
More Information
Submitted: July 23, 2022 | Approved: August 18, 2022 | Published: August 19, 2022
How to cite this article: Foreste V, Pellicano M, Santini M, Bifulco G, Gallo A. Thoracic endometriosis: A case of one step multidisciplinary surgical treatment. J Clin Adv Dent. 2022; 6: 031-033.
DOI: 10.29328/journal.jcad.1001030
Copyright License: © 2022 Foreste V, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Endometriosis; Thoracic endometriosis; Catamenial pneumothorax

Thoracic endometriosis: A case of one step multidisciplinary surgical treatment
Virginia Foreste1*, Massimiliano Pellicano2, Mario Santini3, Giuseppe Bifulco1 and Alessandra Gallo1
1Department of Neuroscience, Reproductive Sciences and Dentistry, School of Medicine, University of Naples Federico II, Naples, Italy
2Department of Obstetrics and Gynecology, University of Naples Federico II, Naples, Italy
3Division of Thoracic Surgery, Università degli Studi della Campania “Luigi Vanvitelli,” Naples, Italy
*Address for Correspondence: Virginia Foreste, Department of Neuroscience, Reproductive Sciences and Dentistry, School of Medicine, University of Naples Federico II, Naples, Italy, Email: virgi.foreste@hotmail.it
We describe a case of thoracic endometriosis in a patient with a repeated episode of spontaneous pneumothorax. Investigations revealed diaphragmatic fenestrations and right-sided pleural and lung endometriosis. Considering the ultrasound evidence of pelvic endometriosis, the patient was scheduled for multidisciplinary surgical management, to treat in one step thoracic and pelvic endometriosis.
Endometriosis is a condition defined by the presence of endometrial glands and stroma outside the uterine cavity; its main location is in the female pelvis, but it can occur in several distant site such as the urinary and gastrointestinal tract [1]. Although rare, endometriosis of the thoracic cavity is the most affected extra pelvic site and in 50% - 80% of patients is associated with pelvic endometriosis [2].
Thoracic endometriosis is related to a range of clinical and radiological manifestations, such as catamenial pneumo-thorax, catamenial hemothorax, catamenial hemoptysis and pulmonary nodules. Together, they are identified as thoracic endometriosis syndrome (TES). Usually, catamenial pneumothorax is the main manifestation (80%) [3].
Although the differential diagnosis of TES is wide-ranging, features that differentiate TES from other disorders include the temporal relationship with menses, predominant right-sided symptoms, young age, presence of recurrent disease and a history of infertility [4].
According to the treatment, usually the resection of the thoracic lesions is performed at a separate time from the pelvic approach [5].
In our experience, it has been shown according to literature data, that the multidisciplinary approach is safe, feasible and cost-effective [6]. It allows the resolution of pelvic and thoracic endometriosis in a limited surgical time, with no complications, also thanks to the advantage of single anesthesia.
We describe a rare case of thoracic endometriosis diagnosticated in a 36 - year’s old woman.
The patient presented to our clinic for a routinely gynecological control referring dysmenorrhea and pelvic pain refractory to medical therapy; in her pathological anamnesis, she referred a history of repeated episodes of spontaneous pneumothorax that usually occurs within 24 - 48 hours before or after menstruation and continuous right thoracic pain during the menstrual period. Computed tomography (CT) imaging of the chest showed a right apical parieto-basal hydropneumothorax with focal thickening of the right diaphragmatic pleura.
Due to her chest symptomatology and the presence of pelvic deep infiltrating endometriosis, she was scheduled for surgery with a multidisciplinary approach to treat both thoracic and pelvic disease in a single procedure.
After the resolution of endometriosis of the pelvic compartment, with the eradication of deep infiltrating endometriosis, the upper abdomen was studied and at the inspection of the diaphragm, the surface was interested in multiple fenestrations (Figure 1). A video assisted thoracoscopy (VATS) was performed. Multiple localization of spots of endometriosis were detected on the lung (Figure 2) and on the pleura (Figure 3). A chemical talc pleurodesis was done (Figure 4) and the diaphragmatic fenestrations were repaired (Figure 5).
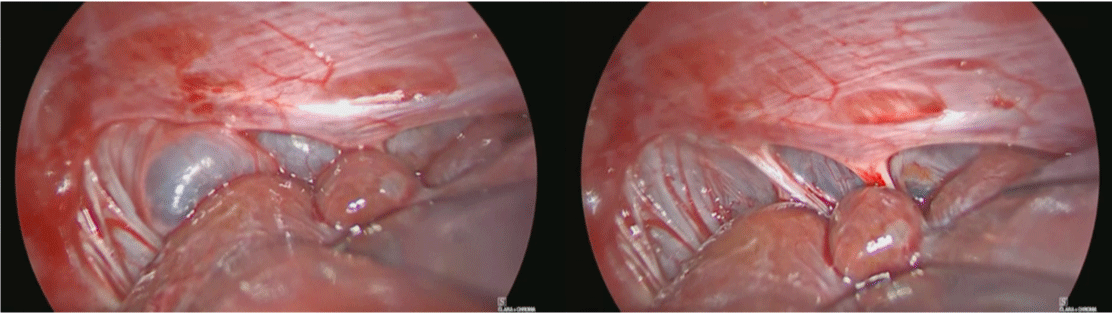
Figure 1: Retraction of the liver for diaphragm inspection. Notice the diaphragmatic fenestrations secondary to endometriosis and the lung position with insufflations-desufflations maneuvers.
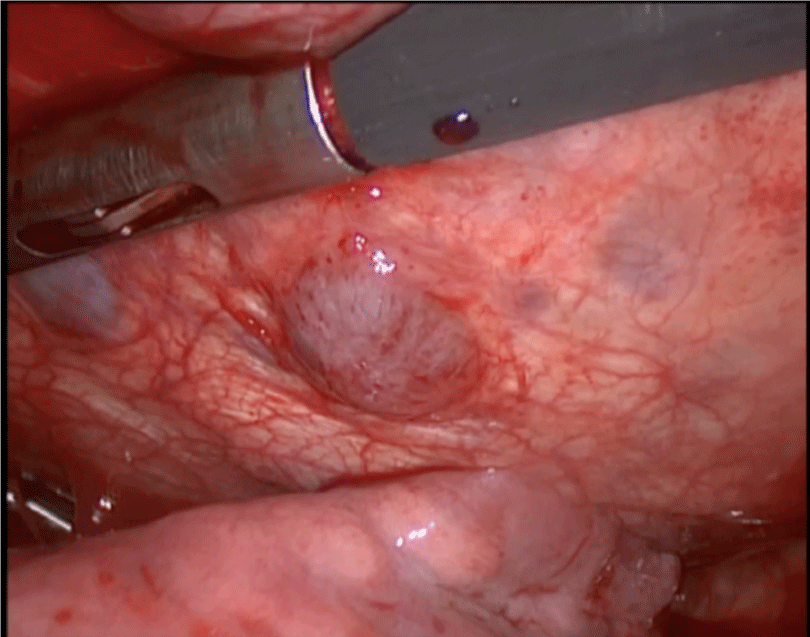
Figure 2: Blu spot of thoracic endometriosis.
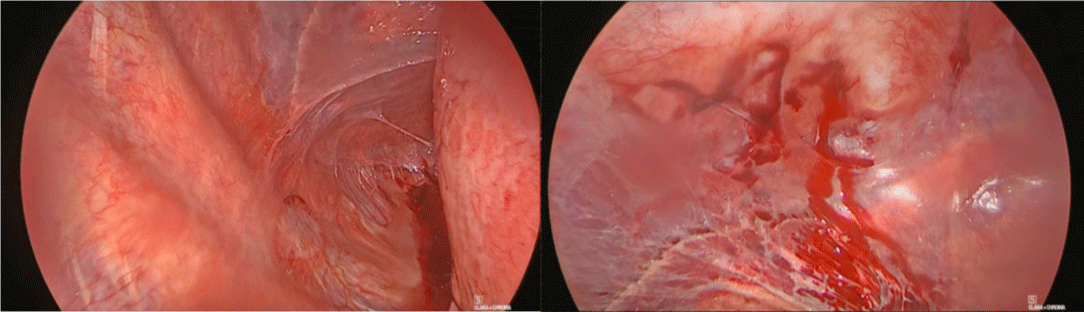
Figure 3: Pleural endometriosis.
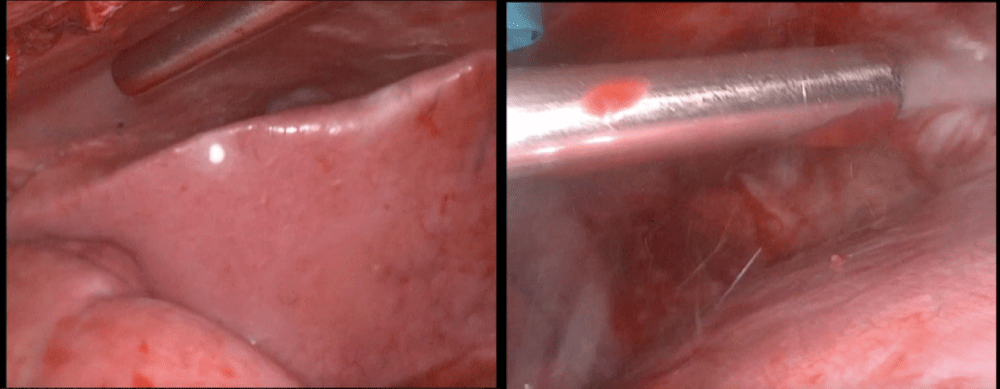
Figure 4: Talc pleurodesis.
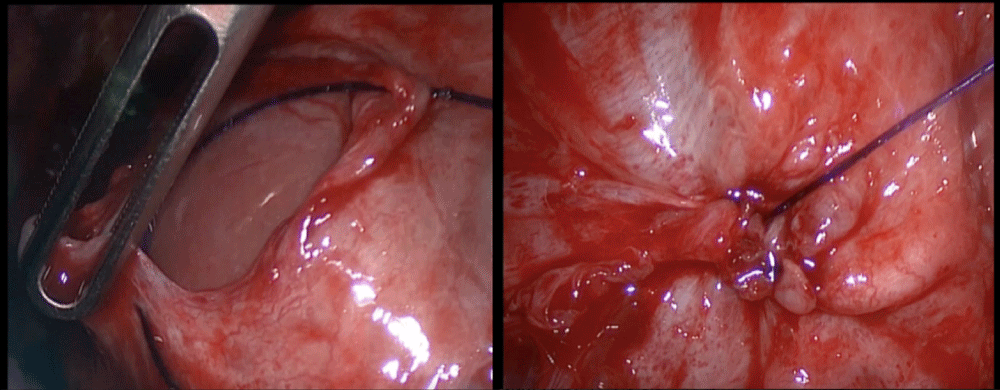
Figure 5: Repair of diaphragmatic fenestrations.
This surgical approach, combining video laparoscopy (VL) performed by a gynecologic surgeon and VATS performed by a thoracic surgeon, allowed a resolution of pelvic and thoracic endometriosis in less than 3 hours (2 hours and 45 minutes).
Adjuvant hormonal therapy with GnRH a was prescribed after the surgical treatment.
Thoracic endometriosis, defined as the presence of endometrial implants in the pleura, airways, or lung parenchyma, although rare is a condition that can be associated with severe symptoms such as catamenial pneumothorax and hemothorax [7]. Several theories have been proposed and examined for the pathogenesis of thoracic endometriosis, but the precise mechanism of development is still unclear [5]. The most reliable hypothesis is retrograde menstruation, first described by Sampson at the beginning of the last century [8], according to which endometrial cells disseminate from the uterus and tubes and accumulate in the subdiaphragmatic space, causing diaphragmatic endometriosis; then, they could also reach the peritoneal cavity, as they enter the pleural space through diaphragmatic defects. Other theories propose lymphatic or hematogenous dissemination, following the behavior of cancer metastases. The coelomic metaplasia theory would explain the evidence of thoracic endometriosis without diaphragmatic involvement; it theorizes that mesothelial cells would be capable of transforming into endometrial cells under the influence of hormonal factors. The last theory, first described in 1974 by Rossi, et al. suggests a hormonal model according to which a high prostaglandin F2 level at the menstrual period causes vasoconstriction and ischemia in the lungs [9].
The diagnosis of TES still represent a challenge and it is often delayed, due to its rarity and to the poor confidence of the gynecologist with upper abdominal surgery [10]; moreover, patients often do not correlate symptoms such as shoulder pain, chest pain, and shortness of breath to the thoracic location of endometriosis. This may also explain the higher mean age at diagnosis of TES, compared to the diagnosis of pelvic endometriosis. Nezhat, et al. in their series, found a mean age at diagnosis of thoracic endometriosis of 37.7 years, consistent with the previously reported mean age of 35 years [5] and with the age of the patient of our case; this may also be related to the longer time to development of thoracic endometrial implants. Anamnesis, radiologic examination, and histopathological confirmations are involved in the diagnosis of thoracic endometriosis. Sometimes, laparoscopic inspection is responsible for the diagnosis, when typical thoracic symptoms are lacking.
Upper abdomen ultrasound (US), chest x-ray, chest compu-ted tomography (CT) and magnetic resonance imaging (MRI) have been used for the diagnosis of thoracic endometriosis. Trans abdominal US is a valid, feasible and cost-effective instrument; in the presence of thoracic symptoms, CT is the first line method, even if it has poor specificity; it is especially useful in ruling out other pulmonary conditions. MRI is recommended for the detection of diaphragmatic endometriosis with high sensitivity [11].
VATS represent the gold standard method to confirm endometrial implants in the thorax, allowing the treatment of the lesion and biopsy with histological examination [12]. A combined approach of VATS and VL is the best diagnostic and therapeutic option when both pelvic and thoracic symptoms are present. Surgical treatment, performed with a minimally invasive technique, should be used alone or in association with medical therapy; danazol and gonadotropin-releasing hormone agonists (GnRHa) can be administered to gain the suppression of ovarian estrogen secretion. Chemical pleurodesis in the presence of hemothorax and pneumothorax is an option before major surgical procedures [13].
Since thoracic and pelvic endometriosis is often concomi-tant, in a patient with pelvic endometriosis and symptoms concerning for TES, a chest CT is required, and in case of surgical indication, a multidisciplinary surgical approach to manage both thoracic and pelvic endometriosis in a single procedure provides the most effective outcome.
- Burney RO, Giudice LC. Pathogenesis and pathophysiology of endometriosis. Fertil Steril. 2012 Sep;98(3):511-9. doi: 10.1016/j.fertnstert.2012.06.029. Epub 2012 Jul 20. PMID: 22819144; PMCID: PMC3836682.
- Chen ML, Li CY. Thoracic Endometriosis. N Engl J Med. 2021 Nov 4;385(19):e65. doi: 10.1056/NEJMicm2105508. PMID: 34731539.
- Chen C, Zhai K, Tang Y, Qu W, Zuo J, Ke X, Song Y. Thoracic endometriosis: a case report and review of the literature. Ann Palliat Med. 2021 Mar;10(3):3500-3503. doi: 10.21037/apm-21-280. PMID: 33849132.
- Andres MP, Arcoverde FVL, Souza CCC, Fernandes LFC, Abrão MS, Kho RM. Extrapelvic Endometriosis: A Systematic Review. J Minim Invasive Gynecol. 2020 Feb;27(2):373-389. doi: 10.1016/j.jmig.2019.10.004. Epub 2019 Oct 13. PMID: 31618674.
- Nezhat C, Main J, Paka C, Nezhat A, Beygui RE. Multidisciplinary treatment for thoracic and abdominopelvic endometriosis. JSLS. 2014 Jul-Sep;18(3):e2014.00312. doi: 10.4293/JSLS.2014.00312. PMID: 25392636; PMCID: PMC4154426.
- Nezhat C, Nicoll LM, Bhagan L, Huang JQ, Bosev D, Hajhosseini B, Beygui RE. Endometriosis of the diaphragm: four cases treated with a combination of laparoscopy and thoracoscopy. J Minim Invasive Gynecol. 2009 Sep-Oct;16(5):573-80. doi: 10.1016/j.jmig.2009.06.012. PMID: 19835800.
- Pankratjevaite L, Samiatina-Morkuniene D. A case report of thoracic endometriosis - A rare cause of haemothorax. Int J Surg Case Rep. 2017;33:139-142. doi: 10.1016/j.ijscr.2017.02.052. Epub 2017 Mar 4. PMID: 28315819; PMCID: PMC5358902.
- Sampson JA. The development of the implantation theory for the origin of peritoneal endometriosis. Am J Obstet Gynecol 1940; 40:549-557
- Soares T, Oliveira MA, Panisset K, Habib N, Rahman S, Klebanoff JS, Moawad GN. Diaphragmatic endometriosis and thoracic endometriosis syndrome: a review on diagnosis and treatment. Horm Mol Biol Clin Investig. 2021 Feb 18. doi: 10.1515/hmbci-2020-0066. Epub ahead of print. PMID: 34704688.
- Bobbio A, Canny E, Mansuet Lupo A, Lococo F, Legras A, Magdeleinat P, Regnard JF, Gompel A, Damotte D, Alifano M. Thoracic Endometriosis Syndrome Other Than Pneumothorax: Clinical and Pathological Findings. Ann Thorac Surg. 2017 Dec;104(6):1865-1871. doi: 10.1016/j.athoracsur.2017.06.049. Epub 2017 Oct 17. PMID: 29054304.
- Ceccaroni M, Roviglione G, Farulla A, Bertoglio P, Clarizia R, Viti A, Mautone D, Ceccarello M, Stepniewska A, Terzi AC. Minimally invasive treatment of diaphragmatic endometriosis: a 15-year single referral center's experience on 215 patients. Surg Endosc. 2021 Dec;35(12):6807-6817. doi: 10.1007/s00464-020-08186-z. Epub 2021 Jan 4. Erratum in: Surg Endosc. 2021 Jan 13;: PMID: 33398589.
- Peterzan M, Reynolds T, Dulay K, Wooldridge R. Thoracic endometriosis syndrome manifesting as atraumatic haemothorax causing difficult ventilation under general anaesthesia. BMJ Case Rep. 2012 Dec 19;2012:bcr2012007206. doi: 10.1136/bcr-2012-007206. PMID: 23257939; PMCID: PMC4543866.
- Sevinç S, Unsal S, Oztürk T, Uysal A, Samancilar O, Kaya SO, Ermete S. Thoracic endometriosis syndrome with bloody pleural effusion in a 28 year old woman. J Pak Med Assoc. 2013 Jan;63(1):114-6. PMID: 23865146.