Multicomponent, high-intensity, and patient-centered care intervention for complex patients in transitional care: SPICA program
 Miguel García-Hernández1,2†
Miguel García-Hernández1,2†  Beatriz González de León1,2†
Beatriz González de León1,2†  Silvia Barreto-Cruz1,2
Silvia Barreto-Cruz1,2  José Ramón Vázquez-Díaz1,2*
José Ramón Vázquez-Díaz1,2*- 1Unidad Docente de Atención Familiar y Comunitaria La Laguna-Tenerife Norte, Gerencia de Atención Primaria del Área de Salud de Tenerife, Santa Cruz de Tenerife, Spain
- 2Network for Research on Chronicity, Primary Care, and Health Promotion (RICAPPS), Tenerife, Spain
Multimorbidity is increasingly present in our environment. Besides, this is accompanied by a deterioration of social and environmental conditions and affects the self-care ability and access to health resources, worsening health outcomes and determining a greater complexity of care. Different multidisciplinary and multicomponent programs have been proposed for the care of complex patients around hospital discharge, and patient-centered coordination models may lead to better results than the traditional ones for this type of patient. However, programs with these characteristics have not been systematically implemented in our country, despite the positive results obtained. Hospital Universitario de Canarias cares for patients from the northern area of Tenerife and La Palma, Spain. In this hospital, a multicomponent and high-intensity care program is carried out by a multidisciplinary team (made up of family doctors and nurses together with social workers) with complex patients in the transition of care (SPICA program). The aim of this program is to guarantee social and family reintegration and improve the continuity of primary healthcare for discharged patients, following the patient-centered clinical method. Implementing multidisciplinary and high-intensity programs would improve clinical outcomes and would be cost-effective. This kind of program is directly related to the current clinical governance directions. In addition, as the SPICA program is integrated into a Family and Community Care Teaching Unit for the training of both specialist doctors and specialist nurses, it becomes a place where the specific methodology of those specialties can be carried out in transitional care. During these 22 years of implementation, its continuous quality management system has allowed it to generate an important learning curve and incorporate constant improvements in its work processes and procedures. Currently, research projects are planned to reevaluate the effectiveness of individualized care plans and the cost-effectiveness of the program.
Introduction
Chronic conditions and multimorbidity
Chronic diseases are becoming more frequent. They are considered to be responsible for 74% of the deaths in the world (1) and, according to the Global Burden of Disease and Injury in 2019, account for more than 80% of disability-adjusted life years in Europe (2). Moreover, analyses carried out in Spain have postulated that the use of primary care increases in people with chronic diseases (3–5).
Although there are many definitions, multimorbidity is mainly considered to be the presence of more than one chronic condition, which are clinical and non-clinical (6). The presence of multimorbidity is increasingly present worldwide (7). It has been observed in studies with Spanish patients that those who use primary care the most are multimorbid people (3, 4). This supposes significant challenges for health systems (8, 9). It has been considered to increase mortality, decrease quality of life (10, 11), and increase costs and negative consequences for patients (12, 13).
Associated with the concept of multimorbidity, we found the concept of complexity. The presence of several chronic diseases is added to the fact that there are social and environmental conditions that have an impact on self-care and access to resources (14). In other words, not only the number of simultaneous chronic diseases influences health but also the severity of them added to several psychosocial factors (15). Complexity could be understood as a dynamic state in which socioeconomic, cultural, environmental, behavioral, and biological aspects operate as factors that hinder the understanding and management of health in certain people (16). Consequently, the interrelation between different factors may lead to interactions of diagnostic procedures or interventions, different treatment strategies, and multiple healthcare (16). That is why we distinguished between the complexity of the case, which refers to overlapping diseases and symptoms, and the complexity of care, which refers to the provision of healthcare and the joint involvement of systems and specialties. A complex case does not necessarily need complex care and vice versa despite, in most cases, both appear. In addition, complexity in terms of healthcare utilization can be identified and may manifest as care-regimen complexity, healthcare system navigation challenges, or complex networks of healthcare providers (17). For that reason, we must take into account all types of complexity when approaching a patient. If we did not, medical care would not be efficient (18).
Complexity
Thus, complexity, the quality of self-care, and consequently health outcomes depend on the balance between the patient/relatives' capacity (skills, resources, or willingness to address the demands, including physical and psychological functioning, socioeconomic resources, social support, literacy, attitudes, and beliefs) and the workload of the demands (all the tasks and responsibilities that people face on a day-to-day basis) (19). Given this perspective, it is clear that the disease-centered care model cannot be applied to complex patients (20). The need to care for this kind of patient has led experts to seek a change in health systems with perspectives of systemic thinking and the search for common goals (21).
Care transition and transitional patient care
Among the different elements that increase patients' complexity, the care transition processes between levels of healthcare should be highlighted. Patients face several difficulties with healthcare system navigation, so the transition of care from home to the hospital and back to home after discharge has a great impact on patients. In the case of complex patients, there is a high susceptibility to suffering an interruption in the continuity of care (22, 23). This lack of continuity has not only been perceived by professionals but also by patients. Several experiences of patients in different countries point to the presence of coordination gaps between levels. Patients perceive that information is often not passed on during transitions from hospitals to community settings after discharge (24). In fact, deficits in communication and information transfer at hospital discharge are common and may adversely affect patient care, in terms of clinical outcomes, risk of readmission, and quality of care and costs (23, 25).
Likewise, some reasons could explain this discontinuation. First, the physical remoteness of family doctors hinders follow-up on patients admitted to the hospital. Although the new technological and information tools have improved the transmission of information between levels, they fail to replace the benefit of direct contact between professionals and patients. Regarding the organization, the care objectives of family doctors and hospital specialists may not be shared, which can cause coordination problems. Likewise, the patient-centered clinical methods of family doctors, a core value in family medicine (26, 27), contrast from those of hospital doctors, which are centered on the disease. That determines the difference between actions and decisions. Finally, complex patients, due to their inherent characteristics, have a lower capacity to face by their own means the necessary care that originates after hospital admission (28).
There are several strategies that have been carried out with the intention of overcoming this complexity and improving health outcomes, especially in transitional care. Some of these strategies demonstrate a reduction in hospital readmissions and the average stay (29–31). Among them, it has been observed that uniprofessional interventions do not show significant results on aspects such as hospital readmissions (32) and that it could be more appropriate to design multiprofessional and comprehensive care programs in which the patient is assessed and treated as a whole, and not just as the sum of its diagnostics (33, 34). Additionally, in the context of transitional care, high-intensity interventions have been defined as those long-term interventions committed to continuity of care, those which involve patient and caregivers, and those performed before, during, and after hospital discharge (35); and multicomponent interventions are those consisting of at least two simple components. It has been observed that high-intensity, multicomponent, and multidisciplinary interventions are likely to be effective in reducing readmission rates (33, 35, 36). Besides, mortality and quality of life improved with high-intensity and complexity (i.e., frequent contacts and more intervention components) of transitional care interventions (37).
In contrast, we cannot ignore the need for the patient to take an active part in this process. In this regard, we have the so-called patient-centered care (PCC) (38–40). Person-centered interventions during the care transition of complex patients have been identified by patients and relatives as facilitating factors of healthcare (41). So, patient involvement in care planning increases adherence to the care plan and improves the quality of life (42). This leads us to shared decision-making, which is a part of PCC. However, associated with the presence of great complexity of management, these patients find themselves in a stressful life situation, which makes the shared decision-making process especially complicated.
A multicomponent and high-intensity care program, using the PCC method, is carried out by a multidisciplinary team with complex patients in the transition of care, which is named as SPICA program. The main aim is to guarantee the continuity of care for hospitalized patients and improve their socio-family reintegration of them after hospital discharge.
Context (setting and population) in which the innovation occurs
SPICA is a technical name formed by the acronym for “Subprograma de Integración y Coordinación Asistencial” (care integration and coordination subprogram -or subprocess, too-), but “Spica” also is a Latin word which means both spike and tenon. As is well known, a spike is an inflorescence formed by a set of wheat grains that are arranged along an axis, which holds them together. Furthermore, a tenon is a piece widely used in carpentry to join two elements and makes an invisible junction. Therefore, the SPICA program can be considered metaphorically as that tenon that brings together all the elements to maintain the continuity of transitional care. Furthermore, it does it discreetly, without making these unifying elements too visible. SPICA program serves as a link between the patient, primary care, and the hospital providers to maintain continuity of care (43).
SPICA is identified as an integrated health service delivery in which the patient is the subject of the integration of different elements, which are needed to facilitate their care. From the point of view of integration typologies, SPICA incorporates the elements that have been described (system, organizational, functional, professional, service, and personal), with different degrees of intensity (44). In turn, it is a model that encompasses the individual integrated care that includes case management, individual care planning, and patient-centered medical home coordination. Being developed in the care transition, the program focuses on those hospitalized patients who present greater complexity, and therefore, greater difficulty and support needs to return home.
Its activity takes place at the Teaching Unit of Family and Community Care “La Laguna-Tenerife Norte” (45), which is located in Hospital Universitario de Canarias and attends to patients admitted to it, with a reference population of ~384,000 people, of which 338,000 are adults.
This program is currently made up of 5 teams, and each one is made up of a family doctor and a primary care nurse. It also has administrative support. It is coordinated by one of the team's family doctors. In turn, this coordinator reports to the director of this Teaching Unit.
The team has management by objectives and values, linked to incentives, with quantitative and qualitative components.
The base of patients of which SPICA works is around 22.000 hospital admissions (2021) in Hospital Universitario de Canarias (La Laguna), of which 16.300 constitute the actual target population for Spica (patients discharged from medical services or surgeries and more than 1 day of hospital stay).
Thus, from a quantitative point of view, the overall objective of this program is to include 900 patients per year with established quality standards (representing at least 5.5% of target patients). An efficiency of 85% is required from the teams, that is, out of these 900 patients, at least 792 (12%) must be discharged home (which represents at least 4.9% of hospital discharges). The qualitative objectives are related to the content and timing of the global care plan. This plan must be available before the first appointment with primary care professionals after discharge.
The program works with highly complex patients without specific age criteria or reason for admission if they meet the inclusion criteria established by the program itself (refer to Table 1). The inclusion criteria have been selected in relation to the characteristics of the patients that determine a complex hospitalization or a greater possibility of difficulties or barriers at discharge.
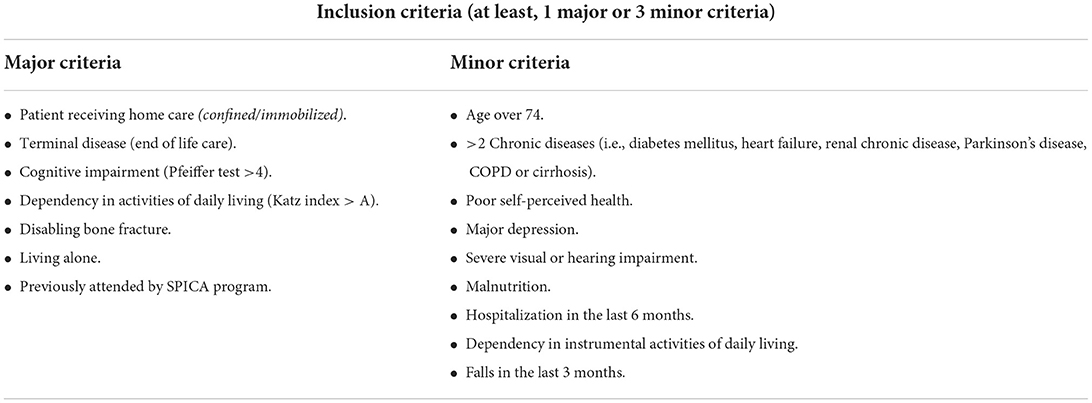
Table 1. Inclusion criteria for the SPICA program.
Patients access the program through the following two different ways:
(A) Hospital inpatient screening: The program considers the group of hospitalized patients as a population with risk components, especially in terms of continuity of care after discharge. For this reason, the screening process is carried out by the team's own professionals, who include the patients they consider to benefit most from their care (according to the criteria. Refer to Table 1).
(B) Opportunistic recruitment: It is carried out at the request of the service responsible for the hospital admission, primary care doctor, family, social workers, or the own patient.
As the SPICA program is part of the Canary Health Service, it will not be able to coordinate those patients who are referred from or to private health services. Likewise, when patients are discharged prematurely or the hospitalization time is too short (72 h), they cannot be coordinated. Finally, those patients who reject it or who are transferred to other hospitals are also excluded.
As mentioned earlier, although SPICA attends without age restriction, hospital inpatient screening among pediatric, obstetric, and psychiatric patients is not performed, and only opportunistic recruitment is conducted.
Detail to understand key programmatic elements
Since its design, the SPICA program incorporated and developed the core elements of the Chronic Care Model (46–49). SPICA professionals work in functional alliance with other medical specialists (both medical and surgical specialties), social workers and nurses specialized in other areas (depending on the case they attend), and family doctors and primary healthcare nurses. So, SPICA is a patient-centered program that incorporates comprehensive and contextual assessment, evidence-based clinical practice, and intra- and inter-level and inter-sectorial (with social services) coordination. In addition, the program purposes problem-solving through a multiprofessional and cooperative style.
As it has been said, this is a high-intensity and multicomponent program. So, it was ahead of its time, since it was not until a few years after its design that the efficacy of high-intensity and multicomponent interventions was confirmed (33, 35, 37).
Patient-centered comprehensive assessment
SPICA program intends to move away from transversality in care, and its main aim is to maintain continuity of care. When a patient is included in the program, and before the first assessment, SPICA professionals inquire on patients' history, their pathobiography, and context in which they live before admission. In this way, professionals seek a unique integrated understanding of each patient and acquire longitudinal knowledge of them. Deep knowledge of the previous state of the patient allows us to take the helm from primary care, continue it during hospitalization, and return it back to primary care after discharge.
After acquiring this prior information, the team performs its face-to-face evaluation of the patient. The patient assessment includes a comprehensive biopsychosocial evaluation (including patients, their family environment, and the available resources) (refer to Table 2 and more detailed information in Supplementary Appendix I) and is complementary and synergistic to the clinical evaluation carried out in the hospital. In this part, the objective is to know not only the patient's disease (medical history, physical examinations, and diagnostic tests) and experience of the disease but also their aspirations and their meaning. Specifically, illness experience exploration and the four key dimensions of it (feelings, ideas, functions, and expectations) (39, 40) are the essential activities of the SPICA program that is always performed. Besides, the program pursues understanding the social context in which the patients live their lives. Families and their life cycles and concerns are taken into account and displayed by structural and functional genogram, which is routinely performed on every patient. Thus, close contact is maintained with the patient's relatives, and family interventions are habitually conducted. This allows the professional to reach a proper meaning of the problems and attend to patients' perceptions of health and experience of the disease. In stressful circumstances such as hospital admission, changes occur in the elements; therefore, the understanding of the problems can change, and this leads to a permanent construction and reconstruction of the meaning. Bearing in mind this dynamic condition of construction and reconstruction of meanings is what allows us to formulate all the patient's problems before discharge. Therefore, the evaluation pursues an intentionality that is not merely contemplative but operational, with an aim at seeking keys to act and establish an adequate helping relationship (50).
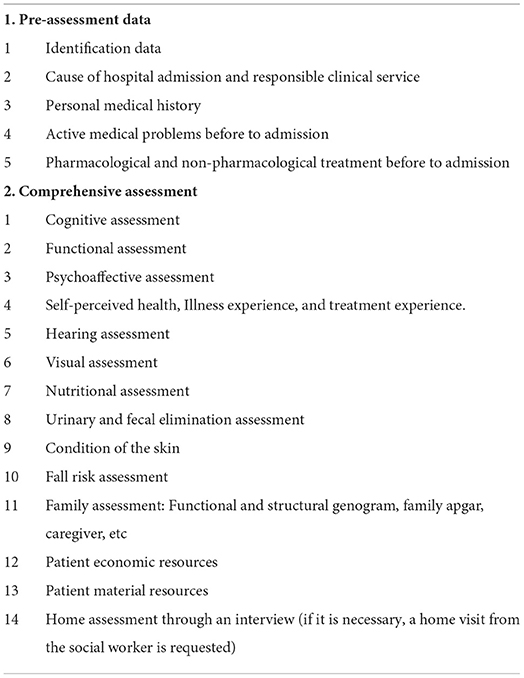
Table 2. SPICA program comprehensive assessment template.
Helping relationship: Patients, families, and professionals
During hospital admission, an increase in the complexity of future care is often derived, since the burdens of illness and care tend to raise and the ability to cope with it decreases (19). One of the challenges is to intervene to reduce these burdens of disease and/or care and increase the capacities and/or possibilities of patients to assume them. For that reason, the SPICA team has the role of carrying out horizontal coordination with all the professionals who care for the patient during hospitalization. Moreover, it also has the function of performing vertical coordination with primary care professionals, other professionals outside the hospital environment, the family/caregiver, the social network, and the patient.
As the SPICA program works with those patients who present not only the complexity of the case but also the complexity of care, in many cases, a large number of recommendations from different professionals are presented, which can be overlapping and contradictory. The program is responsible for coordinating these recommendations. At this time, the aim is to design an individualized care plan by establishing the goals and priorities of treatment and identifying the roles to be assumed by patients, caregivers, and professionals. To achieve this, the SPICA program searches for a common ground of understanding among professionals and the patient that allows the development of a care plan that matches the patient's preferences and is congruent with medical expertise and the best available evidence, but also feasible to apply in their environment.
In these special circumstances of the case and care complexity and taking into account that the patient is experiencing a stressful life event, shared decision-making is desirable but difficult. To reach a mutual decision, the SPICA team must gain the trust of the patient/caregiver. This trust is acquired when the patient, relative, and caregiver (depending on the case) have the perception that the professional has a deep understanding of the patient and by maintaining frequent contact during hospitalization. After exploring whether the patient and/or caregiver wants or can make decisions, the professional exposes the options. Once exposed, it is ensured that the patient and/or caregiver are able to understand them, and later, a decision will be made together. On occasions, it is advisable to have some time before making a decision. It should be noted that this plan is dynamic and interactive, and this is important for the patient to understand.
Transferring the care plan
During admission, continuous contact is maintained not only with the patient and their family/caregivers but also with their primary care providers, relaying a comprehensive report. At discharge, honoring that intention of maintaining continuity of care, the SPICA team is in charge of transmitting this information in the most detailed way possible, both to the professionals and to the patient/caregiver (refer to Figure 1 and Supplementary Appendix II). Moreover, the intervention seeks to improve the quality of life by enhancing the recovery of the patient's previous state of health and, if this is not possible, helping to accept and cope with the new health situation, promoting self-care training, empowering the patient, providing emotional support, and enhancing the patient-clinician relationship (refer to Figure 2).
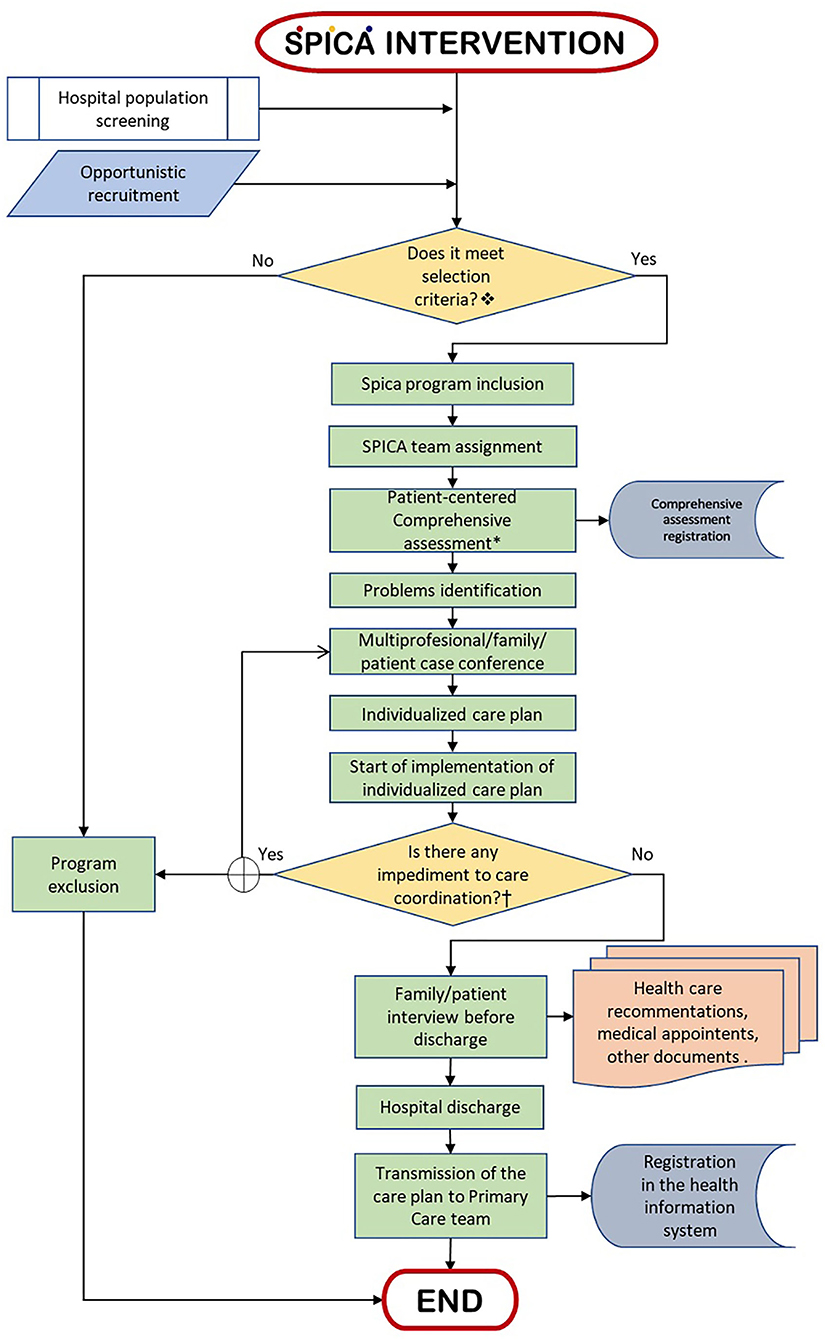
Figure 1. Flowchart (summarized) of the SPICA intervention process.  Inclusion criteria of the SPICA program are described in Table 1. *The sections that make up the SPICA comprehensive assessment are described in Supplementary Annex I.†Circumstances that do not allow the care coordination for patients included in SPICA program are: transfer of patients to other hospital or an intermediate care facility; death; or patient/family rejection.
Inclusion criteria of the SPICA program are described in Table 1. *The sections that make up the SPICA comprehensive assessment are described in Supplementary Annex I.†Circumstances that do not allow the care coordination for patients included in SPICA program are: transfer of patients to other hospital or an intermediate care facility; death; or patient/family rejection.

Figure 2. Main components of the Spica intervention.
Discussion section that shares practical implications and lessons learned for future applications
The fact that the SPICA program was proposed in 2000 in “La Laguna-Tenerife Norte” Multiprofessional Teaching Unit of Family and Community Care represents a singularity in the Spanish National Health Service. The team that makes up this Teaching Unit identifies itself with common professional values that try to make resident doctors and nurses visible during their training. That is what we call “values function deployment” (51). These values are Science, Humanity, Commitment, and Excellence. In this value-oriented training plan, it is created the conditions in which residents are exposed to the “daily experience of value,” as a necessary starting point for learning. The specialized training is based on supervised clinical practice and personal study, with the progressive assumption of responsibility, and is complemented by other types of regulated training activities. Regarding this commitment to training, the SPICA program is an ideal setting for learning fundamental values, knowledge, and abilities of the specialty of family and community care itself (refer to Figure 3). Every year, fifteen resident medical doctors in their third year of training and six resident nurses in their second year of training from this Teaching Unit are trained by working in this program. Each of them does it for 2 and 1.5 months, respectively (refer to Supplementary Appendices III, IV). In turn, this program receives resident nurses and doctors from other Teaching Units in Spain.
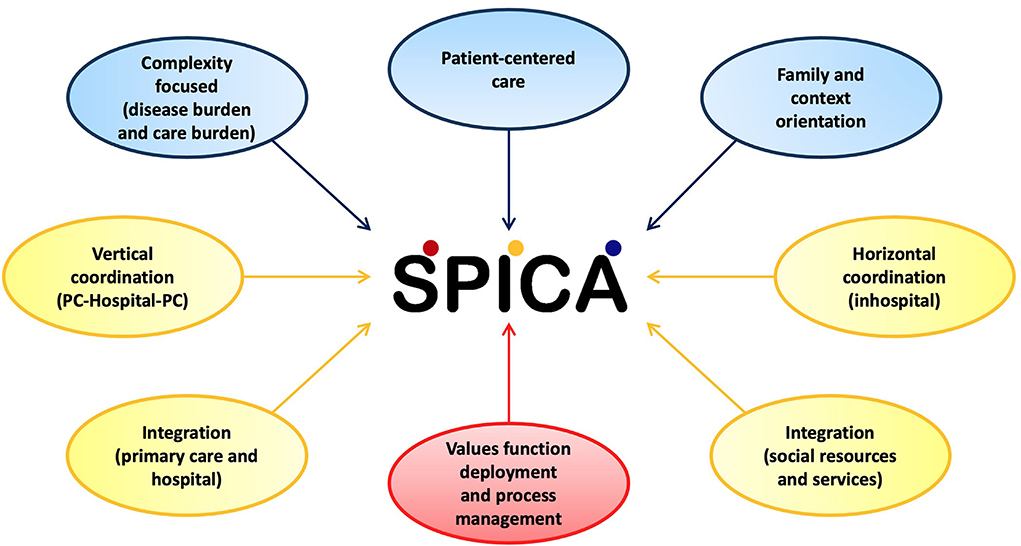
Figure 3. Major components of the Spica design (PC, primary care).
This program is committed to offering quality healthcare, which is why it pursues continuous quality management. Its first evaluation, at the end of 2000, showed positive effects in reducing hospital stays and readmissions. In later years, evaluations showed similar results and were presented at different national and regional congresses. Positive results have been observed in patient satisfaction. In addition, focus groups have been carried out to explore the perception of patients and caregivers, as well as primary care professionals, which has allowed us to know the utilities perceived by them and some improvement areas. The feedback from the different hospital services is collected through daily interaction and through the presentation of the annual results in joint sessions.
In 2006, a complete review of the program was carried out to adapt it to Process Management System and integrate it into the hospital and primary care management systems. Subsequently, in 2009, the program was reviewed again, to adapt to the ISO 9001 standard. The program was audited the same year, obtaining the certificate. Besides, in 2010, within the framework of management by processes, Hospital Universitario de Canarias defined the hospitalization and discharge process, and the SPICA program is embedded within it. In 2012 and 2013, improvements in interprofessional communication were incorporated. So, the SPICA program has been included in the hip fracture clinical pathway (since 2013) and the amyotrophic lateral sclerosis committee of Hospital Universitario de Canarias (since 2022). Although these improvements, the program's key components have remained stable since its formation in 2000.
Nowadays, the program is developing new research projects with the aim of reevaluating the effectiveness and cost-effectiveness of the program and its individualized care plans, focusing on the help relationship established with the patients. Thus, current interests also improve research on the creation and establishment of a common ground for understating meanings, problems, and/or conditions where shared decision-making occurs in vulnerable environments.
Acknowledgment of any conceptual or methodological constraints
Some of the limitations that SPICA faces derive from the characteristics of the context that make it necessary.
Organizational culture understood as the set of predominant values, attitudes, and behaviors that characterize the functioning of an organization (52), is crucial in a health system. The Spanish Health Care System is focused mainly on single diseases, and clinical guidelines usually take a single-morbidity approach (53). This ignores the complexity in caring for the increasing number of patients with multimorbidity. The fact that our health organization has been eminently sectorized by diseases or medical specialties makes it difficult to change the perspective of health professionals toward a more holistic, comprehensive, and cooperative approach (54). In 2012, a chronicity management strategy was attempted in our country. However, this strategy has not been properly implemented and has not received the necessary resources. So, it has not had the desired success (55). These reflect the need for a change in the organizational culture that enhances primary care and its role in coordinating the global care of patients, regardless of where they are.
Family medicine in Spain is going through an identity crisis (56, 57), and primary care has organizational problems that prevent it from exercising its leadership as the axis of the system. In our environment, there is no notification system for hospital admissions and hospital discharges, which notifies the primary care professional of what is happening. The clinical history recording system is organized by episodes, which facilitates the care of acute patients but makes it difficult to carry out the longitudinal follow-up of chronic patients. Furthermore, its design does not prioritize continuity, affecting all its components: informative, longitudinal, and interpersonal (58, 59). This will have implications from an organizational and clinical perspective (50).
The integration of services is consistent from the point of view of financing, organization, provision of services, and clinical practices, to improve care for complex people. The health sectorization, which we have already mentioned, prevents this integration. The SPICA program depends on primary care management but assumes responsibility for planning the hospital discharge of the most complex patients. Besides, this is made without an integration structure or hierarchy. The stability of this functionality over time is based on an agreement between managers (hospital and primary care ones) that assumes a win-win negotiation and on the team's ability to adequately manage the soft power that has been granted to it.
Difficulties in integration occur not only among clinical areas but also between health and social ones. Although the experiences in countries such as the USA (60) and England (61) have been promising, the truth is that in our country, there is still a sectorization between social and clinical services that greatly limit efficient system development. In the SPICA program, professionals work as a team with social workers, despite these barriers, offering the patient the possibility of integrating both spheres.
Since its creation, the SPICA program has covered the entire reference population of a tertiary care hospital on the island of Tenerife. His career and permanence in time speak in favor of its usefulness, in addition to all the aspects reported in this article. Thereby, the program can be considered a singularity among the Family and Community Care Teaching Units in Spain. “La Laguna–Tenerife Norte” Teaching Unit has direct clinical responsibilities, and in this sense, it has a great similarity with any other hospital services. That is not the usual framework in which the Family and Community Care Teaching Units are structured in our environment (Spanish Health System). In fact, SPICA depends financially and organically on Primary Care but attends to the patients within the hospital, is integrated into the hospital's process map, is also part of their discharge planning program, and supports various clinical pathways of the hospital itself. These disruptive elements with respect to the care and teaching model established in Spain, which are considered key elements of its success, can also become barriers to entry or elements of difficulty to encourage other managers and Teaching Units to follow the same path. During all these years, the team has invested all their energy in fully developing the program by implementing systems of management, evaluation, and quality improvement. So, a process of external communication, sharing experience with the scientific, professional, and management community, is currently started through this study and successes that are in the pipeline.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
MG-H and BG contributed to the conceptualization and writing and the editing. SB-C participated in the conceptualization and revision. JV-D participated in the conceptualization and writing and revision. All authors contributed to manuscript revision, read, and approved the submitted version.
Acknowledgments
The authors would like to thank Asunción López Hijazo, Félix Díez Salvador, and Concepción Rivera Pedraja for their help with the design and start of the SPICA program implementation. Besides, they would like to thank Yeiza Semiramis Reyes Melián and Vanesa Martínez Hernández for critically reviewing an earlier version of the manuscript. Finally, the authors would like to thank all the healthcare professionals who have made possible for the SPICA program being a useful reality and facilitating the care transition of the most complex patients over these 22 years.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2022.1033689/full#supplementary-material
References
1. Chigom E. Non-communicable Diseases Progress Monitor 2022. Geneva: World Health (2022). Available online at: https://www.who.int/es/publications/i/item/978924004776 (accessed August 31, 2022).
2. Vos T, Lim SS, Abbafati C, Abbas KM, Abbasi M, Abbasifard M, et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. (2020) 396:1204–22. doi: 10.1016/S0140-6736(20)30925-9
3. Barrio Cortes J, Suárez Fernández C, Bandeira de Oliveira M, Beca Martínez MT, Lozano Hernández C, Del Cura-González I. [Health services utilization in Primary Care in patients with chronic conditions according to risk levels]. Rev Esp Salud Publ. (2019) 93:1–15. doi: 10.1016/j.anpede.2019.12.006
4. Monterde D, Vela E, Clèries M, García Eroles L, Pérez Sust P. Validity of adjusted morbidity groups with respect to clinical risk groups in the field of primary care. Aten Primaria. (2019) 51:153–61. doi: 10.1016/j.aprim.2017.09.012
5. Millá Perseguer M, Guadalajara Olmeda N, Vivas Consuelo D. Impact of cardiovascular risk factors on the consumption of resources in primary care according to clinical risk groups. Aten Primaria. (2019) 51:218–29. doi: 10.1016/j.aprim.2017.11.008
6. Almirall J, Fortin M. The coexistence of terms to describe the presence of multiple concurrent diseases. J Comorbidity. (2013) 3:4–9. doi: 10.15256/joc.2013.3.22
7. Nguyen H, Manolova G, Daskalopoulou C, Vitoratou S, Prince M, Prina AM. Prevalence of multi-morbidity in community settings: a systematic review and meta-analysis of observational studies. J Comorbidity. (2019) 9:2235042X1987093. doi: 10.1177/2235042X19870934
8. Smith SM, Wallace E, Clyne B, Boland F, Fortin M. Interventions for improving outcomes in patients with multi-morbidity in primary care and community setting: a systematic review. Syst Rev. (2021) 10:1–23. doi: 10.1186/s13643-021-01817-z
9. Prados-Torres A, del Cura-González I, Prados-Torres JD, Leiva-Fernández F, López-Rodríguez JA, Calderón-Larrañaga A, et al. Multimorbilidad en medicina de familia y los principios Ariadne Un enfoque centrado en la persona. Atención Primaria. (2017) 49:300–7. doi: 10.1016/j.aprim.2016.11.013
10. Gijsen R, Hoeymans N, Schellevis FG, Ruwaard D, Satariano WA, van den Bos GAM. Causes and consequences of comorbidity. J Clin Epidemiol. (2001) 54:661–74. doi: 10.1016/S0895-4356(00)00363-2
11. Williams JS, Egede LE. The association between multi-morbidity and quality of life, health status and functional disability. Am J Med Sci. (2016) 352:45–52. doi: 10.1016/j.amjms.2016.03.004
12. Caballer Tarazona V, Guadalajara Olmeda N, Vivas Consuelo D, Clemente Collado A. [Impact of morbidity on health care costs of a department of health through clinical risk groups. Valencian community, Spain]. Rev Esp Salud Publica. (2016) 90:e1–15.
13. Picco L, Achilla E, Abdin E, Chong SA, Vaingankar JA, McCrone P, et al. Economic burden of multimorbidity among older adults: impact on healthcare and societal costs. BMC Health Serv Res. (2016) 16:1–12. doi: 10.1186/s12913-016-1421-7
14. Safford MM, Allison JJ, Kiefe CI. Patient complexity: more than comorbidity. The vector model of complexity. J Gen Intern Med. (2007) 22:382–90. doi: 10.1007/s11606-007-0307-0
15. Valderas JM, Starfield B, Sibbald B, Salisbury C, Roland M. Defining comorbidity: implications for understanding health and health services. Ann Fam Med. (2009) 7:357–63. doi: 10.1370/afm.983
16. Nicolaus S, Crelier B, Donzé JD, Aubert CE. Definition of patient complexity in adults: a narrative review. J Multimorb Comorbidity. (2022) 12:263355652210812. doi: 10.1177/26335565221081288
17. Schaink AK, Kuluski K, Lyons RF, Fortin M, Jadad AR, Upshur R, et al. A scoping review and thematic classification of patient complexity: offering a unifying framework. J Comorbidity. (2012) 2:1–9. doi: 10.15256/joc.2012.2.15
18. de Jonge P, Huyse FJ, Stiefel FC. Case and care complexity in the medically Ill. Med Clin North Am. (2006) 90:679–92. doi: 10.1016/j.mcna.2006.04.005
19. Shippee ND, Shah ND, May CR, Mair FS, Montori VM. Cumulative complexity: a functional, patient-centered model of patient complexity can improve research and practice. J Clin Epidemiol. (2012) 65:1041–51. doi: 10.1016/j.jclinepi.2012.05.005
21. Willis CD, Best A, Riley B, Herbert CP, Millar J, Howland D. Systems thinking for transformational change in health. Evid Policy A J Res Debate Pract. (2014) 10:113–26. doi: 10.1332/174426413X662815
22. Daliri S, Hugtenburg JG, Ter Riet G, van den Bemt BJF, Buurman BM, Scholte op Reimer WJM, et al. The effect of a pharmacy-led transitional care program on medication-related problems post-discharge: a before—after prospective study. PLoS ONE. (2019) 14:e0213593. doi: 10.1371/journal.pone.0213593
23. Kripalani S, LeFevre F, Phillips CO, Williams MV, Basaviah P, Baker DW. Deficits in communication and information transfer between hospital-based and primary care physicians. JAMA. (2007) 297:831. doi: 10.1001/jama.297.8.831
24. Schoen C, Osborn R, Squires D, Doty M, Pierson R, Applebaum S. New 2011 survey of patients with complex care needs in eleven countries finds that care is often poorly coordinated. Health Aff. (2011) 30:2437–48. doi: 10.1377/hlthaff.2011.0923
25. Nicolet A, Al-Gobari M, Perraudin C, Wagner J, Peytremann-Bridevaux I, Marti J. Association between continuity of care (COC), healthcare use and costs: what can we learn from claims data? A rapid review. BMC Health Serv Res. (2022) 22:1–30. doi: 10.1186/s12913-022-07953-z
26. McWhinney IR. Primary care: core values core values in a changing world. BMJ. (1998) 316:1807–9. doi: 10.1136/bmj.316.7147.1807
27. Michels NRM, Maagaard R, Švab I, Scherpbier N. Teaching and learning core values in general practice/family medicine: a narrative review. Front Med. (2021) 8:1–6. doi: 10.3389/fmed.2021.647223
28. Finlayson K, Chang AM, Courtney MD, Edwards HE, Parker AW, Hamilton K, et al. Transitional care interventions reduce unplanned hospital readmissions in high-risk older adults. BMC Health Serv Res. (2018) 18:956. doi: 10.1186/s12913-018-3771-9
29. Gonçalves-Bradley DC, Lannin NA, Clemson L, Cameron ID, Shepperd S. Discharge planning from hospital. Cochrane Database Syst Rev. (2022) 2022:CD000313. doi: 10.1002/14651858.CD000313.pub6
30. Leppin AL, Gionfriddo MR, Kessler M, Brito JP, Mair FS, Gallacher K, et al. Preventing 30-day hospital readmissions. JAMA Intern Med. (2014) 174:1095. doi: 10.1001/jamainternmed.2014.1608
31. Linertová R, García-Pérez L, Vázquez-Díaz JR, Lorenzo-Riera A, Sarría-Santamera A. Interventions to reduce hospital readmissions in the elderly: in-hospital or home care. A systematic review. J Eval Clin Pract. (2011) 17:1167–75. doi: 10.1111/j.1365-2753.2010.01493.x
32. Wong CH, Cheung WK, Zhong CC, Yeoh E, Hung CT, Yip BH, et al. Effectiveness of nurse-led peri-discharge interventions for reducing 30-day hospital readmissions: network meta-analysis. Int J Nurs Stud. (2021) 117:103904. doi: 10.1016/j.ijnurstu.2021.103904
33. Morkisch N, Upegui-Arango LD, Cardona MI, van den Heuvel D, Rimmele M, Sieber CC, et al. Components of the transitional care model (TCM) to reduce readmission in geriatric patients: a systematic review. BMC Geriatr. (2020) 20:345. doi: 10.1186/s12877-020-01747-w
34. Goodwin A, Henschen BL, O'Dwyer LC, Nichols N, O'Leary KJ. Interventions for frequently hospitalized patients and their effect on outcomes: a systematic review. J Hosp Med. (2018) 13:853–9. doi: 10.12788/jhm.3090
35. Verhaegh KJ, MacNeil-Vroomen JL, Eslami S, Geerlings SE, de Rooij SE, Buurman BM. Transitional care interventions prevent hospital readmissions for adults with chronic illnesses. Health Aff. (2014) 33:1531–9. doi: 10.1377/hlthaff.2014.0160
36. Leithaus M, Beaulen A, De Vries E, Goderis G, Flamaing J, Verbeek H, et al. Integrated care components in transitional care models from hospital to home for frail older adults: a systematic review. Int J Integr Care. (2022) 22:28. doi: 10.5334/ijic.6447
37. Li Y, Fu MR, Fang J, Zheng H, Luo B. The effectiveness of transitional care interventions for adult people with heart failure on patient-centered health outcomes: a systematic review and meta-analysis including dose-response relationship. Int J Nurs Stud. (2021) 117:103902. doi: 10.1016/j.ijnurstu.2021.103902
38. Balint M. The Doctor, His Patient and the Illness, 2nd Edn. London; New York: International Universities Press (1957).
39. Brown J, Stewart M, McCracken E, McWhinney IR, Levenstein J. The patient-centred clinical method. 2. Definition and application. Fam Pract. (1986) 3:75–9. doi: 10.1093/fampra/3.2.75
40. Stewart M, Belle J, Wayne W, McWhinney IR, McWilliam CL, Freeman T, et al. Patient—Centered Medicine: Transforming the Clinical Method, 3rd Edn. New York, NY: Radcliffe Publishing (2014). doi: 10.1201/b20740
41. Joo JY, Liu MF. The experience of chronic illness transitional care: a qualitative systematic review. Clin Nurs Res. (2022) 31:163–73. doi: 10.1177/10547738211056166
42. Bratzke LC, Muehrer RJ, Kehl KA, Lee KS, Ward EC, Kwekkeboom KL. Self-management priority setting and decision-making in adults with multi-morbidity: a narrative review of literature. Int J Nurs Stud. (2015) 52:744–55. doi: 10.1016/j.ijnurstu.2014.10.010
43. Unidad Docente Multiprofesional de Atención Familiar y Comunitaria “La Laguna-Tenerife Norte,.” SPICA: Subproceso de Integración y Coordinación Asistencial, La Laguna (2016). Available online at: https://www.programaspica.es/ (accessed August 31, 2022).
44. Health Services Delivery Programme Division of Health Systems and Public Health. WHO Integrated Care Models: An Overview. Geneva: World Health Organization, Regional Office for Europe (2016). Available online at: https://www.euro.who.int/__data/assets/pdf_file/0005/322475/Integrated-care-models-overview.pdf (accessed August 31, 2022).
45. Unidad Docente Multiprofesional de Atención Familiar y Comunitaria “La Laguna-Tenerife Norte.” Unidad Docente de Atención Familiar y Comunitaria, La Laguna. Available online at: www.atencionfamiliar.es
46. Wagner EH, Austin BT, Von Korff M. Organizing care for patients with chronic illness. Milbank Q. (1996) 74:511–44. doi: 10.2307/3350391
47. Wagner EH, Glasgow RE, Davis C, Bonomi AE, Provost L, McCulloch D, et al. Quality improvement in chronic illness care: a collaborative approach. Jt Comm J Qual Improv. (2001) 27:63–80. doi: 10.1016/S1070-3241(01)27007-2
49. Wagner EH. Organizing care for patients with chronic illness revisited. Milbank Q. (2019) 97:659–64. doi: 10.1111/1468-0009.12416
50. Vázquez-Díaz J, Pérez Valencia J, Serrano Martínez M. La continuidad. In:Serrano Martínez M, Casado Vicente V, Bonal Pitz P, , editors. Medicina de Familia. Barcelona: Editorial Ariel SA (2005). p. 201–19.
51. Vazquez-Díaz JR. El despliegue de la función valor. Doctutor, Semfyc (2015). Available online at: https://www.doctutor.es/2015/06/11/el-despliegue-dela-funcion-valor (accessed August 31, 2022).
52. Segredo Pérez AM, García Milian AJ, León Cabrera P, Perdomo Victoria I. Desarrollo organizacional, cultura organizacional y clima organizacional. Una aproximación conceptual. Rev Inf científica para la Dir en Salud INFODIR. (2016) 3521:86–99.
53. Boyd CM, Darer J, Boult C, Fried LP, Boult L, Wu AW. Clinical practice guidelines and quality of care for older patients with multiple comorbid diseases: implications for pay for performance. J Am Med Assoc. (2005) 294:716–24. doi: 10.1001/jama.294.6.716
54. Tambo-Lizalde E, Febrel Bordejé M, Urpí-Fernández AM, Abad-Díez JM. La atención sanitaria a pacientes con multimorbilidad. La percepción de los profesionales Atención Primaria. (2021) 53:51–9. doi: 10.1016/j.aprim.2020.05.013
55. Ministerio de Sanidad,. Estrategia para el Abordaje de la Cronicidad en el Sistema Nacional de Salud. Madrid: Ministerio De Sanidad, Servicios Sociales e Igualdad Igualdad (2021). Available online at: https://servicios.mpr.es/VisorPublicaciones/visordocumentosicopo.aspx?NIPO=133210122&SUBNIPO=&IDPUBLICACION=014613321 (accessed August 31, 2022).
56. Lopez-Valcarcel BG. Family medicine in the crossroad. Risks and challenges. Atencion Primaria. (2020) 52:65–6. doi: 10.1016/j.aprim.2019.12.003
57. Vázquez Díaz JR. Necesidad de nuevos liderazgos en Atención Primaria y Medicina de Familia en España. Atención Primaria. (2022) 54:102282. doi: 10.1016/j.aprim.2022.102282
58. Saultz JW. Defining and measuring interpersonal continuity of care. Ann Fam Med. (2003) 1:134–43. doi: 10.1370/afm.23
59. Ljungholm L, Liljegren AE, Ekstedt M, Klinga C. What is needed for continuity of care and how can we achieve it? Perceptions among multiprofessionals on the chronic care trajectory. BMC Health Serv Res. (2022) 22:1–15. doi: 10.1186/s12913-022-08023-0
60. Kaufman BG, Spivack BS, Stearns SC, Song PH, O'Brien EC. Impact of accountable care organizations on utilization, care, and outcomes: a systematic review. Med Care Res Rev. (2017) 76:255–90. doi: 10.1177/1077558717745916
61. National Health Service. The NHS Long-Term Plan. (2019). Available online at: https://www.longtermplan.nhs.uk/wp-content/uploads/2019/08/nhs-long-term-plan-version-1.2.pdf (accessed August 31, 2022).
Keywords: family practice, multimorbidity, internship and residency, patient care management, patient-centered care, patient discharge, primary health care, transitional care
Citation: García-Hernández M, González de León B, Barreto-Cruz S and Vázquez-Díaz JR (2022) Multicomponent, high-intensity, and patient-centered care intervention for complex patients in transitional care: SPICA program. Front. Med. 9:1033689. doi: 10.3389/fmed.2022.1033689
Received: 31 August 2022; Accepted: 01 November 2022;
Published: 24 November 2022.
Edited by:
Ana Clavería, Instituto de Investigación Sanitaria Galicia Sur (IISGS), SpainReviewed by:
Simin Jahani, Ahvaz Jundishapur University of Medical Sciences, IranMaría Victoria Martín Miguel, Sociedad Española de Reumatología (SER), Spain
Vanja Lazic, Health Center Zagreb, Croatia
Copyright © 2022 García-Hernández, González de León, Barreto-Cruz and Vázquez-Díaz. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: José Ramón Vázquez-Díaz, joseramonvd.mfyclalaguna@gmail.com
†These authors have contributed equally to this work and share first authorship