
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Indexing
- Current Issue
- Past Issue
 Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices
Journal of Public Health Issues and Practices Volume 2 (2018), Article ID: JPHIP-143
https://doi.org/10.33790/jphip1100143Research Article
The Affecting Factors of Premenstrual Syndrome in Female College Students with Disabilities in Taiwan
Chu-Mei Lan1*, Tsung-Ming Su2
1Assistant Professor, Department of Health Psychology, College of Health Sciences, Chang Jung Christian University, No.1,Changda Rd., Gueiren District, Tainan City 711, Taiwan (R.O.C.).
2Department of Neurosurgery, Kaohsiung Chang Gung Memorial Hospital and Chang Gung University College of Medicine, No. 123 Dapi Road, Niaosong District, Kaohsiung City 83301, Taiwan.
Corresponding Author Details: Chu-Mei Lan, Assistant Professor, Department of Health Psychology, College of Health Sciences, Chang Jung Christian University, No.1,Changda Rd.,Gueiren District, Tainan City 711, Taiwan (R.O.C.). Fax:+886-6- 2785138. E-mail: cmlan@mail.cjcu.edu.tw
Received date: 16th June, 2019
Accepted date: 17th July, 2019
Published date: 23th July, 2019
Citation: Lan CM, Su TM (2019) The affecting factors of premenstrual syndrome in female college students with disabilities in Taiwan. J Pub Health Issue Pract 3: 143.
Copyright: ©2019, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
Objective: This study measured the symptoms of Premenstrual Syndrome (PMS) and explored the affecting factors and predictors in female students with disabilities.
Materials and Methods: This is a cross-sectional and quantitative study. The subjects were female college students with disabilities who were recruited from Taiwan through college counseling centers using cluster random sampling. A total of 180 subjects completed valid questionnaires. The research data was analyzed by SPSS Version 18.0 through independent t-test and stepwise regression.
Results: The mean age of participants was 20.85 years. The most severe and remissive symptoms were irritability, unstable mood and lack of energy. There was high prevalence of PMS for female students with disabilities (97.2%). The affecting factors of the severe PMS were gynecological disease, diet, family menstruation uncomfortable history, irregularity, lifestyle, irregular diet, learning hassles, interpersonal hassles, and irregular exercise. The crucial predictors of the severity of PMS were interpersonal hassles, gynecological disease, and irregular exercise. The explained proportion of variance was 16.9%, while the affecting factors of the remission of PMS were the severity of PMS and acceptance of mindfulness, while the crucial predictors of the remission of PMS were the same two factors. The explained proportion of variance was 67.3%.
Conclusion: This study offers suggestions for how to manage PMS by exercise, diet, healthy lifestyle, decreasing psychological disturbances, and offering mindfulness practices. Allowing mindfulness philosophy to be practiced in students’ daily lives can improve their symptoms of PMS.
Key words: Female college students with disabilities, Premenstrual Syndrome (PMS), the Affecting factors
Introduction
Premenstrual syndrome (PMS) is a herd of psychological and somatic symptoms occurring specifically during the last half of the luteal phase of the menstrual cycle and subsiding at the end of menstruation [1]. The studies about premenstrual syndrome (PMS) and its more severe counterpart, premenstrual dysphoric disorder (PMDD) have rarely focused on Taiwanese students with disabilities. PMDD is accompanied with social and occupational disabilities; especially, there is mood distress, behavioral disturbances and physical problems that emerge to affect female function and quality of life [2]. Many women in Taiwan experience disturbance in their lives because of their menstruation cycles, with psychological problems, emotional problems, and pain being the most common complaints in PMS [3].
Prevalence of PMS was 50%-92.3% and that of PMDD was 3-8% among female university students in two studies [4,5]. The most common symptoms were fatigue with correspondent decreased interest in daily activities [5], body ache/joint pain and feeling depressed/blue respectively [6], irritability, breast fullness, and abdominal distension [1]. More than 70 % subjects reported symptoms that they had been dealing with using some medication; however, more than half of the students had never sought help [1]. In women with intellectual disability, cramps, hot flushes, affection, orderliness, excitement, and bursts of energy/activity were the most prevalent symptoms during the perimenstrual phase [7]. There was an 82–95% prevalence rate of premenstrual symptoms, such as irritability, tension, fatigue, and dysphoria among Taiwanese college students [8].
A study of medical students of an Indian medical college found that PMDD was present in 37% of the participants, a higher rate in older and postgraduate students. Lifestyle factors, sleep, physical activity, total tea/coffee intake, and change in tea/coffee and food intake under stress were significantly related to PMDD [6]. PMDD prevalence rate was higher among older students than younger students [4]. PMDD patients had significantly higher scores on the Neuroticism Scale on the Eysenck Personality Inventory (EPI) [5] and the condition induced female students’ academic performance to become poorer [4]. The participants’ unique characteristics such as level of intellectual disability, marital status and their specific background and experiences in reproduction and sexuality were associated with PMS [7]. Consumption of caffeine-containing drinks may cause PMS [9]. The consumption of caffeine-containing drinks and the presence and severity of PMS revealed a strong relationship. More consumption of caffeine-containing drinks manifested more presence and severity of PMS [9].
Actually, studies of PMS among college students with disabilities are rare in Taiwan. Chou, Lu, and Pu studied women with intellectual disability, and they addressed that special attention should be paid to the experiences and perceptions of PMS in such subjects [9]. Accordingly, this study’s subjects were female college students with disability.
The purposes of the present study were as follows: (1) to explore the background information, mindfulness level, and PMS status of female college students with disabilities in Taiwan; (2) to confirm the relationships of PMS status with background information and mindfulness level; and (3) to explore the crucial predictors of PMS in female college students with disabilities.
Materials and Methods
Methods
Participants and procedures
This is a cross-sectional study. The participants were informed of the study’s purpose and procedures by following the instructions from the documents advised by the National Cheng Kung University Human Research Ethics Committee (No. 104-279). The participants were female college students with disabilities and having a disability as categorized according to the World Health Organization ( WHO ) International Classification of Functioning, Disability, and Health ( ICF ), and were recruited from 20 universities in Taiwan using cluster random sampling. The research assistant approached the guidance teachers of college counseling centers by e-mail and telephone to explain the research procedure, then, these guidance teachers assisted their students with disabilities to complete the paper questionnaire, with a valid returned number of 180 copies.
Instruments
Demographics and background information
The scale used in this study was developed from those of previous studies [2,6,10]. The questionnaire was included of age, grade, nationality, academic accomplishment, regularity of menstruation, level of mindfulness, amount of exercise, daily lifestyle, diet, family history of PMS, gynecological disease, and number of daily disturbances. Premenstrual Syndrome Scale (PMSS). The PMSS used in this study was developed and revised from previous studies [11-13]. There were psychological and physical dimensions in PMSS. The psychological dimension included items like as mood instability, loss of energy, hopelessness and comprised 10 items. The physical dimension had 13 items, including those on change in appetite, abdominal not comfortable, increased weight, and muscle pain. PMSS was to measure the student’s premenstrual symptoms from the past 12 months. The symptoms were divided into severity and remission. Severity was reported using a 4-point Likert scale by no, mild, moderate, and severe (0, 1, 2, 3 ). Remission was reported using a 4-point Likert scale by no symptom, continued, remission, and disappeared (0, 1, 2, 3 ). Higher scores on the scale indicate higher of severity and remission. The internal consistency alpha and Kaiser– Meyer–Olkin (KMO) of sampling adequacy were more than .90.
Mindfulness Scale (MS)
The MS was developed for this study from several studies [14-16]. The MS had a total of 7 items and two dimensions (awareness and acceptance). The awareness dimension included 3 items like: “I am aware of my body” ;“I am aware of my mood and feelings” ;“I am aware of my thoughts or ideas.” in the moment of doing something. The acceptance dimension had 4 items: “I avert my thoughts in the moment of doing something”; “I recognize and try to accept them when I have thought disturbances,”; “I recognize and try to experience them when I have feelings of distress,”; “I accept the feeling in my body.” The MS was scored from completely disagree to completely agree (1-5). Higher scores on the scale indicate higher levels of mindfulness. The internal consistency alpha and KMO of sampling adequacy were more than .90.
Data analysis
SPSS version 18.0 was used to analyze the research data by employing descriptive analysis, Pearson product–moment correlation, independent t-test, and stepwise regression.
Results
The mean age of participates was 20.85 years, 42.2 % of participants were medium-severe in their disability degree, 32.8% had hearing disorders, and 23.3% had physical disorders. More than half of the students in their academic accomplishment were lower than their classmates, their menstruation cycle was regular, their life style was irregular, 80.6% had no gynecological disease, 46.1% of them drank hot beverages, while 60.6% of them reported their symptoms did not influence daily life during menstruation duration. The most disturbances of their daily life were learning, career and interpersonal hassles. Only 11.7% of the participants had psychiatric disorders and 36.1% of them had a family history of uncomfortable menstruation (Table 1).
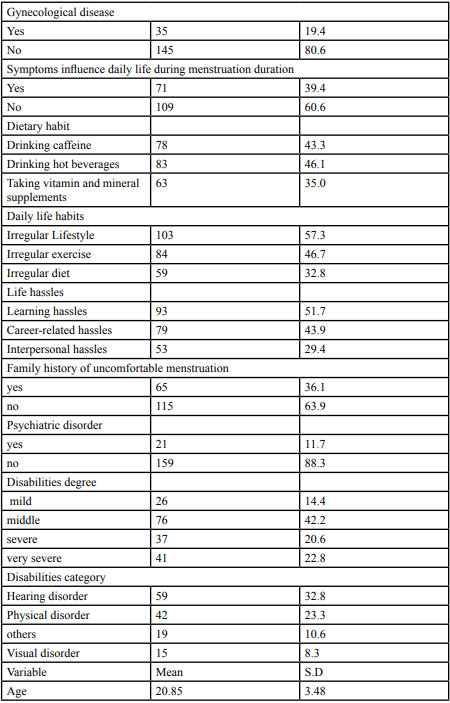
Table: 1 Participants’ demographics and other background information
The mean score of mindfulness in each item was between general to agree (mean= 3.53) and awareness was more than acceptance. The severity and remission of PMS was mental symptoms more than physical symptoms. The most severe and remission symptoms were irritable, mood unstable and lack of energy. There was highly prevalence of PMS for female student of disabilities (97.2%) (Table 2).
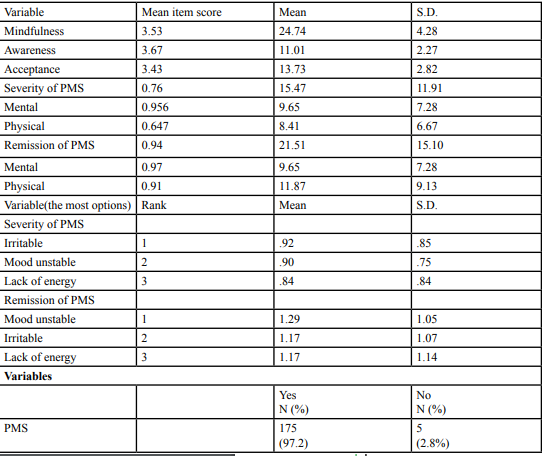
Table: 2 Mindfulness and PMS in college students with disabilities.
Gynecological disease, irregular lifestyle, irregular exercise, irregular diet, learning hassles, interpersonal hassles, family history of uncomfortable menstruation and the severity of PMS had significant relationships. Gynecological disease was significantly related with the remission of PMS. Acceptance and the severity of PMS had positive relationship (Table 3).
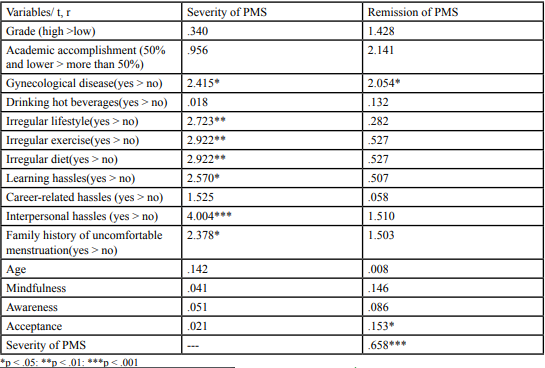
Table: 3 The relationships of foundational data, mindfulness and PMS.
The crucial predictors of the severity PMS were interpersonal hassles, gynecological disease, irregular exercises. The explained proportion of variance was 16.9%. The crucial predictors of the remission of PMS were severity of PMS and acceptance of mindfulness. The explained proportion of variance was 67.3% (Table 4).
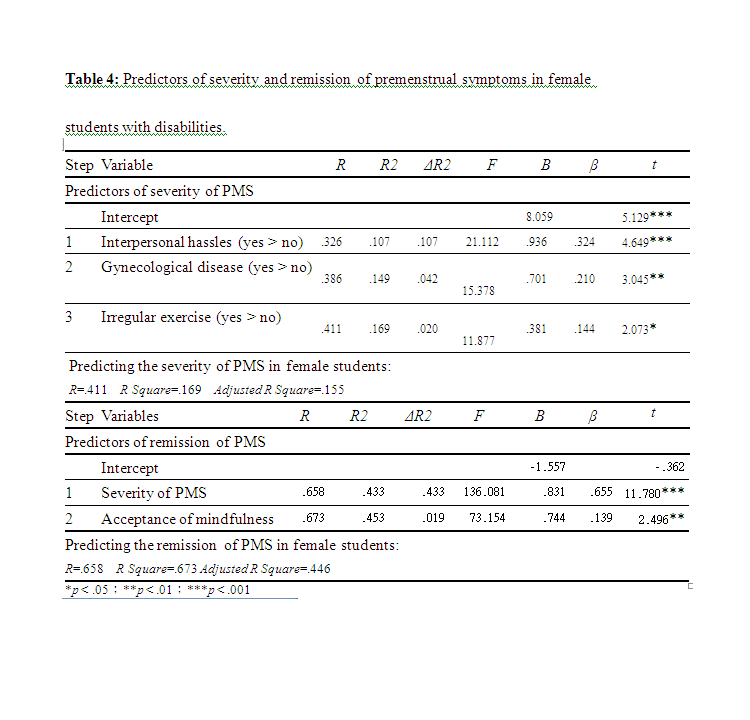
Table: 4 Predictors of severity and remission of premenstrual symptoms in female students with disabilities.
Discussion
From this results presented that 60.6% of participates reported their symptoms did not influence daily life during menstruation duration. The author supposed that most disabilities could cope their symptoms of PMS, basing on most of their symptoms were mild and they had abilities to copy their distress from their disabilities, so that their lives were not affecting more. The most disturbances of their daily life were learning, career and interpersonal hassles. Those results were compatible with Guo et al. found that college students are constantly influenced by the intensive demands of developmental and academic tasks [17].
The most severe and remission symptoms were irritable, mood unstable and lack of energy. Those results were compatible with Naeimi address that the most common mood- and physiology-related symptoms were fatigue [11]. The most severe symptoms of PMS for college students with disabilities were compatible with adult women showed that tension and irritability were the most severe symptoms [18]. There were 97.2% of PMS for female student of disabilities in this study that mean PMS was more popular than general female college students [11].
Students had under conditions that gynecological disease, irregular lifestyle, irregular exercise, irregular diet, learning hassles, interpersonal hassles, a family history of uncomfortable menstruation, their PMS were more sever. Therefore, gynecological disease induced hypothalamus–gonadal cyclicity, that might affect PMS [2]. Lifestyle and physical activity was related with menstrual symptoms [6]. People with a healthy diet, their PMS were significantly reduced [19]. Stress had a strong relationship with PMS [20]. Significant correlations were found between the premenstrual severity and functional impairment, social impairment, and occupational impairment [18]. A family history of uncomfortable menstruation was significantly related with PMS [21]. These results were compatible with pre-studies.
Students had gynecological disease, more acceptance of mindfulness; the more severe of PMS, the more remission of PMS were in this study. PMS occurs 1 to 2 weeks before menstruation and disappears after menstruation [22], so that the severity and remission of PMS were paired. Mindfulness increased positive health perceptions that was supported by this study [23].
The predictors of the severity PMS were interpersonal hassles, gynecological disease, irregular exercises that were compatible with previously reported that traumatic events, history of anxiety disorder, and elevated daily hassle score were the predictors of PMDD [24]. The predictors of the remission of PMS were severity of PMS, acceptance of mindfulness; and the explained proportion of variance was 67.3%. Mindfulness programs have effectively reduced feelings of stress, increased positive health perceptions and health behaviors [23]. Nonjudgmental facets of mindfulness was related with positive functioning significantly [25].
There were 77.3 % subjects had been using some medication; however, 57.6 % students had never sought help [1]. The related however, 57.6 % students had never sought help [1]. The related health education programs to share their experiences across their menstrual cycles; to understand the relationship between womanhood and menstruation; and to learn how to live with their body was important for women [7].
Based on these results, for preventing and remission the symptoms of PMS among college students with disabilities, several suggestions were offered as following. First, the staffs in the health center of colleges can track the students with gynecological disease, to understand their family history of PMS, offering the knowledge of health life style such as regular diet, regular exercises and so on. Second, the counselors in the counseling center of colleges can help to deal with students’ learning hassles and interpersonal hassles, especially when they have the symptoms of PMS, which will help students to copy their physical and mental symptoms. Third, mindfulness program maybe offered from mindfulness education group. By offering information and practicing, educating the skills of mindfulness, addressing acceptance and experiencing the feeling in physical and mental dimensions, when students with PMS. Let the mindfulness philosophy be practice in students’ daily lives and improve their health.
The limitation of this study was small sample size, affecting the representative of sample. Future research could extent sample size and examine the moderators and mediators between mindfulness and PMS. This is cross-sectional study; there are more longitudinal study to follow the symptoms of PMS for college students with disabilities.
Conclusion
The affecting factors of the severity PMS were gynecological disease, family menstruation uncomfortable history, irregular lifestyle, irregular diet, learning hassles, interpersonal hassles, and irregular exercise. The predictors of the severity PMS were interpersonal hassles, gynecological disease, irregular exercises and the explained proportion of variance was 16.9%. The predictors of the remission of PMS were severity of PMS, acceptance of mindfulness; and the explained proportion of variance was 67.3%.
Acknowledgments
I would like to thank the teachers and students of University in Taiwan. The Ministry of Science and Technology, Taiwan, R.O.C., offered the funding for this study (MOST105-2633-S-309-001-).
Conflict of Interest
Authors report there is no conflict of interest of any kind and attests to the originality of this work.
References
Guler T, Yavuz U, O¨ zkum D, Demirdamar R (2013) Effects of perimenstrual complaints on sexuality and disability and coping strategies of university students. Sexuality & Disability 31: 93–101.
Cunningham J, Yonkers KA, O’Brien S, Eriksson E (2009) Update on research and treatment of premenstrual dysphoric disorder. Harvard Rev Psychiat 17: 120–137.View
Chen WY, Chen A (2013) A discussion on the impacts of physical fitness activities on premenstrual syndrome. J Exerc Health Res 3: 57–71.
Shehadeh JH, Hamdan-Mansour AM (2018) Prevalence and association of premenstrual syndrome and premenstrual dysphoric disorder with academic performance among female university students. Perspect Psychiatr C 54: 176-184.View
Singh C, Jain J, Singh J, Jain M, Chaudhary A (2016) A study of premenstrual dysphoric disorder prevalence, phenomenology and personality factors in college going students. Ind J Health and Wellbeing 7: 962-965.
Mishra A, Banwari G, Yadav P (2015) Premenstrual dysphoric disorder in medical students residing in hostel and its association with lifestyle factors. Ind Psychiatry J 24: 150-7.View
Chou YC, Lu JZ, Pu CY (2009) Prevalence and severity of menstrual symptoms among institutionalised women with an intellectual disability. J Intell Dev Dis 34: 36–44.View
Zou LC (1994) A questionnaire survey of psychosomatic symptoms related to menstruation cycle among college female students. Public Health 20: 343–352. [In Chinese].
Rossignol AM (1985) Caffeine-containing Beverages and Premenstrual Syndrome in Young Women. Am J Public Health 75: 1335-1337.View
Liang HJ, Pan WL (2007) A Survey of Premenstrual Syndrome and Its Related Factors of the Adolescents. Chang Gung Nursing, 18: 32 - 44.
Naeimi N (2015) The prevalence and symptoms of premenstrual syndrome under examination. J Biosci Med 3: 1-8.View
Steiner M, Peer M, Palova E (2011) The premenstrual symptoms screening tool revised for adolescents (PSST-A): prevalence of severe PMS and premenstrual dysphoric disorder in adolescents. Arch Womens Ment Health 14: 77–81.View
Kring AM, Johnson SL, Davison GC, Neale JM (2014) Abnormal Psychology (12th ed. DSM-5 update; International student version). Hoboken, N J: John Wiley & Sons.View
Lee YH (2012) Pilot studies with the Chinese Version of Kentucky Inventory of mindfulness skills and the effect of mindfulness on emotion regulation in borderline disorder. Taipei City: National Science Committee.
Baer RA, Smith GT, Hopkins J, Krietemeyer J, Toney L, et al. (2006) Using self report assessment methods to explore facets of mindfulness. Assessment 13: 27–45.View
Brown KW, Ryan RM (2003) The benefits of being present: Mindfulness and its role in psychological well-being. J Pers Soc Psychol 84: 822-848.View
Guo Y-J, Wang SC, Veronica J (2011) College students stress under current economic downturn. College Student J 45: 536- 543.View
Schmelzer K, Ditzen B, Weise C, Andersson G., Hiller W, et al. (2015) Clinical Profiles of Premenstrual Experiences Among Women Having Premenstrual Syndrome (PMS): Affective Changes Predominate and Relate to Social and Occupational Functioning. Health Care Women In 36: 1104–1123. View
Srd G. BB (1988) Pre-menstrual syndrome and diet. J Nutr Environ Med 8: 65-75. View
Singh R, Sharma R, Rajani H (2015) Impact of stress on menstrual cycle: A comparison. Saudi J Health Sci 4: 115-119.View
Nisar N, Zehra N, Haider G, Munir AA, Sohoo NA, et al. (2008) Frequency, intensity and impact of premenstrual syndrome in medical students. J College Physicians Surgeons Pak 18: 481- 484.View
Rapkin AJ, Mikacich JA (2013) Premenstrual dysphoric disorder and severe premenstrual syndrome in adolescents diagnosis and pharmacological treatment. Pediatr Drugs 15: 191–202.View
Roberts KC, Danoff-Burg S (2010) Mindfulness and health behaviors: Is paying attention good for you? J Am Coll Health 59: 165-173.View
Perkonigg A, Yonkers K, Pfiste H, Lieb R, Wittchen HU , et al. (2004) Risk factors for premenstrual dysphoric disorder in a community sample of young women: the role of traumatic events and posttraumatic stress disorder. J Clin Psychiat 65: 1314–1322.View
Bodenlos JS, Noonan M, Wells SY (2013) Mindfulness and alcohol problems in college students: The mediating effects of stress. J Am Coll Health 61: 371-378.View