
Effect of Chlorogenic Acids on Cognitive Function in Mild Cognitive Impairment: A Randomized Controlled Crossover Trial
Abstract
Background:
Mild cognitive impairment (MCI) is a global-scale issue, due in large part to the rapidly growing elderly population. The main polyphenol contained in coffee beans, chlorogenic acid (CGA), improves attention in healthy individuals. The utility of CGAs for treating MCI, however, has not been evaluated.
Objective:
To determine the effects of continuous CGA intake on cognitive function, especially attention, in patients diagnosed with MCI.
Methods:
The study was a randomized controlled crossover trial including 34 patients with MCI. Participants were randomly divided into two groups: Those who first ingested a placebo beverage and those who first ingested an active beverage containing CGAs (553.6 mg/bottle) twice daily for 12 weeks. After a 4-week washout period, the subjects ingested the other beverage (i.e., placebo or active beverage) in the same manner. Endpoint measures included scores on the Japanese version of the Mini-Mental State Examination (MMSE), the Japanese version of the Alzheimer’s Disease Assessment Scale-cognitive component (ADAS-cog) testing overall cognitive function, and the Japanese version of the Trail Making Test (TMT-A, TMT-B) testing attention, along with the results of blood tests to evaluate safety.
Results:
In the TMT-B test, participants had a significantly reduced number of errors while ingesting the CGA beverage as compared with the placebo beverage (p < 0.05), although there was no difference in test completion time. Scores in the MMSE, ADAS-cog, and TMT-A did not differ significantly between conditions.
Conclusion:
Continuous intake of CGAs appears to improve attention and executive function among cognitive functions in MCI.
INTRODUCTION
Improving and maintaining cognitive functions are important goals for patients with mild cognitive impairment (MCI), in order to delay the transition to dementia. Memory impairment is the main symptom of dementia, and impairment in attention and executive ability underlie the deterioration of memory [1]. Therefore, evaluating attention, in addition to memory function, is important in patients with MCI.
Coffee intake has protective effects against some diseases, including type 2 diabetes mellitus, Alzheimer’s disease, and Parkinson’s disease [2–4]. Some of these health benefits are attributed to the chlorogenic acids (CGAs) in coffee beans [5, 6]. A recent study reported that consuming CGAs (300–600 mg/day) improved postprandial lipid metabolism, insulin resistance, vascular endothelial function, and sleep in healthy humans [7–10]. CGAs and their metabolites also exhibit neuroprotective effects and inhibit amyloid-β aggregation [11–13]. In a mouse model of scopolamine-induced cognitive impairment, administration of 5-CQA, the main component of CGAs, suppressed hippocampal acetylcholinesterase activity and reduced oxidative stress [14]. Thus, CGAs are expected to be effective for improving cognitive function in humans.
We recently reported that a continuous intake of CGA (300 mg/day) for 4–6 months improved cognitive function, especially attention and executive function, in middle-aged and elderly populations [15, 16]. This study conducted a randomized controlled trial to clarify the potential for patients with MCI.
MATERIALS AND METHODS
Participants
Participants were recruited from MCI patients (men and women, 60–84 years of age) who attended the Memory Clinic Ochanomizu (Tokyo, Japan). They were screened to confirm that they had not progressed to dementia and to obtain initial data. Eligibility criteria for participants at screening were as follows: MCI, defined as stage 0.5 on the Japanese version of the Clinical Dementia Rating (CDR) [17]; more than 23 points on the Japanese version of the Mini-Mental State Examination (MMSE) [18]; no history of treatment for a serious illness (cancer, myocardial infarction, and stroke) within the previous 5 years; no dementia drugs taken; less than 5 points on the Japanese version of the Geriatric Depression Scaler–Short Version (GDS) [19]; and the ability to understand the study and consent to participation. Patients with food allergies, receiving psychotropic drugs, or judged to be inappropriate for the study by the principal investigator were excluded. Participants were recruited by doctors.
Study protocol
The study protocol was reviewed and approved by the Human Ethics Committee of Kao Corporation (Sumida-ku, Tokyo, Japan [approval date, September 5, 2017]) and Shinagawa Season Terrace Health Care Clinic (Minato-ku, Tokyo, Japan [approval date, September 15, 2017]), and registered in the UMIN Clinical Trial Registry before enrollment of the first participant (UMIN-CTR; URL: http://www.umin.ac.jp/ctr/, ID:UMIN000029163). All participants provided written informed consent before participation in the study. The study was conducted under the supervision of the principal investigator in accordance with the principles of the Declaration of Helsinki. Activities related to the implementation of this study were managed by the KSO Corporation (Tokyo, Japan) and conducted at the Memory Clinic Ochanomizu from September 2017 through to October 2018.
Test beverage and production
In order to clarify the potential of patients with MCI, this study was designed to continue with an intake of 1 g/day, the highest dietary dose of CGA [20]. The test beverages were specially prepared for the study and included an active beverage that contained 553.6 mg of CGAs in 100 ml of water and a placebo beverage in an identical sealed aluminum bottle that contained no CGAs; both beverages had the same volume and taste, and contained fewer than 5 kcal. The test beverage was taken twice a day.
CGAs were extracted from Coffea canephora green coffee beans by a hot water extraction method and decaffeinated using activated carbon; dry powder was then produced by spray drying [21]. As caffeine impairs sleep function [22], the caffeine level of the beverage was adjusted to less than 1 mg/100 ml. The CGAs comprised three quinic acid derivatives: 68.9% caffeoylquinic acids, 13.2% feruloylquinic acids, and 17.9% dicaffeoylquinic acids. A cup of coffee (200 ml) contains 70r–200 mg of CGAs, and CGAs are also found in fruits and vegetables, and are thus consumed on a daily basis [20]. Therefore, the daily intake of CGA in this study was equivalent to 5 or 6 cups of coffee.
Study design
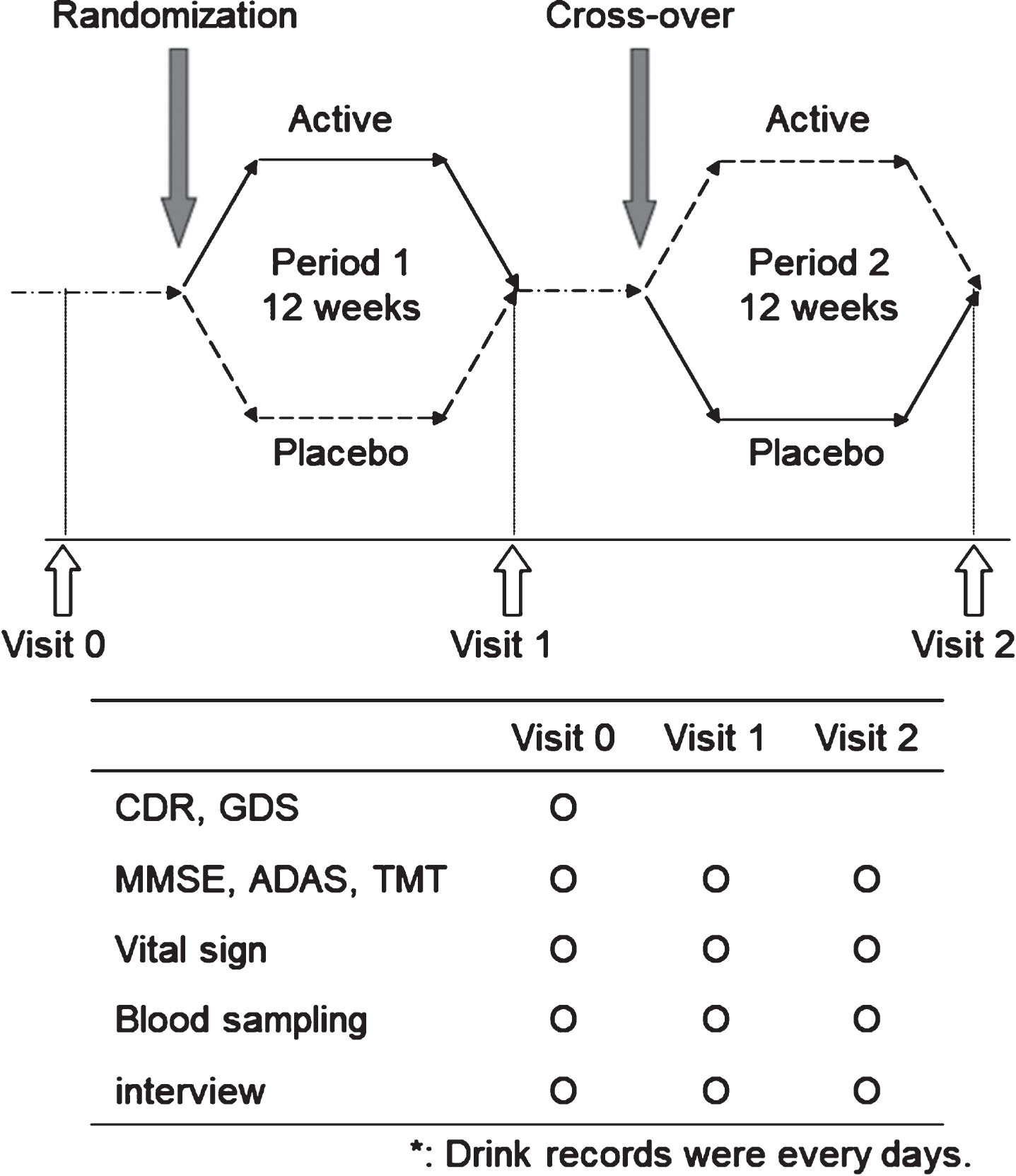
This was a randomized, double-blind, placebo-controlled crossover trial (Fig. 1). The study comprised two 12-week intake periods, with a 4-week washout period between them (total of 28 weeks). The cognitive function tests and medical checkups were performed at the study site at the end of each intake period (Visit 1 and Visit 2). Before the first intake (Visit 0), the principal or sub-investigator administered CDR, GDS, and cognitive function tests; measured vital signs; and conducted blood tests for screening. The principal investigator selected the participants to be enrolled based on the eligibility and exclusion criteria. The selected participants were assigned to one of the two groups (Sequence A and Sequence B) by stratified block randomization. The stratification factors were age, MMSE scores, and Alzheimer’s Disease Assessment Scale-cognitive component (ADAS-cog) scores [23]. Subjects ingested the active or placebo beverage for 12 weeks. After a washout period of at least 4 weeks, they ingested the other beverage (i.e., placebo or active beverage) for 12 weeks. The first 12-week intake period was referred to as Period 1, and the second 12-week intake period was referred to as Period 2. The allocation table was sealed by the person responsible for group allocation and stored in a sealed container until breaking of the blinding. The subjects consumed two test beverages per day (active beverage, CGAs 553.6 mg/100 mL×2; placebo beverage, CGAs 0 mg/100 mL×2) during the period after dinner to 1 h before bedtime. In order to maintain the compliance of participants: 1) doctors and staff were advised to encourage participants to drink test beverages during outpatient visits, 2) the participants recorded their daily physical condition and test beverage consumption, and 3) the required amount of test beverages was provided every 2 weeks.
Fig.1
Trial design. CDR, Japanese version of Clinical Dementia Rating; GDS, Japanese version of Geriatric Depression Scale – Short Version; MMSE, Japanese version of Mini-Mental State Examination; ADAS, Japanese version of Alzheimer’s Disease Assessment Scale-cognitive component; TMT, Japanese version of the Trail Making Test.
Cognitive function assessments
This study was conducted in patients who had already been diagnosed with MCI due to a decline in cognitive function and who were attending clinic. A simple test was chosen to ensure a cognitive test for MCI patients. Cognitive function tests, the MMSE, ADAS-cog, and Trail Making Test (TMT-A and -B), were administered at the beginning (Visit 0) and end of each period (Visit 1 and 2). The TMT is an appropriate evaluation for detecting differences between healthy individuals and MCI patients [24], and was used to assess psychological attention [25, 26] or executive function [27].
The Japanese version of the TMT-B contains 25 circled numbers and letters (13 numbers from 1 to 13, and 12 Japanese hiragana characters). For both tests, when a participant made a mistake in the order of connecting the numbers during the test, the sub-investigator immediately asked the participant to correct the error and continue. The time required to connect the lines and the number of errors in both tests were recorded. If subjects could not complete the tests within 5 min, the tests were stopped, and the last number or letter reached was recorded. The TMTs were administered after participants performed a practice exercise with a 10-number/character version.
Blood chemistry and interview
Blood samples were collected during screening and at the end of each treatment period. Blood count and chemistry parameters were measured by the LSI Medience Corporation (Tokyo, Japan). The blood CGA levels were measured by Sumika Chemical Analysis Service (Osaka, Japan) according to the reported method [28]. A physician interview was conducted to evaluate each subject’s subjective symptoms and objective findings.
Safety assessments
Safety evaluations included all recorded adverse events (AEs), blood tests at visits (screening and at the end of the treatment periods), vital signs, and interview. AEs were any undesirable or unintended medical signs that occurred in participants during the study beverage intake period.
Statistical analysis
The analysis was repeated using the per-protocol set (PPS), which was defined as those participants who did not drop out during the test beverage intake period and had all cognitive tests after treatment and did not receive any anti-dementia drugs. The full analysis set (FAS), defined as all randomized participants that received study treatment and had at least one cognitive test after treatment and safety test values, were evaluated. The efficacy for cognitive functions in patients with MCI was compared between conditions using the Wilcoxon signed rank test. Blood CGA levels were compared between the baseline and end of the active condition using a paired t-test. Safety data were compared between conditions using a paired t-test. AEs were recorded in all randomized participants, and the incidence of AEs was compared between conditions using Fisher’s exact test. Missing values were not replaced by other values to conduct the analysis. The sample size was determined to be 20 per group on the basis of a previous study in healthy subjects [16]. The significance level for all tests was set at 5%. Statistical data are expressed as mean±standard deviation (SD). SPSS version 24 (SPSS Japan Inc., Tokyo) was used for statistical analysis.
RESULTS
Participants and initial characteristics
Thirty-four subjects agreed to participate in this study and underwent screening; all were judged to be eligible and were enrolled. The flow of participants in this study is shown in Fig. 2. The study was started after the participants were allocated to either Sequence A or Sequence B. During Period 1, three subjects (placebo beverage) withdrew from the study after it began. The reasons for withdrawal included AEs (n = 2) and personal reasons (n = 1). During Period 2, two subjects (placebo beverage [n = 1] and active beverage [n = 1]) withdrew from the study due to AEs. A total of 29 subjects (Sequence A, 13 subjects; Sequence B, 16 subjects) completed the study. A total of 31 participants, excluding three who lacked all test values after allocation, were analyzed as the FAS. Of the 29 participants who completed the study, one was determined to be taking a dementia drug listed in the exclusion criteria and was excluded. Therefore, 28 participants were analyzed as the PPS. The initial background data of the 34 study participants are summarized in Table 1, and treatment compliance is shown in Supplementary Table 1. The initial background characteristics of the PPS (n = 28) and six subjects who dropped out or were excluded from the analysis are shown in Supplementary Table 2, and there were no significant differences in the initial cognitive function values. Therefore, analysis was performed on the PPS. Over 80% of the test beverages were ingested during the study period.
Fig.2
Flow diagram.
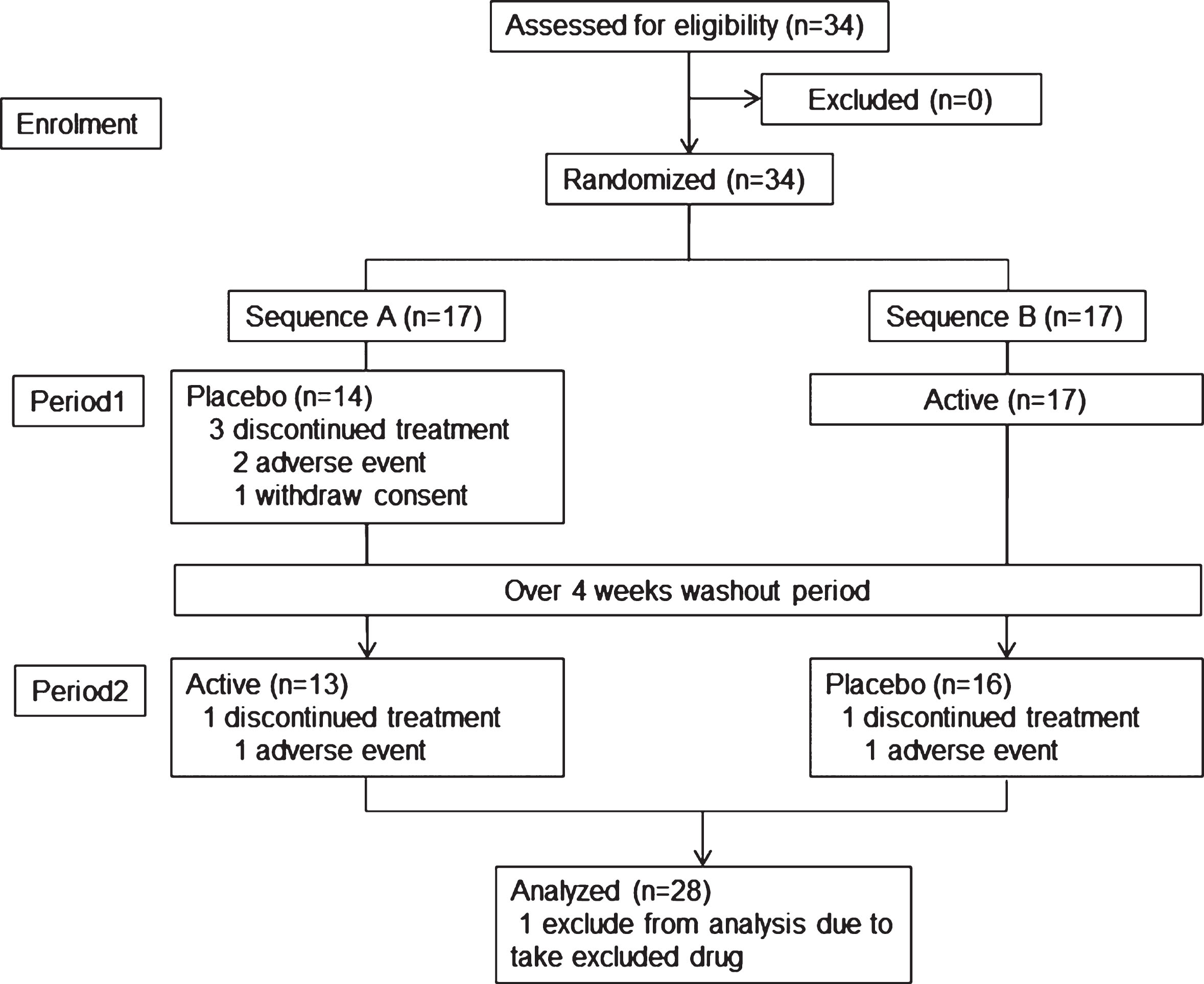
Table 1
Characteristics of the participants
| Mean±SD | |
| Number | 34 (Female 19) |
| Age (y) | 73.7±6.0 |
| Education (y) | 13.8±2.4 |
| Height (cm) | 157.3±8.7 |
| Body weight (kg) | 56.6±9.6 |
| BMI (kg/m2) | 22.8±2.9 |
| SBP (mmHg) | 138.4±14.1 |
| DBP (mmHg) | 76.2±8.8 |
| GDS | 1.7±1.4 |
| MMSE | 26.9±2.8 |
| ADAS-cog | 5.3±3.6 |
| TMT-A | |
| Time (s) | 57.4±29.8 |
| Errors | 0.0±0.2 |
| TMT-B | |
| Time (s) | 147.6±74.7 |
| Errors | 1.4±1.9 |
BMI, body mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure; GDS, Japanese version of Geriatric Depression Scale – Short Version; MMSE, Japanese version of Mini-Mental State Examination; ADAS-cog, Japanese version of Alzheimer’s Disease Assessment Scale-cognitive component; TMT-A, Japanese version of the Trail Making Test A; TMT-B, Japanese version of the Trail Making Test B.
Cognitive function assessment
The baseline characteristics of the participants are shown in Table 1. Cognitive test results after intervention with the test beverages are shown in Table 2. A 12-week period of continuous intake of the test beverage significantly reduced the number of TMT-B errors in the active beverage condition as compared with the placebo beverage condition (p < 0.05). No significant change was observed between conditions in the times taken to complete the MMSE, ADAS-cog, and TMT. All cognitive tests had no significant carryover effect in Period 1 and Period 2.
Table 2
The scores of cognitive tests
| Placebo | Active | p | |
| MMSE | 27.7±2.3 | 27.5±3.0 | 0.765 |
| ADAS-cog | 4.4±3.6 | 4.4±3.7 | 0.866 |
| TMT-A | |||
| Time (s) | 51.4±21.2 | 51.7±26.3 | 0.996 |
| Error | 0.0±0.0 | 0.2±0.5 | 0.063 |
| TMT-B | |||
| Time (s) | 124.5±53.6 | 121.4±62.0 | 0.657 |
| Error | 1.3±2.5 | 0.5±0.7 | 0.018 |
Values are expressed as the mean±SD (N = 28). MMSE, Japanese version of Mini-Mental State Examination; ADAS-cog, Japanese version of Alzheimer’s Disease Assessment Scale-cognitive component; TMT-A, Japanese version of the Trail Making Test A; TMT-B, Japanese version of the Trail Making Test B. The p-value represents the significance level of the difference between the placebo and active beverage conditions (Wilcoxon-signed-rank test).
CGA in the blood
Transition of CGA, which was the active ingredient in the active beverage, to the blood was 7.9±14.5 ng/ml before the start of the test, and 9.4±18.1 ng/ml at the end of the active condition; the difference was not significant (p = 0.585). The details of blood CGA levels are shown in Supplementary Table 3. In addition, there was no significant correlation between the change in blood CGA levels and the number of TMT-B errors before and after intake of the active beverage (R = 0.011, p = 0.571).
Safety assessment
Data regarding weight and blood pressure are summarized in Table 3. Systolic blood pressure was significantly reduced during the 12-week period of continuous intake of the active test beverage condition as compared with the placebo beverage (p < 0.05). Blood test values are shown in Table 4. No significant changes were observed in any items between the conditions. Thirty-one AEs were observed in the active beverage condition and 23 AEs were observed in the placebo beverage condition during the test-beverage intake periods. However, the difference in the number of AEs between the two conditions was not significant. As shown in Supplementary Table 4, there was no significant difference in the incidence of AEs per event between the two conditions, and the investigator judged that there was no relationship between the AEs and the test beverages.
Table 3
Change in weight, blood pressure
| Placebo | Active | p | |
| Body weight (kg) | 57.1±9.7 | 57.0±9.7 | 0.674 |
| BMI (kg/m2) | 22.8±3.0 | 22.8±3.0 | 0.691 |
| SBP (mmHg) | 139.6±16.9 | 134.9±14.7 | 0.036 |
| DBP (mmHg) | 76.2±8.8 | 74.3±8.3 | 0.380 |
Values are expressed as the mean±SD (N = 31). BMI, body mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure. The p-value represents the significance level of the difference between the placebo and active beverage conditions (paired t-test).
Table 4
Change in blood parameters
| Placebo | Active | p | |
| White blood cell (/μL) | 5650.0±1393.5 | 5466.7±1429.8 | 0.212 |
| Red blood cell (10∧4/μL) | 453.8±38.0 | 447.8±44.5 | 0.578 |
| Hemoglobin (g/dL) | 14.1±1.4 | 14.0±1.4 | 0.864 |
| Hematocrit (%) | 43.7±3.4 | 43.5±4.1 | 0.845 |
| Platelet (10∧4/μL) | 22.0±4.6 | 22.4±5.1 | 0.096 |
| Triglyceride (mg/dL) | 152.2±109.6 | 129.0±62.5 | 0.166 |
| Total-cholesterol (mg/dL) | 204.0±35.1 | 201.5±38.9 | 0.722 |
| LDL-cholesterol (mg/dL) | 109.3±29.2 | 110.1±33.3 | 0.787 |
| HDL-cholesterol (mg/dL) | 67.8±19.9 | 67.8±19.9 | 0.931 |
| AST(IU/L) | 24.9±7.1 | 25.7±10.0 | 0.476 |
| ALT(IU/L) | 19.7±7.7 | 21.0±10.1 | 0.138 |
| ALP (IU/L) | 212.7±52.4 | 215.9±54.7 | 0.217 |
| γ-GTP(IU/L) | 31.7±22.3 | 34.7±32.4 | 0.253 |
| CK (CPK) (IU/L) | 149.3±157.2 | 113.1±51.5 | 0.124 |
| Creatinine (mg/dL) | 0.80±0.21 | 0.81±0.22 | 0.983 |
| Uric acid (mg/dL) | 5.7±1.5 | 5.6±1.3 | 0.491 |
| Blood sugar (mg/dL) | 105.6±18.7 | 107.1±33.0 | 0.933 |
| CRP (mg/dL) | 0.13±0.31 | 0.17±0.52 | 0.637 |
Values are expressed as the mean±SD (N = 31). LDL-cholesterol, low-density lipoprotein cholesterol; HDL-cholesterol, high-density lipoprotein cholesterol; AST, aspartate aminotransferase; ALT, alanine aminotransferase; ALP, alkaline phosphatase; γ-GTP, gamma-glutamyltransferase; CK, creatine phosphokinase; CRP, C-reactive protein. The p-value represents the significance level of the difference between the placebo and active beverage conditions (paired t-test).
DISCUSSION
To our knowledge, this is the first report showing that continuous intake of a CGA beverage (1107.2 mg/day) significantly reduces TMT-B errors in MCI patients. In a previous study investigating healthy individuals, we similarly reported that CGAs improved an indicator related to attention [15, 16]. In the first trial of patients with MCI, we observed improvements in the TMT, an indicator of attention and executive function, in the CGA beverage condition [27]. The TMT measures attention, execution speed, and cognitive flexibility. The TMT comprises two tests, TMT-A and TMT-B. The TMT-A is an indicator of perceptual tracking and execution speed and is used to evaluate visual and motor search behavior. The TMT-B is an indicator of the ability to allocate attention and suppress or switch responses [29]. Although CGAs did not affect the TMT-A, improvement in the TMT-B was observed, suggesting that the ability to allocate attention was enhanced. Furthermore, although there was no difference in the test achievement time, there was a significant difference in the number of errors in the TMT-B, suggesting that CGA enhanced attention maintenance and attention levels. Attention impairment affects memory, such as in MCI patients for whom daily activities are apparently non-problematic, but for whom forgetfulness worsens to a more advanced age level [1]. Thus, these findings suggest that CGA, which may improve attention and executive functioning among cognitive functions, may be useful for MCI patients.
In this study, the blood CGA concentration did not significantly increase after a continuous intake for 3 months of the active beverage condition, indicating that CGAs were not accumulated in the body. In a previous report [30], CGAs (176r–704 mg/d) were metabolized within approximately 8 h after ingestion and were not detected in the blood. On this basis, it could be considered that even a large amount of CGAs (1100 mg/d) are mostly metabolized in a short time. Also, the blood CGA concentration did not significantly correlate with the number of TMT-B errors. Therefore, it is unlikely that the effect of CGA on cognitive function is related to CGA levels in the blood. We previously reported that a continuous intake of CGAs reduced blood pressure [31] by improving vascular endothelial function, reducing mRNA levels of NADPH oxidase, a reactive oxygen species [32]. Improving vascular endothelium function is also expected to affect the cerebrovascular system. Attention and executive functions are strongly related to cerebral circulation. Part of the action of CGA may be related to the vascular function improvement effect. In addition, CGA is reported to inhibit acetylcholinesterase and have antioxidant activity in the hippocampus [14]. Furthermore, a CGA metabolite is reported to have nerve growth activity [12]. Thus, cognitive function could be improved by a combination of the various effects of CGAs.
CGAs significantly decreased systolic blood pressure, a safety endpoint, when compared with placebo. Problematic symptoms related to a decrease in blood pressure were not observed and the decrease in blood pressure was not sufficient enough to require an adjustment in the dose of antihypertensive drugs. Our findings are consistent with the fact that CGAs have an antihypertensive effect [33, 34]. The antihypertensive effect of CGAs is due to improvements in endothelial function, and it is unlikely that the blood pressure would be excessively decreased. Thus, CGAs could safely contribute to improving cognitive functions. Considering that hypertension is a risk factor for dementia and impaired cognitive function in the elderly [35], a continuous intake of CGAs would be expected to improve cognitive functions, not only in healthy individuals, but also in individuals with MCI. Therefore, CGAs may have the potential to delay the onset of dementia.
In terms of safety, AEs occurred in 17 subjects in both the CGA-containing beverage and placebo beverage conditions during the 12-week intake period, corresponding to approximately 50% of the study participants. Interviews conducted by the investigator, however, confirmed that none of the AEs were attributable to the test beverages, suggesting that CGA-containing beverages can be safely ingested by MCI patients.
This study has some limitations. First, the participants of this study were individuals with MCI seen at a single memory clinic. However, the participants were from various parts of a large city, Tokyo. Second, although the daily amount of CGA ingested in this study was high, equivalent to that of 5r–6 cups of coffee ( 1000 mg/d), ingesting the test beverage for 12 weeks did not increase CGA blood concentration. This finding suggests that CGA is a metabolizable substance, even at relatively large amounts. Therefore, it is difficult to conclude that the blood CGA concentration is directly associated with the effect of CGAs on cognitive functions. The effects of CGAs on cognitive function requires further elucidation. This study is a 3-month crossover trial, and in the future, it would be important to conduct a long-term parallel trial to verify the effects of CGA. Despite these limitations, our results indicate that a continuous intake of CGAs improves attention and executive function among cognitive functions in patients with MCI.
ACKNOWLEDGMENTS
The authors thank all the participants for their dedication and cooperation. We appreciate Mr. Mutsuki Kikawada of the Memory Clinic Ochanomizu for technical advice. We also thank Mr. Tatsuya Kusaura and Mr. Naoki Oozato of Kao Corporation for supplying the test beverage.
This research was funded by Kao Corporation.
Authors’ disclosures available online (https://www.j-alz.com/manuscript-disclosures/19-0757r1).
SUPPLEMENTARY MATERIAL
[1] The supplementary material is available in the electronic version of this article: https://dx.doi.org/10.3233/JAD-190757.
REFERENCES
[1] | Silveri MC , Reali G , Jenner C , Puopolo M ((2007) ) Attention and memory in the preclinical stage of dementia. J Geriatr Psychiatry Neurol 20: , 67–75. |
[2] | van Dam RM , Hu FB ((2005) ) Coffee consumption and risk of type 2 diabetes. JAMA 294: , 97–104. |
[3] | van Gelder BM , Buijsse B , Tijhuis M , Kalmijn S , Giampaoli S , Nissinen A , Kromhout D ((2007) ) Coffee consumption is inversely associated with cognitive decline in elderly European men: The FINE Study. Eur J Clin Nutr 61: , 226–232. |
[4] | Hernan MA , Takkouche B , Caamano-Isorna F , Gestal-Otero JJ ((2002) ) A meta-analysis of coffee drinking, cigarette smoking, and the risk of Parkinson’s disease. Ann Neurol 52: , 276–284. |
[5] | Ranheim T , Halvorsen B ((2005) ) Coffee consumption and human health – beneficial or detrimental? – Mechanisms for effects of coffee consumption on different risk factors for cardiovascular disease and type 2 diabetes mellitus. Mol Nutr Food Res 49: , 274–284. |
[6] | Butt MS , Sultan MT ((2011) ) Coffee and its consumption: Benefits and risk. Crit Rev Food Sci Nutr 51: , 363–373. |
[7] | Soga S , Ota N , Shimotoyodome A ((2013) ) Stimulation of postprandial fat utilization in healthy humans by daily consumption of chlorogenic acids. Biosci Biotechnol Biochem 77: , 1633–1636. |
[8] | Lecoultre V , Carrel G , Egli L , Binnert C , Boss A , MacMillan EL , Kreis R , Boesch C , Darimont C , Tappy L ((2014) ) Coffee consumption attenuates short-term fructose-induced liver insulin resistance in healthy men. Am J Clin Nutr 99: , 268–275. |
[9] | Ochiai R , Sugiura Y , Otsuka K , Katsuragi Y , Hashiguchi T ((2015) ) Coffee bean polyphenols ameliorate postprandial endothelial dysfunction in healthy male adults. Int J Food Sci Nutr 66: , 350–354. |
[10] | Ochiai R , Tomonobu K , Ikushima I ((2018) ) Effect of chlorogenic acids on fatigue and sleep in healthy males: A randomized, double-blind, placebo-controlled, crossover study. Food Sci Nutr 6: , 2530–2536. |
[11] | Heitman E , Ingram DK ((2017) ) Cognitive and neuroprotective effects of chlorogenic acid. Nutr Neurosci 20: , 32–39. |
[12] | Ito H , Sun XL , Watanabe M , Okamoto M , Hatano T ((2008) ) Chlorogenic acid and its metabolite m-coumaric acid evoke neurite outgrowth in hippocampal neuronal cells. Biosci Biotech Biochem 72: , 885–888. |
[13] | Kurisu M , Miyamae Y , Murakami K , Han J , Isoda H , Irie K , Shigemori H ((2013) ) Inhibition of amyloid beta aggregation by acteoside, a phenylethanoid glycoside. Biosci Biotech Biochem 77: , 1329–1332. |
[14] | Kwon SH , Lee HK , Kim JA , Hong SI , Kim HC , Jo TH , Park YI , Lee CK , Kim YB , Lee SY , Jang CG ((2010) ) neuroprotective effects of chlorogenic acid on scopolamine-induced amnesia via anti-acetylcholinesterase and anti-oxidative activities in mice. Eur J Pharmacol 649: , 210–217. |
[15] | Kato M , Ochiai R , Kozuma K , Sato H , Katsuragi Y ((2018) ) Effect of chlorogenic acid intake on cognitive function in the elderly: A pilot study. eCAM 2018: , 8608497. |
[16] | Saitou K , Ochiai R , Kozuma K , Sato H , Koikeda T , Osaki N , Katsuragi Y ((2018) ) Effect of chlorogenic acids on cognitive function: A randomized double-blind placebo-controlled trial. Nutrients 10: , 1337. |
[17] | Morris JC ((1993) ) The Clinical Dementia Rating (CDR): Current version and scoring rules. Neurology 43: , 2412–2414. |
[18] | Johnson-Kozlow M , Silverstein D , Barrett-Connor E , Morten D ((2002) ) Coffee consumption and cognitive function among older adults. Am J Epidemiol 156: , 842–850. |
[19] | Yesavage JA , Brink TL ((1982) ) Development and validation of a geriatric depression screening scale: A preliminary report. J Psychiatr Res 17: , 37–49. |
[20] | Clifford MN ((1999) ) Chlorogenic acids and other cinnamates nature, occurrence and dietary burden. J Sci Food Agric 79: , 362–372. |
[21] | Ochiai R , Sugiura Y , Shioya Y , Otsuka K , Katsuragi Y , Hashimoto T ((2014) ) Coffee polyphenols improve peripheral endothelial function after glucose loading in healthy male adults. Nutr Res 34: , 155–159. |
[22] | Clark I , Landolt HP ((2017) ) Coffee, caffeine, and sleep: A systematic review of epidemiological studies and randomized controlled trials. Sleep Med Rev 31: , 70–78. |
[23] | Mohs RC , Rosen WG , Davis KL ((1983) ) The Alzheimer’s disease assessment scale: An instrument for assessing treatment efficacy. Psychopharmacol Bull 19: , 448–450. |
[24] | Ashendorf L , Jefferson AL , O’Connor MK , Chaisson C , Green RC , Stern RA ((2008) ) Trail making test errors in normal aging, mild cognitive impairment, and dementia. Arch Clin Neuropsychol 23: , 129–137. |
[25] | Staff, Personnel Research Section, Classification and Replacement Branch, AGO ((1944) ) The new Army individual test of general mental ability. Psychol Bull 41: , 532–538. |
[26] | Rabin LA , Barr WB , Burton LA ((2005) ) Assessment practices of clinical neuropsychologists in the United States and Canada: A survey of INS, NAN, and APA Division 40 members. Arch Clin Neuropsychol 20: , 33–65. |
[27] | Salthouse TA ((2011) ) What cognitive abilities are involved in trail-making performance? Intelligence 39: , 222–232. |
[28] | Matsui Y , Nakamura S , Kondou N , Takasu Y , Ochiai R , Masukawa Y ((2007) ) Liquid chromatography-electrospray ionization-tandem mass spectrometry for simultaneous analysis of chlorogenic acids and their metabolites in human plasma. J Chromatography B 858: , 96–105. |
[29] | Strauss E , Sherman EMS , Spreen O ((2006) ) A compendium of neuropsychological tests: Administration, norms, and commentary (3rd ed.), Oxford University Press, New York, pp. 655–672. |
[30] | Renouf M , Marmet C , Giuffrida F , Lepage M , Barron D , Beaumont M , Williamson G , Dionisi F ((2014) ) Dose-response plasma appearance of coffee chlorogenic and phenolic acids in adults. Mol Nutr Food Res 58: , 301–309. |
[31] | Ochiai R , Chikama A , Kataoka K , Tokimitsu I , Maekawa Y , Ohishi M , Rakugi H , Mikami H ((2009) ) Effects of hydroxyhydroquinone-reduced coffee on vasoreactivity and blood pressure. Hypertens Res 32: , 969–974. |
[32] | Suzuki A , Yamamoto N , Jokura H , Yamamoto M , Fujii A , Tokimitsu I , Saito I ((2006) ) Chlorogenic acid attenuates hypertension and improves endothelial function in spontaneously hypertensive rats. J Hypertens 24: , 1065–1073. |
[33] | Watanabe T , Arai Y , Mitsui Y , Kusaura T , Okawa W , Kajihara Y , Saito I ((2006) ) The blood pressure-lowering effect and safety of chlorogenic acid from green coffee bean extract in essential hypertension. Clin Exp Hypertens 28: , 439–449. |
[34] | Nagao T , Ochiai R , Katsuragi Y , Hayakawa Y , Kataoka K , Komikado M , Tokimitsu I , Tsuchida T ((2007) ) Hydroxyhydroquinone-reduced milk coffee decreases blood pressure in individuals with mild hypertension and high-normal blood pressure. Prog Med 27: , 2649–2664. |
[35] | Matthews F , Arthur A , Barnes LE , Bond J , Jagger C , Robinson L , Brayne C ((2013) ) A two-decade comparison of prevalence of dementia in individuals aged 65 years and older from three geographical areas of England: Results of the Cognitive Function and Ageing Study I and II. Lancet 382: , 1405–1412. |

