Soluble angiotensin-converting enzyme 2 association with lipid metabolism
 Izumi Nagatomo*
Izumi Nagatomo*  Kaori Nakanishi
Kaori Nakanishi  Ryohei Yamamoto
Ryohei Yamamoto  Seiko Ide
Seiko Ide  Chisaki Ishibashi Toshiki Moriyama Keiko Yamauchi-Takihara
Chisaki Ishibashi Toshiki Moriyama Keiko Yamauchi-Takihara- Health Care Division, Health and Counseling Center, Osaka University, Osaka, Japan
Increased expression of angiotensin-converting enzyme 2 (ACE2) is one of the likely explanations for disease severity in patients with coronavirus disease 2019 (COVID-19). In this study, we aimed to test whether soluble ACE2 (sACE2) levels are correlated to known risk factors of severe COVID-19 including biochemical parameters, body mass index and smoking habits. We cross-sectionally evaluated serum sACE2 levels in obese or tobacco-smoking populations and compared them to those in non-obese and non-smoking healthy participants. Additionally, fibroblast growth factor-21 (FGF21) was investigated as a candidate regulator of sACE2. A total of 220 male participants aged 30–59 years undergoing an annual health checkup were enrolled in this study: 59 obese, 80 smokers, and 81 healthy. Serum sACE2 levels were significantly higher in obese participants but not in tobacco-smoking participants when compared to healthy participants. sACE2 levels were significantly correlated with total cholesterol and triglycerides but not with body mass index. Furthermore, no regulatory relationship was found between FGF21 and sACE2. Lipid metabolism disorders accompanied by upregulation of serum sACE2 may be underlying mechanisms of COVID-19 aggravation and might be a novel breakthrough treatment target.
Introduction
The severity of coronavirus disease 2019 (COVID-19) depends on comorbidities; diabetes mellitus (1), hypertension (2), dyslipidemia (3), metabolic syndrome (4), obesity (5), age (6), male sex (7), and smoking habits (8) are known risk factors for aggravation of the disease. However, the causative relationships between comorbidities and disease severity remain unclear. Angiotensin-converting enzyme 2 (ACE2), which is expressed in various tissues, is an important regulator of the renin-angiotensin-aldosterone system and has attracted much attention as a receptor for the coronavirus (9–11). Increased ACE2 expression may be a potential cause of aggravation because it can lead to higher amounts of viral entry into target cells (12). Previous studies have shown a relationship between ACE2 expression levels and some comorbidities; for example, hyperglycemia increases monocyte surface ACE2 expression (13). Smoking has also been shown to upregulate ACE2 expression in the small airway epithelium and pneumocytes (14).
However, assessment of tissue ACE2 expression is technically difficult; therefore, soluble ACE2 (sACE2) in the serum has been evaluated as an alternative. Serum sACE2 has been reported to be upregulated in individuals with obesity and lifestyle-related diseases (15, 16). ACE2 and serum sACE2 expression are also known to be higher in men than in women (17). These findings suggest that higher ACE2 expression could explain the higher risk of severe COVID-19 in patients with these various backgrounds. However, it remains unclear how ACE2 expression is regulated in normal and diseased individuals.
Fibroblast growth factor-21 (FGF21) is a type of cytokine involved in metabolism and is also classified as a type of mitokine that is produced in response to mitochondrial stress (18). Serum levels of FGF21 are increased in individuals with obesity, type 2 diabetes, and metabolic syndromes (19, 20). We also previously reported that smoking increased the serum levels of FGF21 (21). Of note, FGF21 was reported to induce ACE2 expression in adipocytes and renal cells in mouse models (22), which led to our hypothesis that FGF21 upregulation might cause aggravation of COVID-19 via induction of ACE2 in various lifestyle-related diseases. In the present study, we aimed to test this hypothesis by performing a series of cross-sectional examinations focusing on serum sACE2 and FGF21 levels.
Methods
Study participants
This study contains cross-sectional data obtained from employees of Osaka University. The participants were selected from male examinees aged 30–59 years undergoing an annual health checkup at the Osaka University Health and Counseling Center. Patients with chronic illness or taking regular medication for at least 1 year before their health checkup were excluded in advance.
Participants were enrolled with a goal of roughly 300 cases, including obese, smoking, and healthy groups. For the obese group, examinees with a body mass index (BMI) of 30 or higher were selected, and current smokers were excluded from the obese group to avoid complexity. For the smoking group, currently smoking examinees were selected from those with a Brinkman Index of 100 or higher. As a result, there were no current smokers in the obese group, and none in the smoking group met the obesity criteria. As normal participants, healthy examinees were randomly selected who met the following conditions: blood pressure (BP) less than 140/90 mmHg, BMI 18.5–25 kg/m2, hemoglobin A1c (HbA1c) less than 5.6%, and non-smokers.
This study was performed in accordance with the Declaration of Helsinki and the Ethics Guidelines for Clinical Research from the Ministry of Health, Labor and Welfare, and the Ministry of Education, Culture, Sports, Science and Technology. All experimental protocols in this study were approved by the Ethics Committee of Health and Counseling Center, Osaka University, and written informed consent was obtained from all participants prior to participation in the study.
Assessments of physical and biochemical parameters
Body mass index and systolic and diastolic BP were measured as physical parameters. Information on participants’ medical history, current treatments, smoking status, and lifestyle behavior was obtained via questionnaires, which was reconfirmed through expert interviews by trained nurses.
Serum samples were collected from participants in the morning after an overnight fast and kept at ≤−20°C until assayed. Serum concentrations of aspartate aminotransferase (AST), alanine aminotransferase (ALT), gamma-glutamyl transpeptidase (γ-GTP), creatinine (Cr), uric acid (UA), total cholesterol (TCHO), triglyceride (TGL), high-density lipoprotein cholesterol (HDL), low-density lipoprotein cholesterol (LDL), glucose (Glu), and HbA1c were measured as part of an annual health checkup. For this study, serum levels of sACE2 and FGF21 were measured using the surplus of the same serum samples as described above. Serum concentrations of FGF21 were measured using a sandwich enzyme-linked immunoassay system according to the manufacturer’s instructions (R&D Systems Inc., Minneapolis, MN, United States). Serum concentrations of sACE2 were also measured using a sandwich enzyme-linked immunoassay system according to the manufacturer’s instructions (BioVision, Milpitas, CA, United States).
Statistical analyses
All statistical analyses were performed using STATA 16 (STATA Corp LLC, College Station, TX, United States). The distribution of continuous variables was tested using the Shapiro–Wilk test. Normally distributed variables are presented as means ± SD; non-normally distributed variables are presented as medians with interquartile ranges. The ANOVA followed by Tukey-Kramer pairwise comparison, or the Kruskal–Wallis equality-of-populations rank test, followed by Dunn’s pairwise comparison, was used to test differences between the three groups. The Spearman’s rank correlation coefficient was used to analyze the variables. All p-values were two-sided, and a p-value < 0.05 was considered statistically significant.
Results
Age dependency of serum soluble angiotensin-converting enzyme 2 levels
There were several cases in which the surplus samples were insufficient and could not be measured. An additional 16 participants were excluded because serum sACE2 or FGF21 were out of the measurable range and no precise data were available. As a result, a total of 220 men were enrolled in this study: 59 obese, 80 smokers, and 81 healthy.
First, all study participants were divided into three groups according to age, as follows: 30–39, 40–49, and 50–59 years (Table 1). Serum sACE2 levels showed no significant differences with age. On the other hand, FGF21 levels significantly increased with age, consistent with our previous reports (23). BMI was significantly lower in the 30–39 age group.
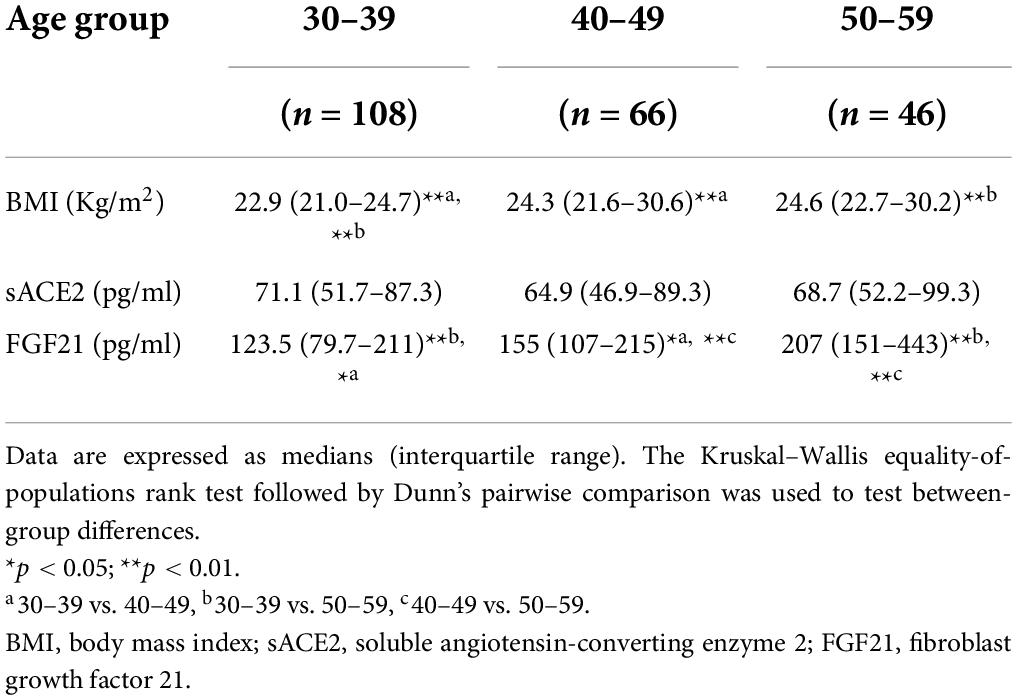
Table 1. Characteristics by age group.
Soluble angiotensin-converting enzyme 2 levels in obese and smoking groups
Next, we investigated whether serum sACE2 levels were altered in the obese and smoking groups compared to the normal group. Serum sACE2 levels were significantly increased in the obese group compared to those in the normal group (Figure 1A). On the other hand, serum sACE2 levels were not significantly different between the smoking and normal groups (Figure 1A). The median serum sACE2 levels were 59.8, 81.6, and 70.9 pg/ml in the normal, obese, and smoking groups, respectively. As shown in Figure 1B, data distribution displayed the difference between obese and other groups, suggesting the upregulation of serum sACE2 in obesity.
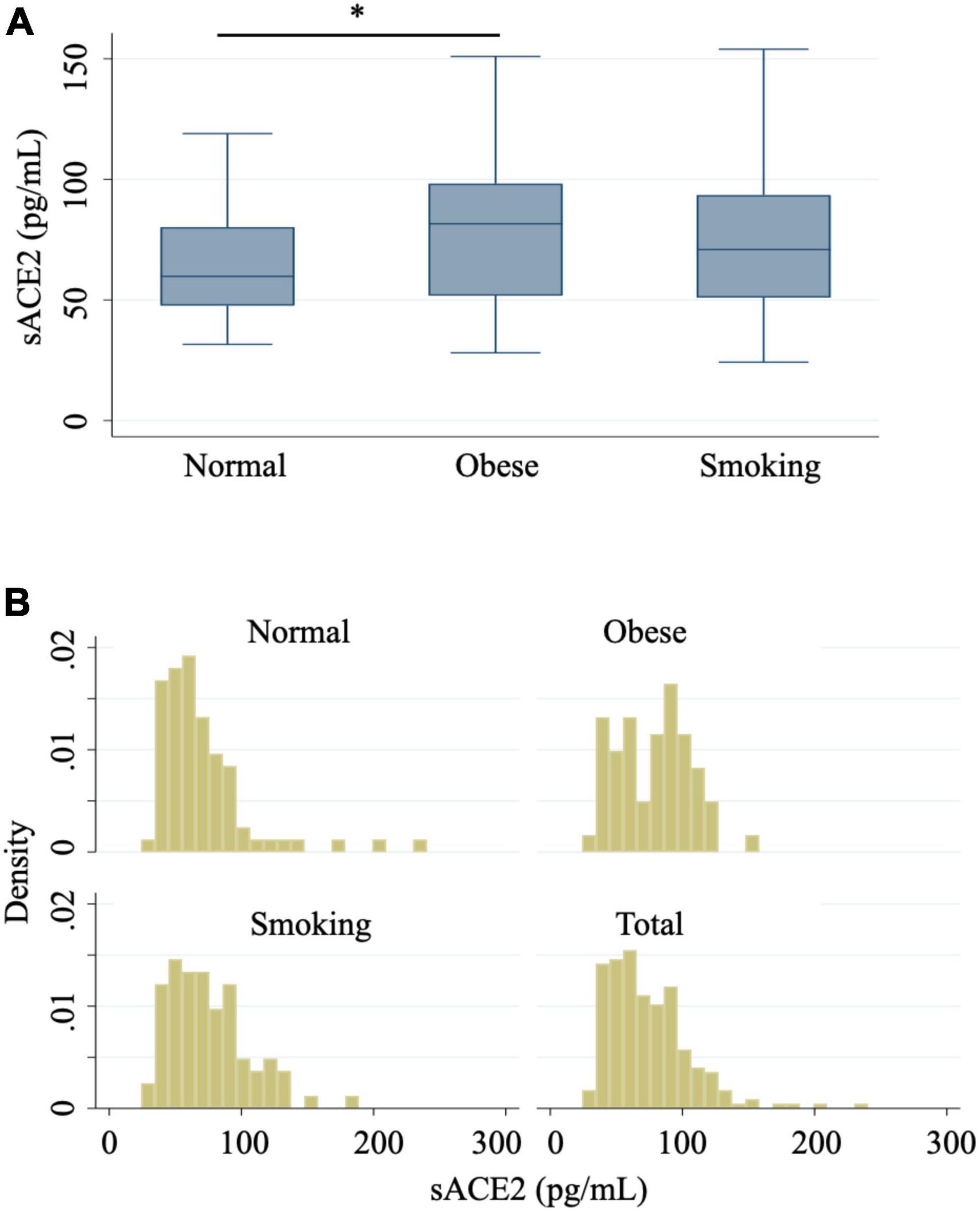
Figure 1. Serum sACE2 levels in normal, obese, and smoking groups. (A) Box plots show serum sACE2 levels from normal, obese, and smoking groups. The Kruskal–Wallis equality-of-populations rank test, followed by Dunn’s pairwise comparison, was used to test between-group differences. *p < 0.05. (B) Histograms provide a visual representation of data distribution in serum sACE2 levels from normal, obese, smoking, and total groups.
Association of soluble angiotensin-converting enzyme 2 levels with metabolic parameters
To further elucidate the role of serum sACE2 in obesity and related systemic metabolic disorders, various parameters, including FGF21, were analyzed. The characteristics of the three groups (normal, obese, and smoking) are shown in Table 2. As expected, TCHO and TGL were significantly higher in the obese and smoking groups compared to the normal group (Table 2). Differences between the obese and smoking groups depended on the parameters.
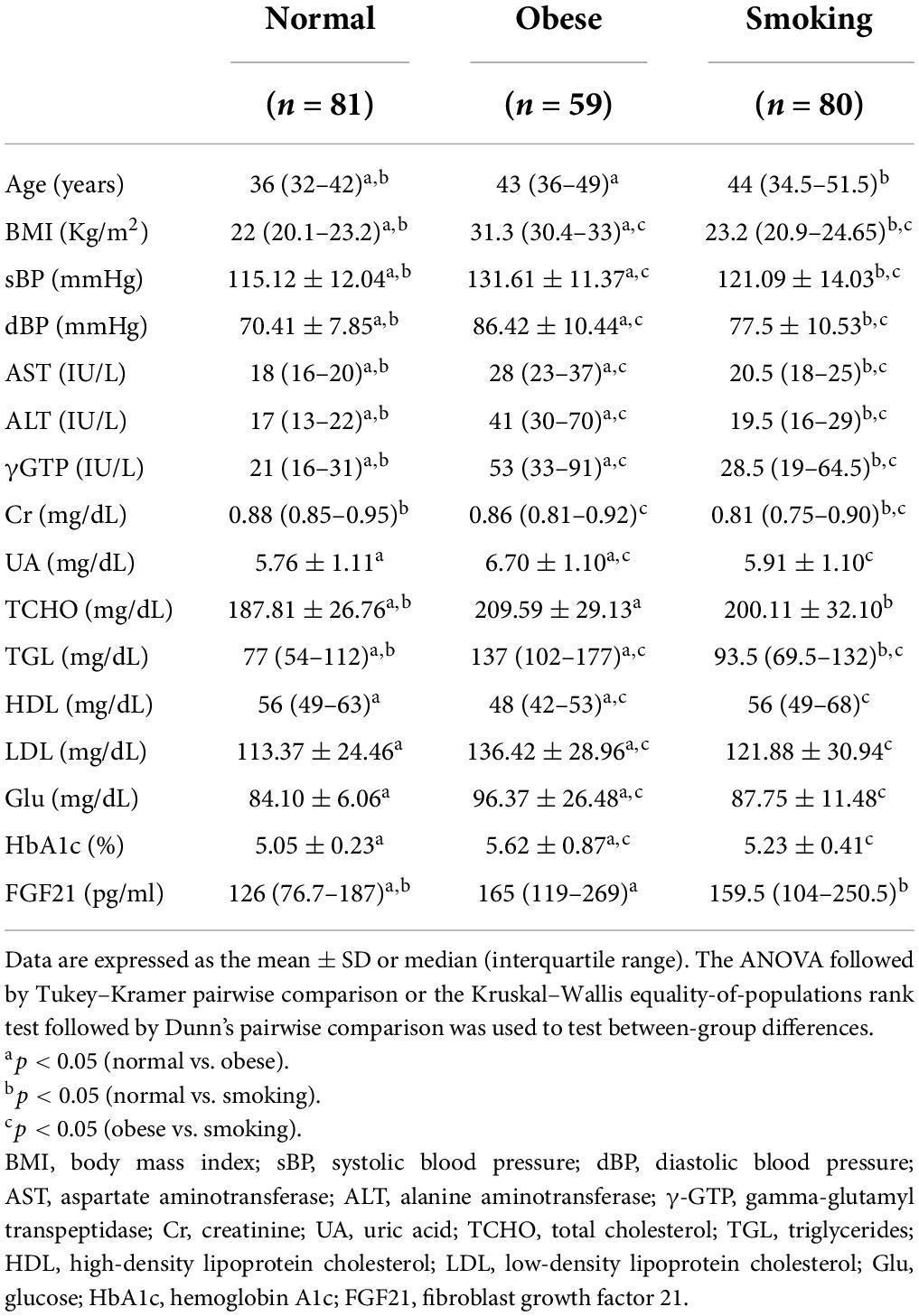
Table 2. Comparison of characteristics between normal, obese, and smoking groups.
Next, we assessed the relationship between serum sACE2 levels and some of the above parameters, confirming that serum sACE2 levels correlated with lipid parameters, TCHO and TGL, but not with Glu (Table 3). However, BMI itself was not significantly correlated with serum sACE2 levels (Table 3). Also, FGF21 did not correlate with serum sACE2 levels (Table 3), suggesting that other mechanisms regulate serum sACE2 levels in these participants. Taken together, serum sACE2 levels certainly increased in obese participants and were more closely correlated to hyperlipidemia than BMI itself in the combined normal, obese and smoking participants.
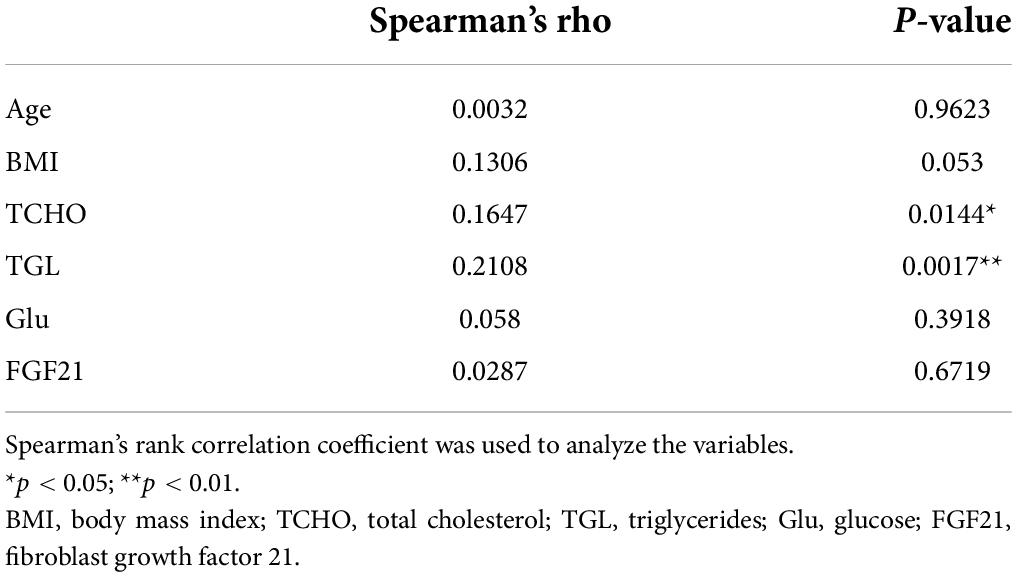
Table 3. Correlation of sACE2 and other factors in all the participants.
Discussion
This study was conducted under the hypothesis that ACE2 expression levels might contribute to COVID-19 aggravation in relation to viral load. We attempted to test this hypothesis by measuring sACE2 at ordinary condition in high-risk populations. We evaluated serum sACE2 levels in obese or smoking individuals and analyzed their relationship with biochemical parameters including FGF21. We found that serum sACE2 levels were significantly elevated in the obese population compared to those in the healthy population. Serum sACE2 levels significantly correlated with TCHO and TGL in all the populations. No correlation was found with FGF21 in any population.
In a previous study, ACE2 expression was found to be upregulated in lung alveolar epithelial cells and adipose tissue in obese or smoking participants (24). These are the target organs of COVID-19, and it is possible that increased expression of ACE2 in these tissues results in increased viral load, contributing to the aggravation of the disease. On the other hand, cytokine storms have been identified as the central pathological mechanism of COVID-19 aggravation (25, 26). In addition, thrombotic tendency is a characteristic of the pathological condition, which is also involved in disease severity (27).
Dyslipidemia is a risk factor for severe COVID-19, probably due to a thrombotic tendency or underlying chronic mild inflammation, which is compatible with our hypothesis in this study. We speculate that the relationship between serum sACE2 levels and lipid metabolism shown in this study also reinforces these findings directly or indirectly. However, the mechanism seems to be complex, and it is certainly not explained by a single factor, such as FGF21. A previous report describes temporal changes in sACE2 associated with metabolic parameters during a weight-loss diet intervention (28). In that study, sACE2 decreased during the intervention and was associated with improvements in metabolic health, including decrease in TGL. Taken together, lipid metabolism is suggested to be intrinsically interacted with sACE2 regulation.
Conflicting reports have been made on the involvement of sACE in the aggravation of COVID-19. We performed this study on the premise that high expression of ACE2 promotes aggravation from the viewpoint of viral load. Indeed, not only ACE2 but also sACE2 can function as a receptor for SARS-CoV-2 (29). However, from the viewpoint of an enzyme, the cardiovascular protective action of ACE2 has been reported to suppress the aggravation. We also assume that sACE2 levels reflect tissue ACE2 expression, but the activity of enzymes such as ADAM17 critically regulates sACE2 levels (30). There are also reports that ACE-I and ARB as antihypertensive drugs do not affect the severity of the disease, making the situation chaotic (31). In addition, our result that sACE2 does not increase in smokers is different from a previous report (15). This difference may be the result of differences in patient background and differences in smoking index standards.
This study has some limitations that should be interpreted with caution. First, from a statistical point of view, the sample size may be insufficient to verify the relationship between some parameters. Second, due to the age bias across all participants, background factors and the obtained data might be biased. Finally, serum sACE2 levels are not necessarily proportional to the ACE2 expression levels in tissues or organs. Despite these restrictions, our data indicate that high expression of ACE2 accompanied by dyslipidemia could be involved in the aggravation of COVID-19. Further investigation is required to fully clarify the significance of serum sACE2 levels in relation to COVID-19 aggravation risk in the obese population.
Data availability statement
The datasets generated and/or analyzed during this study are available from the corresponding author upon reasonable request.
Ethics statement
The studies involving human participants were reviewed and approved by Osaka University Health and Counseling Center Research Ethics Review Committee. Written informed consent was obtained from all participants prior to participation in this study.
Author contributions
IN, KN, and KY-T designed the study. IN performed the experiments, analyzed the data, and wrote the manuscript. CI, KN, and KY-T provided suggestions in the process of this study. SI, RY, and TM provided comments on the first draft. All authors have given approval to the final version of the manuscript.
Funding
This study was supported by a grant for research on lifestyle-related diseases to KY-T (J037701005).
Acknowledgments
The authors thank all the nurses and technicians who helped collect the data. The authors would like to express our appreciation to all study participants. The authors would also like to thank Editage (www.editage.com) for English language editing.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Buicu AL, Cernea S, Benedek I, Buicu CF, Benedek T. Systemic inflammation and COVID-19 mortality in patients with major noncommunicable diseases: chronic coronary syndromes, diabetes and obesity. J Clin Med. (2021) 10:1545. doi: 10.3390/jcm10081545
2. Shibata S, Arima H, Asayama K, Hoshide S, Ichihara A, Ishimitsu T, et al. Hypertension and related diseases in the era of COVID-19: a report from the Japanese society of hypertension task force on COVID-19. Hypertens Res. (2020) 43:1028–46. doi: 10.1038/s41440-020-0515-0
3. Matsunaga N, Hayakawa K, Terada M, Ohtsu H, Asai Y, Tsuzuki S, et al. Clinical epidemiology of hospitalized patients with coronavirus disease 2019 (COVID-19) in Japan: report of the COVID-19 registry Japan. Clin Infect Dis. (2021) 73:e3677–89. doi: 10.1093/cid/ciaa1470
4. Novaes Matias J, Sorrentino Dos Santos Campanari G, Achete de Souza G, Marinho Lima V, José Tofano R, Rucco Penteado Detregiachi C, et al. Metabolic syndrome and COVID-19. AIMS Bioeng. (2020) 7:242–53. doi: 10.3934/bioeng.2020021
5. Ritter A, Kreis NN, Louwen F, Yuan J. Obesity and COVID-19: molecular mechanisms linking both pandemics. Int J Mol Sci. (2020) 21:5793. doi: 10.3390/ijms21165793
6. Channappanavar R, Perlman S. Age-related susceptibility to coronavirus infections: role of impaired and dysregulated host immunity. J Clin Invest. (2020) 130:6204–13. doi: 10.1172/JCI144115
7. Gebhard C, Regitz-Zagrosek V, Neuhauser HK, Morgan R, Klein SL. Impact of sex and gender on COVID-19 outcomes in Europe. Biol Sex Differ. (2020) 11:29. doi: 10.1186/s13293-020-00304-9
8. Zheng Z, Peng F, Xu B, Zhao J, Liu H, Peng J, et al. Risk factors of critical & mortal COVID-19 cases: a systematic literature review and meta-analysis. J Infect. (2020) 81:e16–25. doi: 10.1016/j.jinf.2020.04.021
9. Hikmet F, Méar L, Edvinsson Å, Micke P, Uhlén M, Lindskog C. The protein expression profile of ACE2 in human tissues. Mol Syst Biol. (2020) 16:e9610. doi: 10.15252/msb.20209610
10. Tikellis C, Thomas MC. Angiotensin-converting Enzyme 2 (ACE2) is a key modulator of the renin angiotensin system in health and disease. Int J Pept. (2012) 2012:256294. doi: 10.1155/2012/256294
11. Yamamoto K, Takeshita H, Rakugi H. ACE2, angiotensin 1–7 and skeletal muscle: review in the era of COVID-19. Clin Sci (Lond). (2020) 134:3047–62. doi: 10.1042/CS20200486
12. Stilhano RS, Costa AJ, Nishino MS, Shams S, Bartolomeo CS, Breithaupt-Faloppa AC, et al. SARS-CoV-2 and the possible connection to ERs, ACE2, and RAGE: focus on susceptibility factors. FASEB J. (2020) 34:14103–19. doi: 10.1096/fj.202001394RR
13. Codo AC, Davanzo GG, Monteiro LDB, de Souza GF, Muraro SP, Virgilio-da-Silva JV, et al. Elevated glucose levels favor SARS-CoV-2 infection and monocyte response through a HIF-1α/glycolysis-dependent axis. Cell Metab. (2020) 32:437.e–46.e. doi: 10.1016/j.cmet.2020.07.007
14. Brake SJ, Barnsley K, Lu W, McAlinden KD, Eapen MS, Sohal SS. Smoking upregulates angiotensin-converting Enzyme-2 receptor: a potential adhesion site for novel coronavirus SARS-CoV-2 (Covid-19). J Clin Med. (2020) 9:841. doi: 10.3390/jcm9030841
15. Emilsson V, Gudmundsson EF, Aspelund T, Jonsson BG, Gudjonsson A, Launer LJ, et al. Serum levels of ACE2 are higher in patients with obesity and diabetes. Obes Sci Pract. (2021) 7:239–43. doi: 10.1002/osp4.472
16. Kornilov SA, Lucas I, Jade K, Dai CL, Lovejoy JC, Magis AT. Plasma levels of soluble ACE2 are associated with sex, metabolic syndrome, and its biomarkers in a large cohort, pointing to a possible mechanism for increased severity in COVID-19. Crit Care. (2020) 24:452. doi: 10.1186/s13054-020-03141-9
17. Patel SK, Velkoska E, Burrell LM. Emerging markers in cardiovascular disease: where does angiotensin-converting enzyme 2 fit in? Clin Exp Pharmacol Physiol. (2013) 40:551–9. doi: 10.1111/1440-1681.12069
18. Fisher FM, Maratos-Flier E. Understanding the physiology of FGF21. Annu Rev Physiol. (2016) 78:223–41. doi: 10.1146/annurev-physiol-021115-105339
19. Cheng X, Zhu B, Jiang F, Fan H. Serum FGF-21 levels in Type 2 diabetic patients. Endocr Res. (2011) 36:142–8. doi: 10.3109/07435800.2011.558550
20. Zhang X, Yeung DCY, Karpisek M, Stejskal D, Zhou ZG, Liu F, et al. Serum FGF21 levels are increased in obesity and are independently associated with the metabolic syndrome in humans. Diabetes. (2008) 57:1246–53. doi: 10.2337/db07-1476
21. Nakanishi K, Nishida M, Harada M, Ohama T, Kawada N, Murakami M, et al. Klotho-related molecules upregulated by smoking habit in apparently healthy men: a cross-sectional study. Sci Rep. (2015) 5:14230. doi: 10.1038/srep14230
22. Pan X, Shao Y, Wu F, Wang Y, Xiong R, Zheng J, et al. FGF21 prevents angiotensin II-induced hypertension and vascular dysfunction by activation of ACE2/angiotensin-(1–7) axis in mice. Cell Metab. (2018) 27:1323–37.e5. doi: 10.1016/j.cmet.2018.04.002
23. Nakanishi K, Ishibashi C, Ide S, Yamamoto R, Nishida M, Nagatomo I, et al. Serum FGF21 levels are altered by various factors including lifestyle behaviors in male subjects. Sci Rep. (2021) 11:22632. doi: 10.1038/s41598-021-02075-8
24. Engin AB, Engin ED, Engin A. Two important controversial risk factors in SARS-CoV-2 infection: obesity and smoking. Environ Toxicol Pharmacol. (2020) 78:103411. doi: 10.1016/j.etap.2020.103411
25. del Valle DM, Kim-Schulze S, Huang HH, Beckmann ND, Nirenberg S, Wang B, et al. An inflammatory cytokine signature predicts COVID-19 severity and survival. Nat Med. (2020) 26:1636–43. doi: 10.1038/s41591-020-1051-9
26. Hirano T, Murakami M. COVID-19: a new virus, but a familiar receptor and cytokine release syndrome. Immunity. (2020) 52:731–3. doi: 10.1016/j.immuni.2020.04.003
27. Rodríguez C, Luque N, Blanco I, Sebastian L, Barberà JA, Peinado VI, et al. Pulmonary endothelial dysfunction and thrombotic complications in patients with COVID-19. Am J Respir Cell Mol Biol. (2021) 64:407–15. doi: 10.1165/rcmb.2020-0359PS
28. Cauwenberghs N, Prunicki M, Sabovèik F, Perelman D, Contrepois K, Li X, et al. Temporal changes in soluble angiotensin-converting enzyme 2 associated with metabolic health, body composition, and proteome dynamics during a weight loss diet intervention: a randomized trial with implications for the COVID-19 pandemic. Am J Clin Nutr. (2021) 114:1655–65. doi: 10.1093/ajcn/nqab243
29. Yeung ML, Teng JLL, Jia L, Zhang C, Huang C, Cai J-P, et al. Soluble ACE2-mediated cell entry of SARS-CoV-2 via interaction with proteins related to the renin-angiotensin system. Cell. (2021) 184:2212–28. doi: 10.1016/j.cell.2021.02.053
30. Wang J, Zhao H, An Y. ACE2 shedding and the role in COVID-19. Front Cell Infect Microbiol. (2022) 11:789180. doi: 10.3389/fcimb.2021.789180
Keywords: sACE2, obesity, total cholesterol, triglycerides, COVID-19
Citation: Nagatomo I, Nakanishi K, Yamamoto R, Ide S, Ishibashi C, Moriyama T and Yamauchi-Takihara K (2022) Soluble angiotensin-converting enzyme 2 association with lipid metabolism. Front. Med. 9:955928. doi: 10.3389/fmed.2022.955928
Received: 29 May 2022; Accepted: 25 July 2022;
Published: 10 August 2022.
Edited by:
Sara Manti, University of Catania, ItalyReviewed by:
Vanessa Marthe Monteil, Karolinska Institutet (KI), SwedenŠtefan Zorad, Slovak Academy of Sciences (SAS), Slovakia
Copyright © 2022 Nagatomo, Nakanishi, Yamamoto, Ide, Ishibashi, Moriyama and Yamauchi-Takihara. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Izumi Nagatomo, iznagatomo@hacc.osaka-u.ac.jp