Minimally invasive epicardial left-ventricular lead implantation and simultaneous left atrial appendage closure
 Johannes Petersen1,2*
Johannes Petersen1,2*  Yousuf Alassar1 Yalin Yildirim1 Tobias Tönnis3 Hermann Reichenspurner1,2
Yousuf Alassar1 Yalin Yildirim1 Tobias Tönnis3 Hermann Reichenspurner1,2  Simon Pecha1,2
Simon Pecha1,2
- 1Department of Cardiovascular Surgery, University Heart and Vascular Center Hamburg, Hamburg, Germany
- 2German Center for Cardiovascular Research (DZHK), Hamburg/Kiel/lübeck, Germany
- 3Department of Cardiology, University Heart and Vascular Center Hamburg, Hamburg, Germany
Background: Atrial fibrillation (AF) is common in patients with heart failure resulting in a high prevalence of AF in patients receiving Cardiac Resynchronization Therapy (CRT) implantation. In patients, unsuitable for transvenous left ventricular (LV)-lead implantation, epicardial LV-lead implantation represents a valuable alternative. Epicardial LV-lead placement can be achieved totally thoracoscopical or via minimally invasive left lateral thoracotomy. In patients with atrial fibrillation, concomitant left atrial appendage (LAA) clipping is feasible via the same access. Therefore, the aim of our study was the analysis of safety and efficacy of epicardial LV lead implantation and concomitant LAA clipping via minimally invasive left-lateral thoracotomy.
Methods: Between December 2019 and March 2022, 8 patients received minimally invasive left atrial LV-lead implantation with concomitant LAA closure using the AtriClip. Transesophageal echocardiography (TEE) was performed to intraoperatively guide and control LAA closure.
Results: Mean patients age was 64 ± 11.2 years, 67% were male patients. Minimally invasive left-lateral thoracotomy was used in 6 patients while a totally thoracoscopic approach was performed in 2 cases. Epicardial lead implantation was successfully performed in all patients with good pacing threshold (mean 0.8 ± 0.2 V) and sensing values (10.1 ± 2.3 mV). Posterolateral position of the LV lead was achieved in all patients. Furthermore, successful LAA closure was confirmed during TEE in all patients. No procedure-related complications occurred in any of the patients. Two patients additionally received simultaneous laser lead extraction during the same procedure. Complete lead extraction was achieved in both patients. All patients were extubated in the OR and had an uneventful postoperative course.
Conclusion: Our study highlights a novel treatment approach for patients with atrial fibrillation and the necessity of epicardial LV leads. Placement of a posterolateral LV lead position with concomitant occlusion of the left atrial appendage via a minimally-invasive left-lateral thoracotomy or even a totally thoracoscopic approach is safe and feasible with superior cosmetic result and complete occlusion of the left atrial appendage.
Introduction
Atrial fibrillation (AF) has a high prevalence in patients with heart-failure (1, 2) and consequently, in patients undergoing cardiac resynchronization therapy defibrillator (CRT-D) implantation (3).
In patients, not suitable for transvenous left ventricular (LV) lead implantation, epicardial lead implantation represents a valuable treatment alternative. Most recently, Burger et al. outlined excellent results of epicardial left-ventricular leads with comparable performance of transvenous leads (4). The advantage of epicardial leads is the selection of the ideal left-ventricular target area, independently from the anatomy of the coronary sinus vein. Furthermore, epicardial LV leads are essential treatment options in patients with systemic cardiac device related infections, which is a rare but severe complication of transvenous device therapy. In case of cardiac device infection, complete lead extraction is recommended in those patients (5). In such patients, especially with pacemaker-dependency, epicardial LV leads are helpful tools to ensure continuous stimulation until resolution of infection is achieved. Epicardial LV-lead placement can be achieved via totally thoracoscopic port-access or left-lateral mini-thoracotomy, allowing for a postero-lateral positioning of the LV-lead (6, 7). In patients with AF, concomitant surgical left-atrial appendage closure resulted in a significant stroke risk reduction (8) and therefore concomitant LAA closure is highly recommended in all AF patients undergoing any type of cardiac surgery. The AtriClip® (Fa. AtriCure, Cincinnati, Ohio) LAA exclusion system can be used in minimally- invasive surgery and allows for successful LAA closure through port-access (AtriClip PRO2®) or left-lateral minithoracotomy (AtriClip Pro®).
Therein, we report our initial experience with left-ventricular lead implantation and concomitant LAA closure via a thoracoscopic port-access- or left-lateral mini-thoracotomy.
Methods
Between December 2019 and March 2022 8 patients were planned for LV lead pacing due to left bundle branch block, QRS duration >130 ms and LV ejection fraction below 35%. All patients (n = 8) scheduled for LV lead implantation had a history of atrial fibrillation and were treated via a minimally invasive epicardial lead implantation and concomitant LAA closure. Indications for epicardial LV lead implantation were previously unsuccessful transvenous LV-lead implantation (n = 6) or systemic infection with pacemaker dependency (n = 2). One patient with systemic infection had a complex anatomical condition of a persistent left superior vena cava. All patients gave written informed consent. All patient data were anonymized and retrospectively analyzed. All data were derived from routine in-hospital courses without follow-up. Herewith, no Institutional Review Board approval is required.
Surgical technique
The procedure was performed using general anesthesia and a double-lumen endotracheal tube under transesophageal echo monitoring. Patient is placed in a supine position and the left side of the chest is elevated to gain access to the posterior axillary line.
Thoracoscopic approach
Totally thoracoscopic access was achieved through three-ports (Figure 1A). One 10 mm camera-port was introduced in the 6th intercostal space in the anterior axillary line and 12 mm working ports were introduced in the posterior axillary line in the 4th and 8th intercostal space. CO2 Insufflation was used during the procedure. Using 3D vision endoscopic guidance, the pericardium is opened 3 cm posterior to the phrenic nerve. An AtriClip PRO2® device (Atricure, West Chester, OH), which can be deployed via a 12 mm working port, was placed at the base of the left atrial appendage. Deployment of the AtriClip was guided by live transesophageal echocardiography in order to achieve complete LAA closure. After satisfactory placement, the AtriClip is released and the deployment device retrieved (Figure 2). Secondary, a Greatbatch Myopore™ screw-in lead was placed in the posterolateral LV-wall using a Greatbatch FASTAC™ delivery tool. Sensing, pacing threshold and impedance measurements are carried out. If the electrode values were satisfactory (Pacing threshold ≤1.5 V at 0.5 ms, Sensing ≥5 mV and Impedance between 300 and 1,500 Ω) the end of the lead was externalized, and tunneled into the pacemaker pocket. If measurements were not sufficient, an alternative lead position was used and measurements were performed again. At the end the pericardium is closed and a chest tube is placed through one of the working ports into the left pleural space. Ports are removed and the incisions are closed.
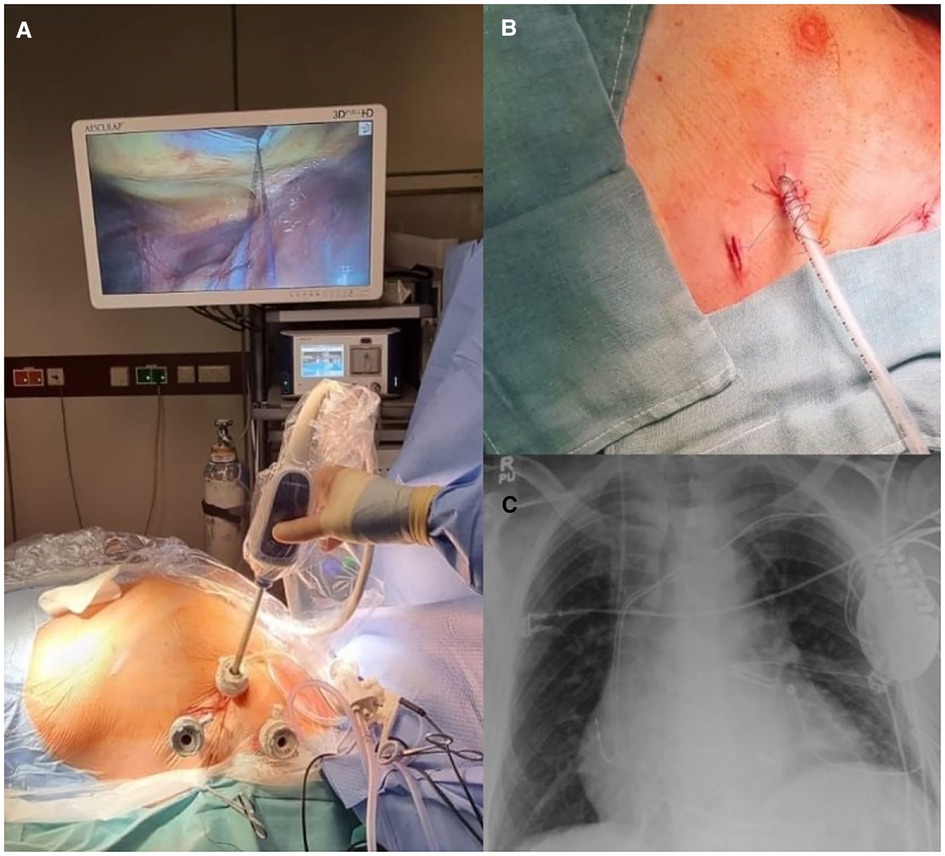
Figure 1. (A) Intraoperative picture showing the three-port access and the 3D videoscopic guidance. (B) Postoperative state after wound closure. (C) Postoperative chest x-ray showing the CRT-D device with the epicardial LV lead and the AtriClip PRO2® device.
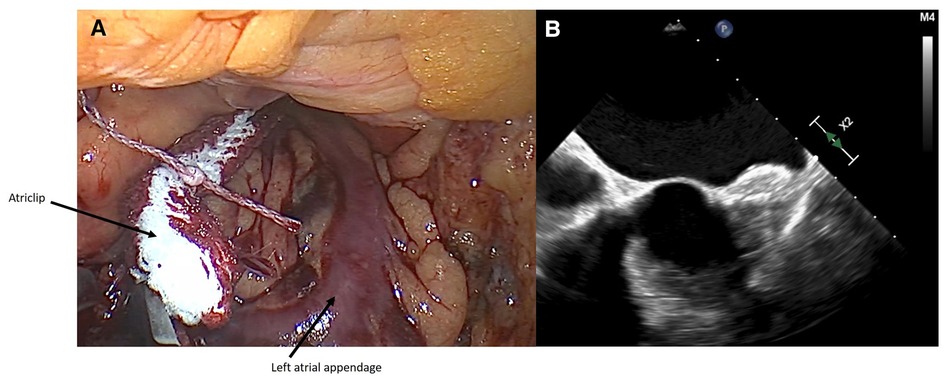
Figure 2. (A) intraoperative closure of LAA with AtriClip PRO2® device. (B) Intraoperative transesophageal echocardiography showing successful closure of LAA.
Minimally invasive left-lateral thoracotomy
Minimally-invasive access was achieved via a 3–5 cm lateral minithoracotomy through the 4th intercostal space on the left side of the chest (Figure 3C). Next, a soft-tissue retractor is inserted. Under direct vision, the pericardium is opened 3 cm posterior to the phrenic nerve. Pericardial stay sutures are placed. An AtriClip PRO® is used to close the LAA at the base with similar confirmation by transesophageal echocardiography. Secondary, a Greatbatch MyoporeTM screw-in lead was placed in the posterolateral LV-wall under direct vision, without necessity of an additional delivery tool. When satisfactory lead measurements are achieved, the pericardium is closed under direct vision and a chest tube is placed.
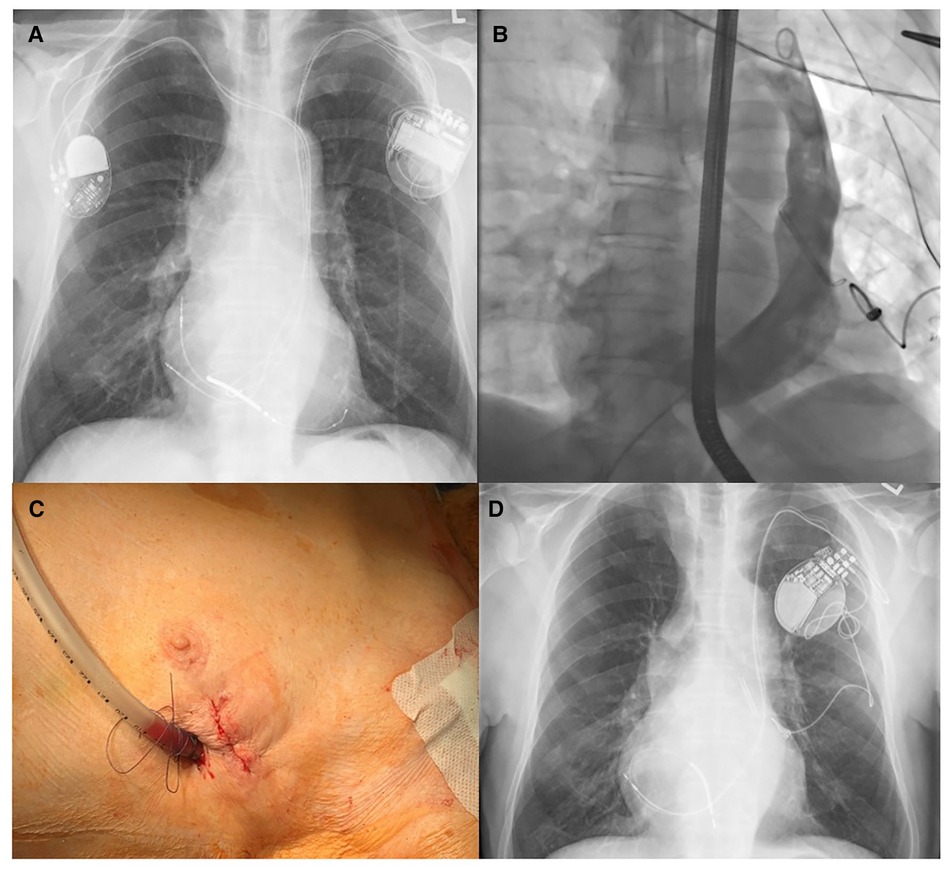
Figure 3. (A) Preoperative chest x-ray showing the left-sided CRT-D device and the right-sided pacemaker through left-sided superior vena cava (SVC). (B) Intraoperative venography, after extraction of all leads, displaying the left-sided SVC and the epicardial LV-lead as well as the AtriClip®. (C) Minimally invasive left-lateral incision in the fourth intercostal space after wound closure. (D) Postoperative chest x-ray showing the AtriClip® and the LV lead connected to a single-chamber pacemaker.
Laser lead extraction
Laser lead extraction was performed in two patients with systemic device related infection and pacemaker dependency as previously described (9). All procedures were performed under fluoroscopic guidance in a hybrid operating room under general anaesthesia. A transoesophageal echocardiography probe was placed to monitor for pericardial or pleural effusion. All patients were prepared for emergent sternotomy with cardiopulmonary bypass standby. Leads were dissected from the scar tissue and the sleeves were removed. Lead locking devices were placed into the lumen of the leads. Laser lead extraction was conducted using Spectranetics 16 F GlideLight (80 Hz) laser sheaths (Spectranetics Corporation, Colorado Springs, CO, USA). Laser lead extractions were performed with a single sheath technique and without outer sheaths.
Postoperative
Patients are extubated in the operating room and transferred towards the general ward after the procedure. Chest x-ray is performed on the day of surgery. Pacemaker/ICD interrogation is performed and chest tube drain is removed on the 1st postoperative day. Anticoagulation is maintained according to CHADS2-VASc Score.
Statistics
Continuous variables are expressed as mean ± standard deviation (SD) for normal distributions and median and interquartile range (IQR) for non-gaussian distributions. Categorial variables are shown as counts and percentages. Statistical analysis was performed using IBM SPSS 25.0 statistical software package (IBM, Armonk, NY, USA).
Results
Patient demographics
Baseline patient characteristics are outlined in Table 1. Mean patients age was 64 ± 11.2 years, 75% were male patients. Ejection fraction was severely reduced in all patients (23.8 ± 4.8%) with heart failure symptoms of NYHA class III and IV. Three patients had paroxysmal AF whereas five patients had persistent AF.
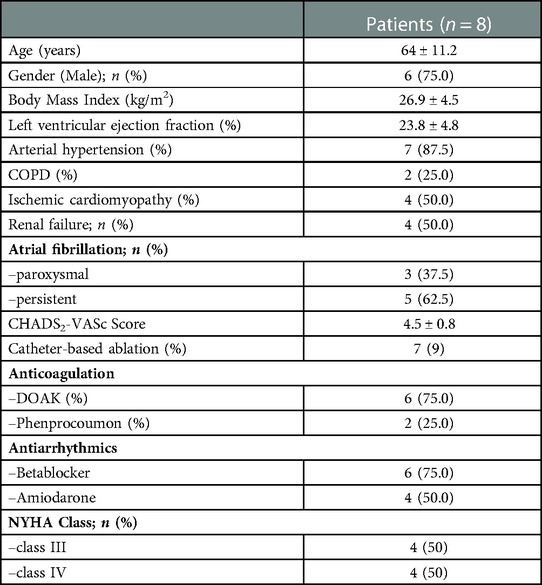
Table 1. Patient demographics.
Perioperative data
The perioperative data is outlined in Table 2. Epicardial lead implantation was successfully performed in all patients with good pacing threshold (mean 0.8 ± 0.2 Volt at 0.5 ms) and sensing values (10.1 ± 2.3 mV). Posterolateral position of the LV lead was achieved in all patients. Furthermore, successful LAA closure was confirmed during transesophageal echocardiography in all patients. Mean procedural time with totally thoracoscopic approach (n = 2) was 116 min whereas the procedure time for the minimally invasive left-lateral thoracotomy approach without laser lead extraction (n = 4) was shorter (72 min). The procedure with additional laser lead extraction was 132 min. All patients were extubated in the OR immediately after the procedure and transferred to the general ward on the same day of surgery. No procedure related complications occurred in any of the patients.
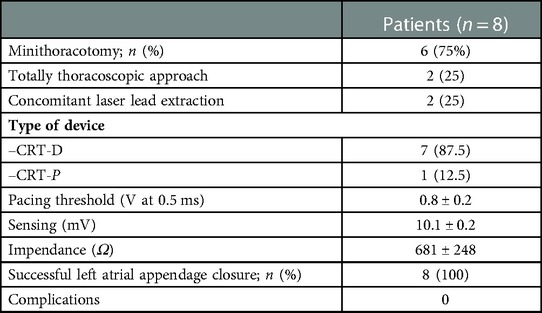
Table 2. Results and complications.
Mean duration of in-hospital stay was 3.8 ± 1.6 days in patients without systemic device-related infection. Hospital stay of the two patients with systemic infection was prolonged due to intravenous antibiotic treatment (36 and 41 days).
Discussion
Herewith, we highlight the possibility of epicardial LV-lead implantation and concomitant closure of the left-atrial appendage through the same totally thoracoscopic port-access- or a minimally invasive left-lateral thoracotomy.
Our described approach allows for minimally-invasive epicardial lead implantation with less surgical trauma and also enables for ideal LV-lead placement, independently from any coronary sinus anatomy. Furthermore, using this access, a posterolateral positioning of the lead can be achieved, which is essential in order to achieve a sufficient cardiac resynchronization therapy. Especially, in patients not suitable for endovascular LV lead implantation, this approach represents an excellent alternative treatment algorithm. Most recently, Burger et al. published their experiences of epicardial LV leads in 158 patients with low complication rates and excellent long-term performance with only a 1.9% lead revision rate at five years (compared to 10.2% for transvenous leads).
In addition, we have shown a treatment algorithm for patients with device endocarditis requiring lead removal, pacemaker dependency and atrial fibrillation. Systemic device related infection represents a rare but serious complication of device therapy, associated with significant morbidity and mortality (10). In systemic device related infection, extraction of all lead material is recommended as a class I indication (11). Especially, patients with pacemaker dependency and systemic infection represent a clinically challenging cohort, since there is a need for a bridging solution. Epicardial LV leads have the benefit of no foreign material in the vascular space, which helps as a bridging option until treatment of systemic infection has been accomplished. For instance, transcutaneous pacing with an externalized pacer can be used as a bridging solution with good results (12). Once the systemic infection is effectively treated, the epicardial LV lead can be easily combined with endovascular right ventricular (RV) and right atrial (RA) leads and a sufficient CRT therapy can be facilitated. Recent studies confirmed the safety of a video-assisted thoracoscopic placement of epicardial LV leads with excellent long-term outcome (6, 7).
Heart failure is often accompanied by atrial fibrillation and therefore many patients presenting for CRT-D implantation suffer from atrial fibrillation (3). A recently published prospective randomized trial, the LAAOS III Study has shown the beneficial effects of concomitant surgical LAA closure in patients with AF undergoing cardiac surgery (8). In the LAAOS III study, a significant stroke reduction has been observed during follow-up, without any evidence of procedure-related adverse events. Therefore, concomitant surgical LAA closure is strongly recommended in patients with AF undergoing any cardiac surgical procedure. This applies on the one hand to conventional surgical procedures (e.g., coronary artery bypass surgery, aortic valve replacement, or mitral valve surgery) but can also be used in other procedures like epicardial LV lead placement. Our study highlights this new approach whereas LAA closure using an epicardial clip can be performed safe and easy. Especially in patients with a high CHA2DS2-VASc Score or a history of stroke, concomitant closure of the LAA is beneficial. For instance, interventional LAA closure proved to be a therapeutic alternative in patients with high bleeding risk or contraindication for anticoagulation. In terms of stroke reduction, interventional LAA occlusion showed to be equally effective as anticoagulation therapy (13, 14). Another most recent study showed that totally thoracoscopic epicardial appendage occlusion without any antithrombotic therapy appears to be safe and effective. Branzoli et al. proposed that this strategy could be advised for stroke prevention in patients with high risk of bleeding (15).
A recent retrospective multicenter study of 175 high stroke risk patients treated by thoracoscopic stand-alone LAA closure using the AtriClip underlined the safety and efficacy of this technique. Procedural success was 99.4% and no stroke occured during a median follow-up duration of 12.5 months besides a predicted stroke rate was 4.8/100 patient-years (calculation based on median CHA2DS2-VASc Score) (16). Besides reduction of stroke risk, the AtriClip provides electrical isolation of the LAA which can be accountable for up to 27% of atrial arrhythmias (17).
Guarricini et al. reported two patients with left atrial appendage closure and concomitant LV epicardial lead implantation via a totally thoracoscopic approach (18). However, our study highlights different approaches to combine LV epicardial lead implantation and LAA closure in a larger patient series. Depending on the clinical scenario either totally thoracoscopic or minimally-invasive left-lateral thoracotomy can be used. This approach combines the benefits of both procedures: exact positioning of the LV lead at a posterolateral position, stroke reduction by complete occlusion of the LAA and a minimized surgical trauma with excellent cosmetic results. Combined with short procedure-times, immediate postoperative extubation and early mobilization according to the principles of enhanced recovery after surgery (19) the patients can be discharged three to four days after surgery. In addition, the totally thoracoscopic approach is a very elegant approach, which however increases the costs in comparison to a thoracotomy approach in terms of materials (FATSTAC Applicator for LV lead and Atriclip Pro2 instead of Atriclip Pro). Therefore our alternative direct vision thoracotomy approach with a 4 cm incision presents an even more cost-effective option.
Limitation
This is a retrospective study with a small patient series. However, this is the largest reported patient series of this novel approach. Since it's a new technique, we report only in-hospital outcome and further follow-up is necessary to analyze long-term outcome and potential stroke risk reduction.
Conclusion
Our study highlights a novel treatment approach for patients with atrial fibrillation and the necessity of epicardial LV leads due to complex anatomical conditions, device endocarditis requiring lead removal or pacemaker dependency. Placement of a posterolateral LV lead position with concomitant occlusion of the left atrial appendage via a minimally-invasive left-lateral thoracotomy or even a totally thoracoscopic approach is safe and feasible with superior cosmetic results and complete occlusion of the left atrial appendage.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
Ethics statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author contributions
JP: conceptualization, data curation, formal analysis, methodology, investigation, and writing of original draft. YA: conceptualization, supervision and review and editing of draft. YY and TT: methodology, review and editing of draft. HR: methodology, resources, supervision, and review and editing of draft. SP: project administration, conceptualization, supervision, writing, review and editing of draft. All authors contributed to the article and approved the submitted version.
Conflict of interest
SP is a consultant for Philips Healthcare. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Anter E, Jessup M, Callans DJ. Atrial fibrillation and heart failure: treatment considerations for a dual epidemic. Circulation. (2009) 119:2516–25. doi: 10.1161/CIRCULATIONAHA.108.821306
2. Santhanakrishnan R, Wang N, Larson MG, Magnani JW, McManus DD, Lubitz SA, et al. Atrial Fibrillation Begets Heart Failure and Vice Versa: temporal Associations and Differences in Preserved Versus Reduced Ejection Fraction. Circulation. (2016) 133:484–92. doi: 10.1161/CIRCULATIONAHA.115.018614
3. Maisel WH, Stevenson LW. Atrial fibrillation in heart failure: epidemiology, pathophysiology, and rationale for therapy. Am J Cardiol. (2003) 91:2D–8D. doi: 10.1016/S0002-9149(02)03373-8
4. Burger H, Pecha S, Hakmi S, Opalka B, Schoenburg M, Ziegelhoeffer T. Five-year follow-up of transvenous and epicardial left ventricular leads: experience with more than 1000 leads. Interact Cardiovasc Thorac Surg. (2020) 30:74–80. doi: 10.1093/icvts/ivz239
5. Blomstrom-Lundqvist C, Traykov V, Erba PA, Burri H, Nielsen JC, Bongiorni MG, et al. European Heart Rhythm Association (EHRA) international consensus document on how to prevent, diagnose, and treat cardiac implantable electronic device infections-endorsed by the Heart Rhythm Society (HRS), the Asia Pacific Heart Rhythm Society (APHRS), the Latin American Heart Rhythm Society (LAHRS), International Society for Cardiovascular Infectious Diseases (ISCVID) and the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Europace. (2020) 22:515–49. doi: 10.1093/europace/euz246
6. Marini M, Branzoli S, Moggio P, Martin M, Belotti G, Molon G, et al. Epicardial left ventricular lead implantation in cardiac resynchronization therapy patients via a video-assisted thoracoscopic technique: long-term outcome. Clin Cardiol. (2020) 43:284–90. doi: 10.1002/clc.23300
7. Kim HR, Lim K, Park SJ, Park JS, Kim JY, Chung S, et al. Thoracoscopic implantation of epicardial left ventricular lead for cardiac resynchronization therapy. J Cardiovasc Dev Dis. (2022) 9(5):160. doi: 10.3390/jcdd9050160.35621871
8. Whitlock RP, Belley-Cote EP, Paparella D, Healey JS, Brady K, Sharma M, et al. Left atrial appendage occlusion during cardiac surgery to prevent stroke. N Engl J Med. (2021) 384:2081–91. doi: 10.1056/NEJMoa2101897
9. Pecha S, Castro L, Gosau N, Linder M, Vogler J, Willems S, et al. Evaluation of tricuspid valve regurgitation following laser lead extraction†. Eur J Cardio-Thorac Surg. (2017) 51:1108–11. doi: 10.1093/ejcts/ezx011
10. Pecha S, Burger H, Chung DU, Möller V, Madej T, Maali A, et al. The German laser lead extraction RegistrY: gALLERY. Europace: Eur Pacing Arrhythmias Card Electrophysiol. (2022) 24:1627–35. doi: 10.1093/europace/euac056
11. Kusumoto FM, Schoenfeld MH, Barrett C, Edgerton JR, Ellenbogen KA, Gold MR, et al. 2018 ACC/AHA/HRS guideline on the evaluation and management of patients with bradycardia and cardiac conduction delay: a Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. Heart Rhythm. (2019) 16:e128–226. doi: 10.1016/j.hrthm.2018.10.037
12. Pecha S, Aydin MA, Yildirim Y, Sill B, Reiter B, Wilke I, et al. Transcutaneous lead implantation connected to an externalized pacemaker in patients with implantable cardiac defibrillator/pacemaker infection and pacemaker dependency. Europace: Eur Pacing Arrhythmias Card Electrophysiol. (2013) 15:1205–9. doi: 10.1093/europace/eut031
13. Holmes DR, Reddy VY, Turi ZG, Doshi SK, Sievert H, Buchbinder M, et al. Percutaneous closure of the left atrial appendage versus warfarin therapy for prevention of stroke in patients with atrial fibrillation: a randomised non-inferiority trial. Lancet (London, England). (2009) 374:534–42. doi: 10.1016/S0140-6736(09)61343-X
14. Holmes DR J, Kar S, Price MJ, Whisenant B, Sievert H, Doshi SK, et al. Prospective randomized evaluation of the watchman left atrial appendage closure device in patients with atrial fibrillation versus long-term warfarin therapy: the PREVAIL trial. J Am Coll Cardiol. (2014) 64:1–12. doi: 10.1016/j.jacc.2014.04.029
15. Branzoli S, Guarracini F, Marini M, D'Onghia G, Catanzariti D, Merola E, et al. Heart team for left appendage occlusion without the use of antithrombotic therapy: the epicardial perspective. J Clin Med. (2022) 11(21):6492. doi: 10.3390/jcm11216492
16. Cartledge R, Suwalski G, Witkowska A, Gottlieb G, Cioci A, Chidiac G, et al. Standalone epicardial left atrial appendage exclusion for thromboembolism prevention in atrial fibrillation. Interact Cardiovasc Thorac Surg. (2022) 34:548–55. doi: 10.1093/icvts/ivab334
17. Di Biase L, Burkhardt JD, Mohanty P, Sanchez J, Mohanty S, Horton R, et al. Left atrial appendage: an underrecognized trigger site of atrial fibrillation. Circulation. (2010) 122:109–18. doi: 10.1161/CIRCULATIONAHA.109.928903
18. Guarracini F, Branzoli S, Marini M, Guarracini S, Di Mauro M, Calafiore AM, et al. Totally thoracoscopic concomitant left atrial appendage closure and left ventricular epicardial lead implantation. J Card Surg. (2021) 36:4403–06. doi: 10.1111/jocs.15928
Keywords: minimally-invasive, totally thoracoscopic, epicardial lead placement, left atrial appendage closure, atrial fibrillation
Citation: Petersen J, Alassar Y, Yildirim Y, Tönnis T, Reichenspurner H and Pecha S (2023) Minimally invasive epicardial left-ventricular lead implantation and simultaneous left atrial appendage closure. Front. Cardiovasc. Med. 10:1129410. doi: 10.3389/fcvm.2023.1129410
Received: 21 December 2022; Accepted: 15 February 2023;
Published: 10 March 2023.
Edited by:
Patrick Badertscher, University Hospital of Basel, SwitzerlandReviewed by:
Massimiliano Marini, Santa Chiara Hospital, ItalyTeodor Serban, Cardiovascular Research Institute Basel (CRIB), Switzerland
© 2023 Petersen, Alassar, Yildirim, Tönnis, Reichenspurner and Pecha. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Johannes Petersen joh.petersen@uke.de
Specialty Section: This article was submitted to Cardiac Rhythmology, a section of the journal Frontiers in Cardiovascular Medicine