions. J Gene Med (2005) 7(11):1380–9. doi: 10.1002/jgm.800
3. Chaurasiya S, Chen NG, Warner SG. Oncolytic Virotherapy Versus Cancer Stem Cells: A Review of Approaches and Mechanisms. Cancers (Basel) (2018) 10(4):124. doi: 10.3390/cancers10040124
4. Bell J, McFadden G. Viruses for Tumor Therapy. Cell Host Microbe (2014) 15(3):260–5. doi: 10.1016/j.chom.2014.01.002
5. Kelly E, Russell SJ. History of Oncolytic Viruses: Genesis to Genetic Engineering. Mol Ther (2007) 15(4):651–9. doi: 10.1038/sj.mt.6300108
6. Gujar S, Bell J, Diallo J-S. Snapshot: Cancer Immunotherapy With Oncolytic Viruses. Cell (2019) 176(5):1240–1240.e1. doi: 10.1016/j.cell.2019.01.051
7. Russell SJ, Peng K-W, Bell JC. Oncolytic Virotherapy. Nat Biotechnol (2012) 30(7):658. doi: 10.1038/nbt.2287
8. Kaufman HL, Kohlhapp FJ, Zloza A. Oncolytic Viruses: A New Class of Immunotherapy Drugs. Nat Rev Drug Discov (2015) 14(9):642–62. doi: 10.1038/nrd4663
9. Filley AC, Dey M. Immune System, Friend or Foe of Oncolytic Virotherapy? Front Oncol (2017) 7:106. doi: 10.3389/fonc.2017.00106
10. Chiocca EA, Rabkin SD. Oncolytic Viruses and Their Application to Cancer Immunotherapy. Cancer Immunol Res (2014) 2(4):295–300. doi: 10.1158/2326-6066.CIR-14-0015
11. Liu Y, Cai J, Liu W, Lin Y, Guo L, Liu X, et al. Intravenous Injection of the Oncolytic Virus M1 Awakens Antitumor T Cells and Overcomes Resistance to Checkpoint Blockade. Cell Death Dis (2020) 11(12):1–13. doi: 10.1038/s41419-020-03285-0
12. Rosewell Shaw A, Porter CE, Watanabe N, Tanoue K, Sikora A, Gottschalk S, et al. Adenovirotherapy Delivering Cytokine and Checkpoint Inhibitor Augments CAR T Cells Against Metastatic Head and Neck Cancer. Mol Ther (2017) 25(11):2440–51. doi: 10.1016/j.ymthe.2017.09.010
13. Zhang W, Zhang C, Tian W, Qin J, Chen J, Zhang Q, et al. Efficacy of an Oncolytic Adenovirus Driven by a Chimeric Promoter and Armed With Decorin Against Renal Cell Carcinoma. Hum Gene Ther (2020) 31(11-12):651–63. doi: 10.1089/hum.2019.352
14. Yang Y, Xu H, Huang W, Ding M, Xiao J, Yang D, et al. Targeting Lung Cancer Stem-Like Cells With TRAIL Gene Armed Oncolytic Adenovirus. J Cell Mol Med (2015) 19(5):915–23. doi: 10.1111/jcmm.12397
15. Tong Y, You L, Liu H, Li L, Meng H, Qian Q, et al. Potent Antitumor Activity of Oncolytic Adenovirus Expressing Beclin-1 via Induction of Autophagic Cell Death in Leukemia. Oncotarget (2013) 4(6):860–74. doi: 10.18632/oncotarget.1018
16. Eriksson M, Guse K, Bauerschmitz G, Virkkunen P, Tarkkanen M, Tanner M, et al. Oncolytic Adenoviruses Kill Breast Cancer Initiating CD44+CD24-/Low Cells. Mol Ther (2007) 15(12):2088–93. doi: 10.1038/sj.mt.6300300
17. Guo W, Zhu H, Zhang L, Davis J, Teraishi F, Roth JA, et al. Combination Effect of Oncolytic Adenovirotherapy and TRAIL Gene Therapy in Syngeneic Murine Breast Cancer Models. Cancer Gene Ther (2006) 13(1):82–90. doi: 10.1038/sj.cgt.7700863
18. Zhang X, Meng S, Zhang R, Ma B, Liu T, Yang Y, et al. GP73-Regulated Oncolytic Adenoviruses Possess Potent Killing Effect on Human Liver Cancer Stem-Like Cells. Oncotarget (2016) 7(20):29346–58. doi: 10.18632/oncotarget.8830
19. Zhang Y, Wang X, Li X, Xi D, Mao R, Wu X, et al. Potential Contribution of Increased Soluble IL-2R to Lymphopenia in COVID-19 Patients. Cell Mol Immunol (2020) 17(8):878–80. doi: 10.1038/s41423-020-0484-x
20. Davies JA, Marlow G, Uusi-Kerttula HK, Seaton G, Piggott L, Badder LM, et al. Efficient Intravenous Tumor Targeting Using the αvβ6 Integrin-Selective Precision Virotherapy Ad5(Null)-A20. Viruses (2021) 13(5):864.
21. Cerullo V, Pesonen S, Diaconu I, Escutenaire S, Arstila PT, Ugolini M, et al. Oncolytic Adenovirus Coding for Granulocyte Macrophage Colony-Stimulating Factor Induces Antitumoral Immunity in Cancer Patients. Cancer Res (2010) 70(11):4297–309. doi: 10.1158/0008-5472.CAN-09-3567
22. Bramante S, Koski A, Liikanen I, Vassilev L, Oksanen M, Siurala M, et al. Oncolytic Virotherapy for Treatment of Breast Cancer, Including Triple-Negative Breast Cancer. Oncoimmunology (2016) 5(2):e1078057. doi: 10.1080/2162402X.2015.1078057
23. Gürlevik E, Woller N, Strüver N, Schache P, Kloos A, Manns MP, et al. Selectivity of Oncolytic Viral Replication Prevents Antiviral Immune Response and Toxicity, But Does Not Improve Antitumoral Immunity. Mol Ther (2010) 18(11):1972–82. doi: 10.1038/mt.2010.163
24. Bauerschmitz GJ, Ranki T, Kangasniemi L, Ribacka C, Eriksson M, Porten M, et al. Tissue-Specific Promoters Active in CD44+CD24-/Low Breast Cancer Cells. Cancer Res (2008) 68(14):5533–9. doi: 10.1158/0008-5472.CAN-07-5288
25. González M, van de Ven R, Haan H, Sluijs J, Dong W, Beusechem V, et al. Oncolytic Adenovirus ORCA-010 Increases the Type-1 T Cell Stimulatory Capacity of Melanoma-Conditioned Dendritic Cells. Clin Exp Immunol (2020) 201:145–60.
26. Yano S, Tazawa H, Hashimoto Y, Shirakawa Y, Kuroda S, Nishizaki M, et al. A Genetically Engineered Oncolytic Adenovirus Decoys and Lethally Traps Quiescent Cancer Stem-Like Cells in s/G2/M Phases. Clin Cancer Res (2013) 19(23):6495–505. doi: 10.1158/1078-0432.CCR-13-0742
27. Chen CY, Wang PY, Hutzen B, Sprague L, Swain HM, Love JK, et al. Cooperation of Oncolytic Herpes Virotherapy and PD-1 Blockade in Murine Rhabdomyosarcoma Models. Sci Rep (2017) 7(1):2396. doi: 10.1038/s41598-017-02503-8
28. Ghouse SM, Nguyen H-M, Bommareddy PK, Guz-Montgomery K, Saha D. Oncolytic Herpes Simplex Virus Encoding IL12 Controls Triple-Negative Breast Cancer Growth and Metastasis. Front Oncol (2020) 10:384. doi: 10.3389/fonc.2020.00384
29. Zhang W, Hu X, Liang J, Zhu Y, Zeng B, Feng L, et al. Ohsv2 can Target Murine Colon Carcinoma by Altering the Immune Status of the Tumor Microenvironment and Inducing Antitumor Immunity. Mol Ther Oncolytics (2020) 16:158–71. doi: 10.1016/j.omto.2019.12.012
30. Benencia F, Courreges M, Fraser N, Coukos G. Herpes Virus Oncolytic Therapy Reverses Tumor Immune Dysfunction and Facilitates Tumor Antigen Presentation. Cancer Biol Ther (2008) 7:1194–205. doi: 10.4161/cbt.7.8.6216
31. Li H, Dutuor A, Tao L, Fu X, Zhang X. Virotherapy With a Type 2 Herpes Simplex Virus–Derived Oncolytic Virus Induces Potent Antitumor Immunity Against Neuroblastoma. Clin Cancer Res (2007) 13(1):316–22. doi: 10.1158/1078-0432.CCR-06-1625
32. Bommareddy PK, Zloza A, Rabkin SD, Kaufman HL. Oncolytic Virus Immunotherapy Induces Immunogenic Cell Death and Overcomes STING Deficiency in Melanoma. OncoImmunology (2019) 8(7):e1591875. doi: 10.1080/2162402X.2019.1591875
33. Sobol PT, Boudreau JE, Stephenson K, Wan Y, Lichty BD, Mossman KL. Adaptive Antiviral Immunity is a Determinant of the Therapeutic Success of Oncolytic Virotherapy. Mol Ther (2011) 19(2):335–44. doi: 10.1038/mt.2010.264
34. Warner SG, Haddad D, Au J, Carson JS, O'Leary MP, Lewis C, et al. Oncolytic Herpes Simplex Virus Kills Stem-Like Tumor-Initiating Colon Cancer Cells. Mol Ther Oncolytics (2016) 3:16013. doi: 10.1038/mto.2016.13
35. Wakimoto H, Kesari S, Farrell CJ, Curry WT Jr., Zaupa C, Aghi M, et al. Human Glioblastoma-Derived Cancer Stem Cells: Establishment of Invasive Glioma Models and Treatment With Oncolytic Herpes Simplex Virus Vectors. Cancer Res (2009) 69(8):3472–81. doi: 10.1158/0008-5472.CAN-08-3886
36. Harrington KJ, Hingorani M, Tanay MA, Hickey J, Bhide SA, Clarke PM, et al. Phase I/II Study of Oncolytic HSVGM-CSF in Combination With Radiotherapy and Cisplatin in Untreated Stage III/IV Squamous Cell Cancer of the Head and Neck. Clin Cancer Res (2010) 16(15):4005–15. doi: 10.1158/1078-0432.CCR-10-0196
37. Hu JC, Coffin RS, Davis CJ, Graham NJ, Groves N, Guest PJ, et al. A Phase I Study of Oncovexgm-CSF, a Second-Generation Oncolytic Herpes Simplex Virus Expressing Granulocyte Macrophage Colony-Stimulating Factor. Clin Cancer Res (2006) 12(22):6737–47. doi: 10.1158/1078-0432.CCR-06-0759
38. Senzer NN, Kaufman HL, Amatruda T, Nemunaitis M, Reid T, Daniels G, et al. Phase II Clinical Trial of a Granulocyte-Macrophage Colony-Stimulating Factor-Encoding, Second-Generation Oncolytic Herpesvirus in Patients With Unresectable Metastatic Melanoma. J Clin Oncol (2009) 27(34):5763–71. doi: 10.1200/JCO.2009.24.3675
39. Xia M, Luo D, Dong J, Zheng M, Meng G, Wu J, et al. Graphene Oxide Arms Oncolytic Measles Virus for Improved Effectiveness of Cancer Therapy. J Exp Clin Cancer Res (2019) 38(1):408. doi: 10.1186/s13046-019-1410-x
40. Bach P, Abel T, Hoffmann C, Gal Z, Braun G, Voelker I, et al. Specific Elimination of CD133+ Tumor Cells With Targeted Oncolytic Measles Virus. Cancer Res (2013) 73(2):865–74. doi: 10.1158/0008-5472.CAN-12-2221
41. Li H, Peng K-W, Dingli D, Kratzke R, Russell SJ. Oncolytic Measles Viruses Encoding Interferon β and the Thyroidal Sodium Iodide Symporter Gene for Mesothelioma Virotherapy. Cancer Gene Ther (2010) 17(8):550–8. doi: 10.1038/cgt.2010.10
42. Ong HT, Hasegawa K, Dietz AB, Russell SJ, Peng KW. Evaluation of T Cells as Carriers for Systemic Measles Virotherapy in the Presence of Antiviral Antibodies. Gene Ther (2007) 14(4):324–33. doi: 10.1038/sj.gt.3302880
43. Lal G, Rajala MS. Combination of Oncolytic Measles Virus Armed With Bnip3, a Pro-Apoptotic Gene and Paclitaxel Induces Breast Cancer Cell Death. Front Oncol (2019) 8:676. doi: 10.3389/fonc.2018.00676
44. Abdullah SA, Al-Shammari AM, Lateef SA. Attenuated Measles Vaccine Strain Have Potent Oncolytic Activity Against Iraqi Patient Derived Breast Cancer Cell Line. Saudi J Biol Sci (2020) 27(3):865–72. doi: 10.1016/j.sjbs.2019.12.015
45. Heinzerling L, Künzi V, Oberholzer P, Kündig T, Naim H, Dummer R. Oncolytic Measles Virus in Cutaneous T-Cell Lymphomas Mounts Antitumor Immune Responses In Vivo and Targets Interferon-Resistant Tumor Cells. Blood (2005) 106:2287–94. doi: 10.1182/blood-2004-11-4558
46. Hu L, Sun S, Wang T, Li Y, Jiang K, Lin G, et al. Oncolytic Newcastle Disease Virus Triggers Cell Death of Lung Cancer Spheroids and Is Enhanced by Pharmacological Inhibition of Autophagy. Am J Cancer Res (2015) 5(12):3612–23.
47. Zamarin D, Holmgaard RB, Subudhi SK, Park JS, Mansour M, Palese P, et al. Localized Oncolytic Virotherapy Overcomes Systemic Tumor Resistance to Immune Checkpoint Blockade Immunotherapy. Sci Transl Med (2014) 6(226):226ra32. doi: 10.1126/scitranslmed.3008095
48. Ye T, Jiang K, Wei L, Barr MP, Xu Q, Zhang G, et al. Oncolytic Newcastle Disease Virus Induces Autophagy-Dependent Immunogenic Cell Death in Lung Cancer Cells. Am J Cancer Res (2018) 8(8):1514.
49. García-Romero N, Palacيn-Aliana I, Esteban-Rubio S, Madurga R, Rius-Rocabert S, Carriَn-Navarro J, et al. Newcastle Disease Virus (NDV) Oncolytic Activity in Human Glioma Tumors Is Dependent on CDKN2A-Type I IFN Gene Cluster Codeletion. Cells (2020) 9(6):1405. doi: 10.3390/cells9061405
50. Wang G, Kang X, Chen KS, Jehng T, Jones L, Chen J, et al. An Engineered Oncolytic Virus Expressing PD-L1 Inhibitors Activates Tumor Neoantigen-Specific T Cell Responses. Nat Commun (2020) 11(1):1–14. doi: 10.1038/s41467-020-15229-5
51. Nakao S, Arai Y, Tasaki M, Yamashita M, Murakami R, Kawase T, et al. Intratumoral Expression of IL-7 and IL-12 Using an Oncolytic Virus Increases Systemic Sensitivity to Immune Checkpoint Blockade. Sci Trans Med (2020) 12(526):eaax7992. doi: 10.1126/scitranslmed.aax7992
52. Parato KA, Breitbach CJ, Le Boeuf F, Wang J, Storbeck C, Ilkow C, et al. The Oncolytic Poxvirus JX-594 Selectively Replicates in and Destroys Cancer Cells Driven by Genetic Pathways Commonly Activated in Cancers. Mol Ther (2012) 20(4):749–58. doi: 10.1038/mt.2011.276
53. Liu Y, Li K, Zhu W-b, Zhang H, Huang W-t, Liu X-c, et al. Suppression of CCDC6 Sensitizes Tumor to Oncolytic Virus M1. Neoplasia (2021) 23(1):158–68. doi: 10.1016/j.neo.2020.12.003
54. Feist M, Zhu Z, Dai E, Ma C, Liu Z, Giehl E, et al. Oncolytic Virus Promotes Tumor-Reactive Infiltrating Lymphocytes for Adoptive Cell Therapy. Cancer Gene Ther (2020) p:1–14.
55. Ochiai H, Moore SA, Archer GE, Okamura T, Chewning TA, Marks JR, et al. Treatment of Intracerebral Neoplasia and Neoplastic Meningitis With Regional Delivery of Oncolytic Recombinant Poliovirus. Clin Cancer Res (2004) 10(14):4831–8. doi: 10.1158/1078-0432.CCR-03-0694
56. Garant K, Shmulevitz M, Pan L, Daigle R, Ahn D, Gujar S, et al. Oncolytic Reovirus Induces Intracellular Redistribution of Ras to Promote Apoptosis and Progeny Virus Release. Oncogene (2016) 35(6):771–82. doi: 10.1038/onc.2015.136
57. Ma J, Ramachandran M, Jin C, Quijano-Rubio C, Martikainen M, Yu D, et al. Characterization of Virus-Mediated Immunogenic Cancer Cell Death and the Consequences for Oncolytic Virus-Based Immunotherapy of Cancer. Cell Death Dis (2020) 11(1):1–15. doi: 10.1038/s41419-020-2236-3
58. Streby KA, Geller JI, Currier MA, Warren PS, Racadio JM, Towbin AJ, et al. Intratumoral Injection of HSV1716, an Oncolytic Herpes Virus, Is Safe and Shows Evidence of Immune Response and Viral Replication in Young Cancer Patients. Clin Cancer Res (2017) 23(14):3566–74. doi: 10.1158/1078-0432.CCR-16-2900
59. Desjardins A, Gromeier M, Herndon JE, Beaubier N, Bolognesi DP, Friedman AH, et al. Recurrent Glioblastoma Treated With Recombinant Poliovirus. N Engl J Med (2018) 379: (2):150–61. doi: 10.1056/NEJMoa1716435
60. Garcia-Carbonero R, Salazar R, Duran I, Osman-Garcia I, Paz-Ares L, Bozada JM, et al. Phase 1 Study of Intravenous Administration of the Chimeric Adenovirus Enadenotucirev in Patients Undergoing Primary Tumor Resection. J Immunother Cancer (2017) 5(1):71. doi: 10.1186/s40425-017-0277-7
61. Husseini F, Delord JP, Fournel-Federico C, Guitton J, Erbs P, Homerin M, et al. Vectorized Gene Therapy of Liver Tumors: Proof-of-Concept of TG4023 (MVA-FCU1) in Combination With Flucytosine. Ann Oncol (2017) 28(1):169–74. doi: 10.1093/annonc/mdw440
62. Dispenzieri A, Tong C, LaPlant B, Lacy MQ, Laumann K, Dingli D, et al. Phase I Trial of Systemic Administration of Edmonston Strain of Measles Virus Genetically Engineered to Express the Sodium Iodide Symporter in Patients With Recurrent or Refractory Multiple Myeloma. Leukemia (2017) 31(12):2791–8. doi: 10.1038/leu.2017.120
63. Cohn DE, Sill MW, Walker JL, O'Malley D, Nagel CI, Rutledge TL, et al. Randomized Phase IIB Evaluation of Weekly Paclitaxel Versus Weekly Paclitaxel With Oncolytic Reovirus (Reolysin®) in Recurrent Ovarian, Tubal, or Peritoneal Cancer: An NRG Oncology/Gynecologic Oncology Group Study. Gynecol Oncol (2017) 146(3):477–83. doi: 10.1016/j.ygyno.2017.07.135
64. Mahalingam D, Fountzilas C, Moseley J, Noronha N, Tran H, Chakrabarty R, et al. A Phase II Study of REOLYSIN(®) (Pelareorep) in Combination With Carboplatin and Paclitaxel for Patients With Advanced Malignant Melanoma. Cancer Chemother Pharmacol (2017) 79(4):697–703. doi: 10.1007/s00280-017-3260-6
65. Packiam VT, Lamm DL, Barocas DA, Trainer A, Fand B, Davis RL, et al. An Open Label, Single-Arm, Phase II Multicenter Study of the Safety and Efficacy of CG0070 Oncolytic Vector Regimen in Patients With BCG-Unresponsive non-Muscle-Invasive Bladder Cancer: Interim Results. Urol Oncol (2018) 36(10):440–7. doi: 10.1016/j.urolonc.2017.07.005
66. Geletneky K, Hajda J, Angelova AL, Leuchs B, Capper D, Bartsch AJ, et al. Oncolytic H-1 Parvovirus Shows Safety and Signs of Immunogenic Activity in a First Phase I/Iia Glioblastoma Trial. Mol Ther (2017) 25(12):2620–34. doi: 10.1016/j.ymthe.2017.08.016
67. Andtbacka RH, Kaufman HL, Collichio F, Amatruda T, Senzer N, Chesney J, et al. Talimogene Laherparepvec Improves Durable Response Rate in Patients With Advanced Melanoma. J Clin Oncol (2015) 33(25):2780–8. doi: 10.1200/JCO.2014.58.3377
68. Chesney J, Awasthi S, Curti B, Hutchins L, Linette G, Triozzi P, et al. Phase Iiib Safety Results From an Expanded-Access Protocol of Talimogene Laherparepvec for Patients With Unresected, Stage IIIB-IVM1c Melanoma. Melanoma Res (2018) 28(1):44–51. doi: 10.1097/CMR.0000000000000399
69. Boasso A. Type I Interferon at the Interface of Antiviral Immunity and Immune Regulation: The Curious Case of HIV-1. Scientifica (2013) 2013:580968. doi: 10.1155/2013/580968
70. Apelbaum A, Yarden G, Warszawski S, Harari D, Schreiber G. Type I Interferons Induce Apoptosis by Balancing Cflip and Caspase-8 Independent of Death Ligands. Mol Cell Biol (2013) 33(4):800–14. doi: 10.1128/MCB.01430-12
71. Stojdl DF, Lichty B, Knowles S, Marius R, Atkins H, Sonenberg N, et al. Exploiting Tumor-Specific Defects in the Interferon Pathway With a Previously Unknown Oncolytic Virus. Nat Med (2000) 6(7):821–5. doi: 10.1038/77558
72. Everts B, van der Poel HG. Replication-Selective Oncolytic Viruses in the Treatment of Cancer. Cancer Gene Ther (2005) 12(2):141–61. doi: 10.1038/sj.cgt.7700771
73. Evgin L, Vنhن-Koskela M, Rintoul J, Falls T, Le Boeuf F, Barrett JW, et al. Potent Oncolytic Activity of Raccoonpox Virus in the Absence of Natural Pathogenicity. Mol Ther (2010) 18(5):896–902. doi: 10.1038/mt.2010.14
74. Cho D-Y, Lin S-Z, Yang W-K, Lee H-C, Hsu D-M, Lin H-L, et al. Targeting Cancer Stem Cells for Treatment of Glioblastoma Multiforme. Cell Transplant (2013) 22(4):731–9. doi: 10.3727/096368912X655136
75. Balachandran S, Porosnicu M, Barber GN. Oncolytic Activity of Vesicular Stomatitis Virus is Effective Against Tumors Exhibiting Aberrant P53, Ras, or Myc Function and Involves the Induction of Apoptosis. J Virol (2001) 75(7):3474–9. doi: 10.1128/JVI.75.7.3474-3479.2001
76. Christian SL, Zu D, Licursi M, Komatsu Y, Pongnopparat T, Codner DA, et al. Suppression of IFN-Induced Transcription Underlies IFN Defects Generated by Activated Ras/MEK in Human Cancer Cells. PloS One (2012) 7(9):e44267. doi: 10.1371/journal.pone.0044267
77. Martin T, Watkins G, Jiang WG. The Coxsackie-Adenovirus Receptor has Elevated Expression in Human Breast Cancer. Clin Exp Med (2005) 5(3):122–8. doi: 10.1007/s10238-005-0076-1
78. Sanjuán X, Fernández Pl, Miquel R, Muñoz J, Castronovo V, Ménard S. Overexpression of the 67-Kd Laminin Receptor Correlates With Tumour Progression in Human Colorectal Carcinoma. J Pathol (1996) 179(4):376–80. doi: 10.1002/(SICI)1096-9896(199608)179:4<376::AID-PATH591>3.0.CO;2-V
79. Masson D, Jarry A, Baury B, Blanchardie P, Laboisse C, Lustenberger P, et al. Overexpression of the CD155 Gene in Human Colorectal Carcinoma. Gut (2001) 49(2):236–40. doi: 10.1136/gut.49.2.236
80. Anderson BD, Nakamura T, Russell SJ, Peng K-W. High CD46 Receptor Density Determines Preferential Killing of Tumor Cells by Oncolytic Measles Virus. Cancer Res (2004) 64(14):4919–26. doi: 10.1158/0008-5472.CAN-04-0884
81. Kim J-S, Lee S-H, Cho Y-S, Choi J-J, Kim YH, Lee J-H. Enhancement of the Adenoviral Sensitivity of Human Ovarian Cancer Cells by Transient Expression of Coxsackievirus and Adenovirus Receptor (CAR). Gynecol Oncol (2002) 85(2):260–5. doi: 10.1006/gyno.2002.6607
82. Tseng J-C, Levin B, Hirano T, Yee H, Pampeno C, Meruelo D. In Vivo Antitumor Activity of Sindbis Viral Vectors. J Natl Cancer Inst (2002) 94(23):1790–802. doi: 10.1093/jnci/94.23.1790
83. Ohka S, Matsuda N, Tohyama K, Oda T, Morikawa M, Kuge S, et al. Receptor (CD155)-Dependent Endocytosis of Poliovirus and Retrograde Axonal Transport of the Endosome. J Virol (2004) 78(13):7186–98. doi: 10.1128/JVI.78.13.7186-7198.2004
84. Dörig RE, Marcil A, Chopra A, Richardson CD, et al. The Human CD46 Molecule is a Receptor for Measles Virus (Edmonston Strain). Cell (1993) 75(2):295–305. doi: 10.1016/0092-8674(93)80071-L
85. Hughes J, Wang P, Alusi G, Shi H, Chu Y, Wang J, et al. Lister Strain Vaccinia Virus With Thymidine Kinase Gene Deletion is a Tractable Platform for Development of a New Generation of Oncolytic Virus. Gene Ther (2015) 22(6):476–84. doi: 10.1038/gt.2015.13
86. Bommareddy PK, Shettigar M, Kaufman HL. Integrating Oncolytic Viruses in Combination Cancer Immunotherapy. Nat Rev Immunol (2018) 18(8):498. doi: 10.1038/s41577-018-0014-6
87. Lichty BD, Breitbach CJ, Stojdl DF, Bell JC. Going Viral With Cancer Immunotherapy. Nat Rev Cancer (2014) 14(8):559–67. doi: 10.1038/nrc3770
88. Versteeg GA, García-Sastre A. Viral Tricks to Grid-Lock the Type I Interferon System. Curr Opin Microbiol (2010) 13(4):508–16. doi: 10.1016/j.mib.2010.05.009
89. Zhang S, Huang W, Zhou X, Zhao Q, Wang Q, Jia B. Seroprevalence of Neutralizing Antibodies to Human Adenoviruses Type-5 and Type-26 and Chimpanzee Adenovirus Type-68 in Healthy Chinese Adults. J Med Virol (2013) 85(6):1077–84. doi: 10.1002/jmv.23546
90. Nwanegbo E, Vardas E, Gao W, Whittle H, Sun H, Rowe D, et al. Prevalence of Neutralizing Antibodies to Adenoviral Serotypes 5 and 35 in the Adult Populations of the Gambia, South Africa, and the United States. Clin Diagn Lab Immunol (2004) 11(2):351–7. doi: 10.1128/CDLI.11.2.351-357.2004
91. Harada JN, Berk AJ. P53-Independent and-Dependent Requirements for E1B-55K in Adenovirus Type 5 Replication. J Virol (1999) 73(7):5333–44. doi: 10.1128/JVI.73.7.5333-5344.1999
92. Goodrum FD, Ornelles DA. P53 Status Does Not Determine Outcome of E1B 55-Kilodalton Mutant Adenovirus Lytic Infection. J Virol (1998) 72(12):9479–90. doi: 10.1128/JVI.72.12.9479-9490.1998
93. Ries S, Korn W. ONYX-015: Mechanisms of Action and Clinical Potential of a Replication-Selective Adenovirus. Br J Cancer (2002) 86(1):5–11. doi: 10.1038/sj.bjc.6600006
94. Goodrum FD, Ornelles DA. The Early Region 1B 55-Kilodalton Oncoprotein of Adenovirus Relieves Growth Restrictions Imposed on Viral Replication by the Cell Cycle. J Virol (1997) 71(1):548–61. doi: 10.1128/jvi.71.1.548-561.1997
95. Schietinger A, Philip M, Liu RB, Schreiber K, Schreiber H. Bystander Killing of Cancer Requires the Cooperation of CD4+ and CD8+ T Cells During the Effector Phase. J Exp Med (2010) 207(11):2469–77. doi: 10.1084/jem.20092450
96. Breitbach CJ, Paterson JM, Lemay CG, Falls TJ, McGuire A, Parato KA, et al. Targeted Inflammation During Oncolytic Virus Therapy Severely Compromises Tumor Blood Flow. Mol Ther (2007) 15(9):1686–93. doi: 10.1038/sj.mt.6300215
97. Breitbach CJ, Arulanandam R, De Silva N, Thorne SH, Patt R, Daneshmand M, et al. Oncolytic Vaccinia Virus Disrupts Tumor-Associated Vasculature in Humans. Cancer Res (2013) 73(4):1265–75. doi: 10.1158/0008-5472.CAN-12-2687
98. Sarkar D, Su Zz, Park ES, Vozhilla N, Dent P, Curiel DT, et al. A Cancer Terminator Virus Eradicates Both Primary and Distant Human Melanomas. Cancer Gene Ther (2008) 15(5):293–302. doi: 10.1038/cgt.2008.14
99. Qian W, Liu J, Tong Y, Yan S, Yang C, Yang M, et al. Enhanced Antitumor Activity by a Selective Conditionally Replicating Adenovirus Combining With MDA-7/Interleukin-24 for B-Lymphoblastic Leukemia via Induction of Apoptosis. Leukemia (2008) 22(2):361–9. doi: 10.1038/sj.leu.2405034
100. Azab BM, Dash R, Das SK, Bhutia SK, Sarkar S, Shen XN, et al. Enhanced Prostate Cancer Gene Transfer and Therapy Using a Novel Serotype Chimera Cancer Terminator Virus (Ad.5/3-CTV). J Cell Physiol (2014) 229(1):34–43.
101. Bhoopathi P, Lee N, Pradhan AK, Shen XN, Das SK, Sarkar D, et al. Mda-7/IL-24 Induces Cell Death in Neuroblastoma Through a Novel Mechanism Involving AIF and ATM. Cancer Res (2016) 76(12):3572–82. doi: 10.1158/0008-5472.CAN-15-2959
102. Bhoopathi P, Lee N, Pradhan AK, Shen XN, Das SK, Sarkar D, et al. Theranostic Tripartite Cancer Terminator Virus for Cancer Therapy and Imaging. Cancers (Basel) (2021) 13: (4):857. doi: 10.3390/cancers13040857
Keywords: oncolytic virus, cancer immunotherapy, cancer vaccine, targeted treatment, immune checkpoint
Citation: Kooti W, Esmaeili Gouvarchin Ghaleh H, Farzanehpour M, Dorostkar R, Jalali Kondori B and Bolandian M (2021) Oncolytic Viruses and Cancer, Do You Know the Main Mechanism? Front. Oncol. 11:761015. doi: 10.3389/fonc.2021.761015
Received: 19 August 2021; Accepted: 22 November 2021;
Published: 22 December 2021.
Edited by:
Massimo Fantini, Precision Biologics, Inc., United StatesReviewed by:
Praveen Bommareddy, Rutgers, The State University of New Jersey, United StatesPaul B. Fisher, Virginia Commonwealth University, United States
Copyright © 2021 Kooti, Esmaeili Gouvarchin Ghaleh, Farzanehpour, Dorostkar, Jalali Kondori and Bolandian. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hadi Esmaeili Gouvarchin Ghaleh, h.smaili69@yahoo.com