 Isabela N. de Almeida1
Isabela N. de Almeida1 Lida J. de Assis Figueredo1
Lida J. de Assis Figueredo1 Valéria M. Soares1Maria C. Vater2Suely Alves2Wânia da Silva Carvalho3Afrânio L. Kritski2Silvana S. de Miranda1*
Valéria M. Soares1Maria C. Vater2Suely Alves2Wânia da Silva Carvalho3Afrânio L. Kritski2Silvana S. de Miranda1*- 1Research Laboratory in Mycobacteria, School of Medicine of the Federal University of Minas Gerais, Belo Horizonte, Brazil
- 2Research Center for Tuberculosis, Academic Program in Tuberculosis, School of Medicine of the Federal University of Rio de Janeiro, Rio de Janeiro, Brazil
- 3School of Pharmacy of the Federal University of Minas Gerais, Belo Horizonte, Brazil
At a global level, with the increase in healthcare costs, there is a need to assess the economic impact of the incorporation of new technologies in different health disorders in different countries. There is scarce information regarding costs incurred with the use of current or new diagnostic tests for tuberculosis or from the vantage point of their incorporation within the healthcare systems of high-burden countries. The present study aimed to assess the mean cost and the activity based cost of the laboratory diagnosis for tuberculosis by means of conventional techniques and from the Detect TB®LabTest molecular test kit in a general high-complexity hospital of the public health system in Brazil. Cost analysis was performed by means of primary data, collected in the Mycobacteria and Molecular Biology Laboratory in 2013. The mean cost and activity based cost were, respectively, U$10.06/U$5.61 for centrifuged bacilloscopy by Ziehl Neelsen (ZN) and Auramine (AU); U$7.42/U$4.15 for direct bacilloscopy by ZN; U$27.38/U$16.50 for culture in a Loweinstein-Jensen solid medium; and U$115.74/U$73.46 for the Detect TB®LabTest Kit. The calculation of the ABC should be used in making decisions by administrators to be the best method of assessing the costs of conventional techniques and molecular method for providing the real value of the tests. So it is need to calculate the ABC, and not of the mean cost, in various scenarios before incorporating new technologies in health institutions.
Introduction
Tuberculosis (TB) remains as one of the central problems of world public health. In 2015, in Brazil, some 71,221 new cases were notified, with 73% confirmed by laboratory diagnosis (bacilloscopy or culture), and 71% presented treatment success (WHO, 2016). The diagnosis of TB by means of high-quality mycobacteriological exams associated with clinical/epidemiological and radiological criteria represent efficient strategies to TB control (BRASIL, 2010). However, these conventional methods present some disadvantages, such as low sensitivity and specificity, as in the case of the bacilloscopy and chest X-ray (The International Journal of Tuberculosis, and Lung Disease [IJTLD], 2012).
The culture, considered the “gold standard”, has limitations, which are inherently linked to the time needed to obtain the results and the need for a robust infrastructure in the laboratory, which is limited to reference centers (Gholoobi et al., 2014). Molecular diagnosis is reported to have higher sensitivity than bacilloscopy and faster than cultures (Almeida et al., 2015). As of 2008, the World Health Organization (WHO) endorsed the use of molecular methods to detect TB and drug-resistant TB as an alternative to a faster diagnosis of TB (WHO, 2008).
These methods present a high specificity, though lower sensitivity in patients with negative bacilloscopy results. The most commercial molecular methods used to detect TB and drug-resistant TB are the GenoType®MTBDRplus (Biomeuriéx) and the Xpert MTB/RIF® (Cepheid). One major advantage of these methods is that these can provide results more quickly than the culture, yet the greatest disadvantage is that they are too expensive and too complex for routine use in contexts with limited resources (Steingart et al., 2015). In Brazil, the Xpert MTB/RIF® was introduced into the public system by recommendation from the Ministry of Health in 2014. A new kit developed in Brazil (Detect TB®LabTestKit, MG, Brazil) has been used for the molecular diagnoses of the Mycobacterium tuberculosis Complex (MTBC) (BRASIL, 2011; Michelon et al., 2011; Schimd et al., 2014).
Nevertheless, in high-burden countries, data concerning the costs incurred with the use of diagnostic tests for TB are scarce in routine conditions, and the TB control programs require decision-making based on algorithms of diagnoses that consider the laboratory costs, as well as those related to clinical treatment and the local prevalence of TB (Shah et al., 2013). At the global level, with the increase in healthcare costs, there is a growing need to assess TB diagnostic methods, both current methods and those planned for future implementation in different countries (Silva, 2003; BRASIL, 2011).
While there are large numbers of studies on accuracy of TB diagnostic tests, there are few studies that are focused on cost. Study conducted in Thailand demonstrated that the costs by Ziehl Neelsen (ZN) and Auramine (AU) were very close. In Zambia compared the values of the culture by different techniques in liquid and solid media found few variations. In South Africa, the cost of molecular method (Xpert MTB/RIF®) was similar to conventional automated liquid culture-based methods and the GenoType®MTBDRplus was higher (Mueller et al., 2008; Sohn et al., 2009a,b; Shah et al., 2013).
Within the methodologies used to calculate the costs of health services, activity based costing (ABC) is appropriate for complex organizations, in which the products consume resources in a highly heterogeneous manner, such as occurs in hospitals. The benefits of ABC are many, especially because it improves managerial decisions; facilitates the determination of relevant costs; allows for the identification of actions geared toward the reduction of overhead costs; provides a greater precision in product costs; determines the costs of services/products; offers support in the negotiation of contracts; provides support in the increase in revenue, helping customers to understand the cost reductions as consequence of the use of their products and services; gives support for benchmarking; and determines the remainder of shared services (BRASIL, 2006).
A study was recently conducted in Brazil aimed at supplying subsidies for managers to identify the main cost guidelines and possible gains in efficiency and effectiveness when adopting the XpertMTB/RIF, using the ABC as a cost methodology to pinpoint the advantage of being able to observe a significant quantity of tests, thus making it possible to identify a standard cost and conduct a detailed inventory of the cost items (Pinto et al., 2015).
In the Brazilian context, considering that the majority of reference laboratories are structured to conduct bacilloscopies and cultures to detect mycobacteria, it thus becomes necessary to measure the real costs of both these technologies and the Detect TB® kit, the only national molecular method (BRASIL, 2010; Michelon et al., 2011).
Therefore, the present study aimed to assess the mean cost and ABC of the laboratory diagnosis of TB by means of conventional techniques and the Detect TB®LabTest molecular test kit in a high-complexity general hospital from the public health system.
Materials and Methods
Design and Study Site
This study’s cost analysis was performed by means of primary data collected in the Research Laboratory in Mycobacteria (RLM) of the Federal University of Minas Gerais (FUMG) School of Medicine (SM), as well as in the Molecular Biology and Public Health Laboratory (MBPH) of the FUMG School of Pharmacy (SP), from January to December 2013. At RLM, TB laboratory diagnoses are conducted on patients who receive medical care at the hospital complex of the Clinical Hospital (CH)/FUMG, a public and general university hospital that conducts educational, research, and medical care activities. CH/FUMG is a reference hospital in the municipal and state health system concerning medical care provided to patients with mid- and high-complexity pathologies, and consists of one hospital unit and seven outpatient care centers (UFMG, 2015).
Study’s Cost Analysis
The costs of TB laboratory diagnoses (bacilloscopy and culture) were evaluated based on two methodologies: by mean cost and by activity. Mean Cost is calculated through the total cost divided by the quantity produced over a determined period of time (BRASIL, 2006), which, in this study, considered the quantity of exams conducted per month.
The ABC is calculated considering an activity as the denominator for the calculation of the unit cost per activity, rather than the real consumed quantity. The aim of this procedure is to avoid fluctuations in the calculation of the activity’s unit cost based on the variation of the real processed quantity. The basic principle of this system is to make the largest possible number of proportional and non-proportional costs more direct, through cost guidelines, as illustrated in Figure 1 (Khoury and Ancelevicz, 2000).
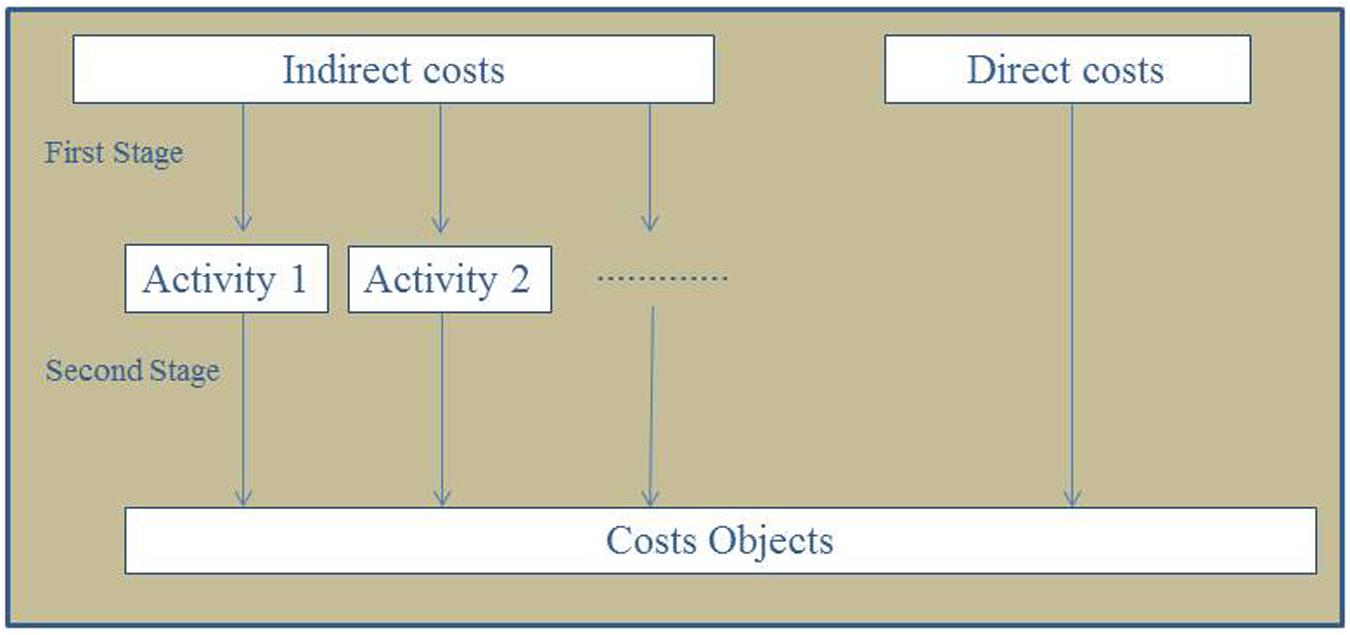
FIGURE 1. Cost flow in the activity based costing systems. ∗Activity = performing one diagnostic test (bacilloscopy, culture, or Detect TB®).
To calculate both costs (mean/ABC), this study verified the values of all cost components of the assessed diagnostic methods, such as: infrastructure, equipment, inputs, personal protective equipment (PPE), human resources, and the maintenance of biosafety laboratories (B3), according to the daily routine at RLM/SM/FUMG in 2013. These data were collected by consulting the purchasing, human resources, and maintenance sectors after prior institutional authorization and study approval by the Ethics Committee (CAAE -11821913.6.000.5257, CAAE – 0223.2412.7.1001.5149, DEPE/CH, protocol number 139/12).
Diagnostic Tests of Tuberculosis Laboratory Routine
The RLM/SM/FUMG counts on two work flows to perform a bacilloscopy: (1) direct bacilloscopy by ZN in samples from emergency rooms and wards at the FUMG Clinical Hospital for the release of exam results in up to four hours; (2) centrifuged bacilloscopy to execute staining by means of the ZN method and fluorescent (AU) of all of the other samples that arrive from the Hospital Complex (out-patient care), including the samples in which the direct bacilloscopy was performed.
The culture is performed in a Loweinstein-Jensen (LJ) solid medium, using four tubes –two tubes without drugs and two with p-Nitrobenzoic acid (PNB) and 2-thyophenecarboxylic acid (TCH). The samples are decontaminated by the N-Acetyl L-Cysteine (NALC) method (WHO, 2009). Monthly, the RLM conducts an average of 100 bascilloscopies and 91 respiratory sample cultures, such as sputum, bronchoalveolar lavage, and endotracheal aspirates, as well as of extra-pulmonary samples, such as cerebrospinal fluid, urine, biopsies, among others.
To calculate the costs of the Detect TB® kit, only the respiratory samples were considered, following both the manufacturer’s recommendations (Labtest, 2012) and all of the conditions established by RLM/SM/FUMG and MBPH/SP/FUMG. The number of samples included in the calculation for the Detect TB® kit was only one per patient. All costs were expressed in U$, using an exchange rate of US$ 1 = R$ 2,34 in 2013 according Brazilian Central Bank.
Results
The Cost of Infrastructure
The results of the mean cost of the RLM/SM/FUMG infrastructure are shown in Table 1; these items did not influence the ABC of the verified methods. It can be observed that security is the item that most influenced the mean cost.
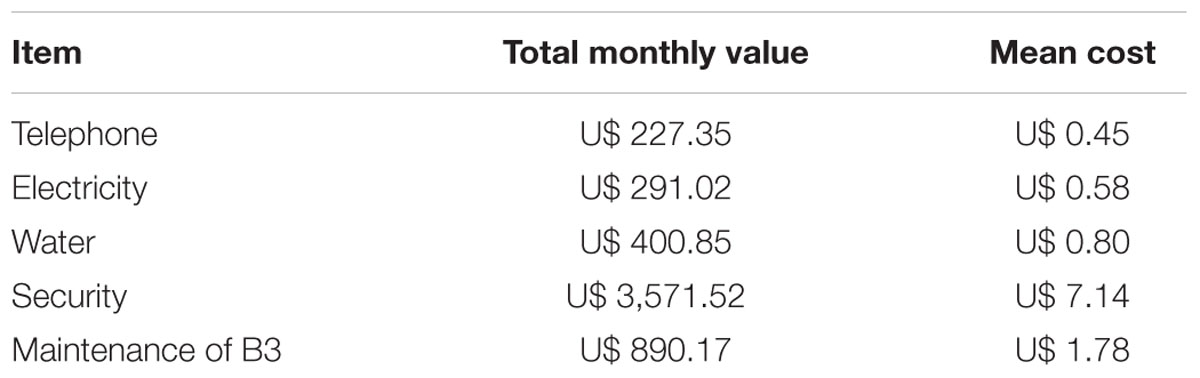
TABLE 1. Cost of Infrastructure of Research Laboratory in Mycobacteria and Molecular Biology and Public Health Laboratory, FUMG.
The Cost of Diagnostic Tests of Tuberculosis Laboratory Routine
The main items that influenced the mean costs and ABC of the bacilloscopy, culture, and Detect TB® kit are shown in Tables 2–4, where one can observe an individual difference in the mean cost of the equipment and a similarity of ABC for inputs. The unit value of the disposable apron observed in Tables 2 and 3 is higher than the other inputs, but did not affect the increase in mean cost and ABC. The mean cost and ABC of the assessed technologies are shown in Table 4; the cost components of each exam are listed in Table 5. The Detect TB® kit presented the highest cost, followed by the culture and the centrifuged and direct bacilloscopies. Among the cost components, in all of the assessed methods, the inputs were what most influenced the increase in the final value of each test followed by human resources, equipment and permanent materials (Table 6).
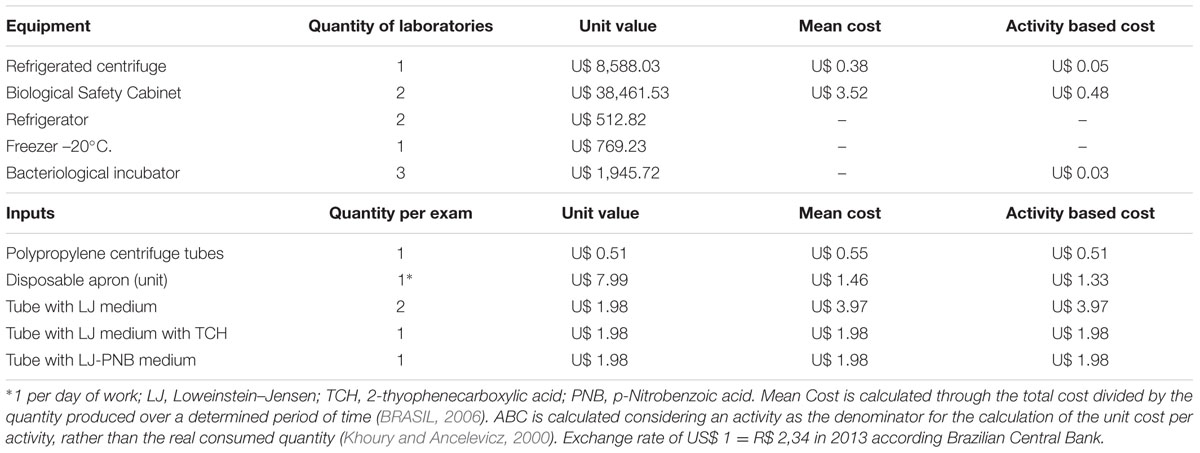
TABLE 2. Solid culture on Loweinsten–Jensen – main cost elements
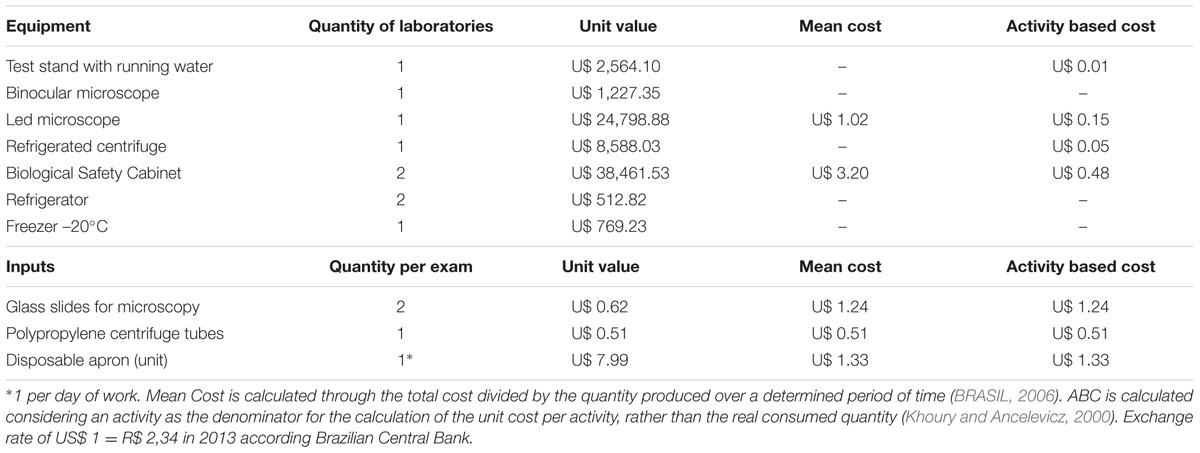
TABLE 3. Cost of the main equipment and inputs for bacilloscopy.
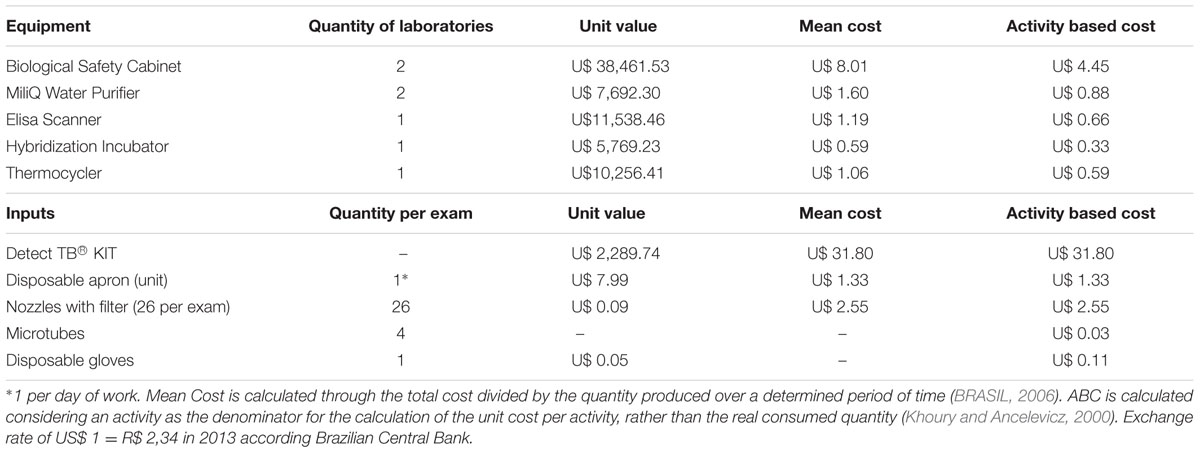
TABLE 4. Main laboratory issued with impact on Detect TB® test costs.
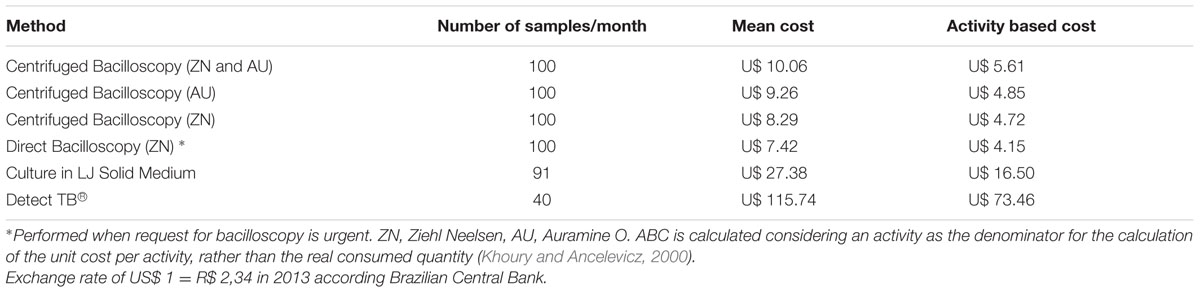
TABLE 5. Mean and activity based cost from the Research Laboratory in Mycobacteria and Molecular Biology and Public Health Laboratory, FUMG.
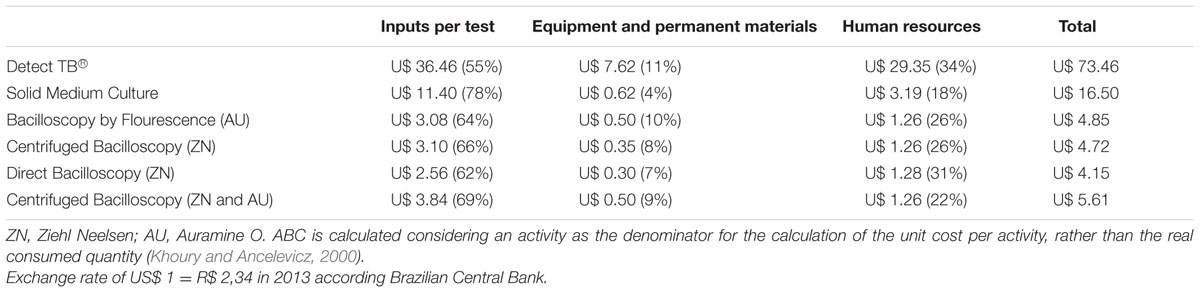
TABLE 6. Cost components of activity based cost for each diagnostic test.
Discussion
The mean cost was higher than the ABC in the diagnosis of pulmonary tuberculosis in the laboratory routine of a High-Complexity Hospital in Brazil. The results of the mean cost and ABC found in this study were of utmost importance for the re-structuring of laboratory activities, since, faced with these results, the routine of performing one slide stained with ZN and one with AU in centrifuged bacilloscopy was changed to only one slide stained with AU.
The impact that this result caused in the laboratory’s routine showed the substantial advantage of having used the ABC as the methodology, as well as the importance of conducting cost studies based on data that has been duly computed and not merely estimated based on other studies or the price of the Unique Health System in Brazil. These data can serve as a parameter for other public laboratories in Brazil that perform the same TB diagnostic methods, in addition to affirming that the correct count of the costs incurred in public services is an important instrument for social control and the assessment of the efficiency of services rendered (Martins, 2003).
The Detect TB® kit was the method that presented the highest costs. Nonetheless, it cannot be inferred whether or not the implementation of this would in fact be more costly, given that the sensitivity and specificity described by Michelon et al. (2011), showed from 75 to 100% and 98 to 100%, respectively, as compared to the bacilloscopy and culture, and presents the advantage of a shorter waiting time for the release of the result as compared to the culture. This fact reinforces the need for a cost study on the effectiveness of this test in low-prevalence locations, such as that carried out in the present work.
The values found for the Detect TB® kit are similar to other studies where molecular tests are assessed together with conventional techniques (Shah et al., 2013). The value of the Detect TB® kit (U$73.46) found in our study is less than the value of the Xpert MTB/RIF® molecular method (U$ 503.05, value of the cartridge) when not subsidized by the health system (BRASIL, 2013; FIND, 2013).
As regards, the bacilloscopy, it could be observed that there is no need to perform two methods of staining, since the costs are approximate and the AU technique is quick and sensitive, and does not expose the technicians to toxic vapors released when heating ZN (BRASIL, 2010). Despite the lower cost of staining by ZN without centrifugation, this method is less sensitive than centrifugation (WHO, 2009). The values of bacilloscopy found in the present study differ from the values cited in a similar study carried out in South Africa, where the ABC of the bacilloscopy stained with AU presented the value of U$3.40 and with ZN of U$2.25. Nevertheless, the values from the present study are near those found in different scenarios in Brazil, where the ABC of both staining methods was U$4.86 and for the mean cost was U$ 6.05 (BRASIL, 2013; Shah et al., 2013). The costs of bacilloscopy in Thailand by ZN and AU were US$1.16 and US$1.03 respectively. In Zambia compared the values of the culture by means of different techniques in liquid and solid media found a variation between US$28 and $32. However, these studies did not evaluate the mean cost and ABC. (Sohn et al., 2009a,b).
In the case of the culture, costs identified in the present study (U$ 16.50) were similar to other studies carried out in Brazil and Africa, with a variation from U$ 12.35 to U$ 28.00 (Mueller et al., 2008; Chihota et al., 2010; BRASIL, 2013).
The results of the ABC of the bacilloscopy and culture found in this study and those reported in national literature (BRASIL, 2013) are higher than the Brazilian Unified Health System’s pay (U$ 1.79 for bacilloscopy and U$ 2.29 for cultures), which alerts to the fact that these values do not reflect the real cost. This divergence confirms the relevance of the assessment of ABC, as the horizontal view of this parameter made it possible to reach an analysis that was not restricted to profit. This view is based on the planning, performing, and aid in strategic decision-making, as well as in the changes in processes, the elimination of waste, and the drafting of estimates based on the executed activities, thus increasing the efficiency of public services (Martins, 2003; Alonso, 2009).
In some countries of Asia and America the health system is private or public–private. In this context, the cost studies are important to improve the ability of management and financing of TB control programs (WHO, 2016).
The limitation of this study, rely on the fact that the individual costs of the patients were not inferred, such as: transport, outcome, among others, which are important variables for future studies on cost effectiveness and the implementation of an algorithm in laboratory diagnoses and strategies for the TB control. In addition, this study was carried out with local data from an NB3 laboratory geared exclusively towards the diagnosis of TB and other mycobacteria from high-complexity hospitals and from Molecular Biology laboratories.
Conclusion
The calculation of the ABC should be used in making decisions by administrators to be the best method of assessing the costs of conventional techniques and molecular method for providing the real value of the tests. So, it is need to calculate the ABC, and not of the mean cost, in various scenarios before incorporating new technologies in health institutions.
Author Contributions
Design of study: IA and SdM. Development of Cost chain: MV and SA. Data analysis: IA, MV, and SA. Article writing: IA, VS, WdSC, LJdAF, and SdM. Article review: MV, SA, AK. Production of the article’s final version: IA, VS, LJdAF, WdSC, MV, SA, AK. Promotion of study financing: SdM and AK. All the authors read and approved the final manuscript.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We wish to thank the Minas Gerais Research Support Foundation (FAPEMIG) (Process number – APQ 03266-13/APQ 00094-12), the National Research Council (CNPq) (Process number – CNPq 310174/2017-7 446796/2014), Labtest, INCT (Process number – CNPq /INCT 573548/2008-0), the Post-Graduate Program in Tropical Medicine and Infectology from the FUMG School of Medicine, Pro Rectory Research/UFMG, and the Brazilian Tuberculosis Network (REDE TB).
References
Almeida, I. N., Aleixo, A. V., Carvalho, W. S., and Miranda, S. S. (2015). In-house PCR with DNA extracted directly from positive slides to confirm or exclude the diagnosis of tuberculosis: focus on biosafety. Rev. Argent. Microbiol. 47, 47–49. doi: 10.1016/j.ram.2014.12.002
BRASIL (2006). “Ministério da Saúde,” in Manual Técnico de Custos – Conceitos e Metodologias, eds E. Ricciardi-Souza, M. M. L. de Lucena Horst, and R. V. Teixeira de Freitas (Brasilia: Secretaria de Ciência, Tecnologia e Insumos Estratégicos).
BRASIL (2010). “Manual nacional de vigilância laboratorial da tuberculose e outras micobactérias,” in Secretaria de Vigilância em Saúde, ed. F. Camilo (Brasília: Ministério da Saúde).
BRASIL (2011). “Ministério da Saúde,” in Xpert MTB/RIF No Diagnóstico da Tuberculose Pulmonar, Vol. 16, eds C. A. Petramale, M. Regina de Oliveira, and F. T. Silva Elias (Brasília: BRATS), 1–13.
BRASIL (2013). Ministério da Saúde. Programa Nacional de Controle da Tuberculose. Relatório Técnico: Estudos Econômicos da Incorporação do Teste Molecular GeneXpert MTB/Rif Para o Diagnóstico de Tuberculose Pulmonar no Sistema Único de Saúde. Available at: http://www.fundacaoataulphodepaiva.com.br/2013/07/Relatoriotecnico_25042013.pdf
Chihota, V. N., Grant, A. D., Fielding, K., Ndibongo, B., ZylVan, A., Muirhead, D., et al. (2010). Liquid vs. solid culture for tuberculosis: performance and cost in a resource-constrained setting. Int. J. Tuberc. Lung Dis. 14, 1024–1031.
FIND (2013). Foundation for Innovative New Diagnostics. Negotiated Prices for Xpert MTB/RIF. Available at: http://www.finddiagnostics.org/
Gholoobi, A., Masoudi-Kazemabad, A., Meshkat, A., and Meshkat, Z. (2014). Comparison of culture and PCR methods for diagnosis of Mycobacterium tuberculosis in different clinical specimens. Jundishapur J. Microbiol. 7, 8939. doi: 10.5812/jjm.8939
Khoury, C. Y., and Ancelevicz, J. (2000). Controvérsias acerca do sistema de custos ABC. ERA 40, 56–62. doi: 10.1590/s0034-75902000000100007
Labtest (2012). Detect TB – Instruções de Uso. Copyright by Labtest Diagnóstica S.A. Ref. 010713. Lagoa Santa: Labtest Diagnóstica S.A.
Michelon, C. T., Rosso, F., Schmid, K. B., Sperhacke, R. D., Oliveira, M. M., Kritski, A. L., et al. (2011). Colorimetric microwell plate reverse-hybridization assay for Mycobacterium tuberculosis detection. Mem. Inst. Oswaldo Cruz 106, 194–199. doi: 10.1590/S0074-02762011000200013
Mueller, D. H., Mwenge, L., Muyoyeta, M., Muvwimi, M. W., Tembwe, R., McNerney, R., et al. (2008). Costs and cost-effectiveness of tuberculosis cultures using solid and liquid media in a developing country. Int. J. Tuberc. Lung Dis. 12, 1196–1202.
Pinto, M., Entringer, A. P., Steffen, R., and Trajman, A. (2015). Análise de custos de um teste de amplificação de ácido nucléico para o diagnostico da tuberculose pulmonar sob a perspectiva do Sistema Único de Saúde. J. Bras. Pneumol. 41, 1–3.
Schimd, K. B., Scherer, L., Barcellos, R. B., Kuhleis, D., Prestes, I. V., Steffen, R. E., et al. (2014). Smear plus detect TB for a sensitive diagnosis of pulmonary tuberculosis: a cost-effectiveness analysis in a incarcerated population. BMC Infect. Dis. 14:678. doi: 10.1186/s12879-014-0678-x
Shah, M., Chihota, V., Coetzee, G., Churchyard, G., and Dorman, E. S. (2013). Comparison of laboratory costs of rapid molecular tests and conventional diagnostics for detection of tuberculosis and drug-resistant tuberculosis in South Africa. BMC Infect. Dis. 13:352. doi: 10.1186/1471-2334-13-352
Silva, L. K. (2003). Avaliação tecnológica e análise custo-efetividade em saúde: a incorporação de tecnologias e a produção de diretrizes clínicas para o SUS. Cien. Saude. Colet. 8, 501–520. doi: 10.1590/S1413-81232003000200014
Sohn, H., Minion, J., Albert, H., Dheda, K., and Pai, M. (2009a). TB diagnostic tests: how do we figure out their costs? Expert Rev. Ant. Infect. Ther. 7, 723–733. doi: 10.1586/eri.09.52
Sohn, H., Sinthuwattanawibool, C., Rienthong, S., and Varma, J. K. (2009b). Fluorescence microscopy is less expensive than Ziehl-Neelsen microscopy in Thailand. Int. J. Tuberc. Lung Dis. 13, 266–268.
Steingart, K. R., Schiller, I., Horne, D. J., Pai, M., Boehme, C. C., and Dendukuri, N. (2015). Xpert® MTB/RIF assay for pulmonary tuberculosis and rifampicin resistance in adults (Review). Cochrane Database Syst. Rev. 1, 1–131.
The International Journal of Tuberculosis, and Lung Disease [IJTLD] (2012). Editorial - Chest radiography for tuberculosis screening is back on the agenda. Int. J. Tuberc. Lung Dis. 16, 1421–1422. doi: 10.5588/ijtld.12.0774
WHO (2008). Policy Statement. Molecular Line Probe Assays for Rapid Screening of Patients at Risk of Multidrug-Resistant tuberculosis. Available at: http://www.who.int/tb/features_archive/policy_statement.pdf
WHO (2009). Approaches to Improve Sputum Smear Microscopy for Tuberculosis Diagnosis. Available at: http://www.who.int/tb/laboratory/egmreport_microscopymethods_nov09.pdf
WHO (2016). Global Tuberculosis Report. Available at: http://www.who.int/tb/publications/global_report.pdf
Keywords: tuberculosis, health system, cost analysis, mycobacteria, technology
Citation: de Almeida IN, de Assis Figueredo LJ, Soares VM, Vater MC, Alves S, da Silva Carvalho W, Kritski AL and de Miranda SS (2017) Evaluation of the Mean Cost and Activity Based Cost in the Diagnosis of Pulmonary Tuberculosis in the Laboratory Routine of a High-Complexity Hospital in Brazil. Front. Microbiol. 8:249. doi: 10.3389/fmicb.2017.00249
Received: 25 October 2016; Accepted: 06 February 2017;
Published: 15 February 2017.
Edited by:
Leonard Peruski, US Centers for Disease Control and Prevention, USAReviewed by:
Levent Dalar, Istanbul Bilim University, TurkeyCristina Vilaplana, Institut d’Investigació Germans Trias i Pujol, Spain
Javier Bezos, Complutense University of Madrid, Spain
Copyright © 2017 de Almeida, de Assis Figueredo, Soares, Vater, Alves, da Silva Carvalho, Kritski and de Miranda. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Silvana S. de Miranda, silvanaspindola@gmail.com