


Isokinetics has been used in testing and rehabilitation for the last 60 years. Its most common use has been for selected musculoskeletal injuries at the knee because of the frequency of injury and ease of testing. Looking back historically, several trends can be identified regarding isokinetics, testing, and rehabilitation. Beginning in the 1960s–1970s an integrated approach combining open kinetic chain (OKC) (isolated joint exercises), closed kinetic chain (CKC) (multi-joint exercises), and functional rehabilitation interventions was advocated. The use of OKC Isokinetic testing and rehabilitation peaked in the 1980s, due largely to the increasing body of evidence demonstrating its effectiveness in assessment and rehabilitation of patients with knee injuries. In the 1990s the focus switched to almost exclusively CKC exercises because they were considered more functional and thought to produce fewer rehabilitation complications, compared to OKC exercises. Beginning in the early 2000s an approach best characterized as “Functional rehabilitation” has been employed almost exclusively largely due to the empirical notion that it has a greater specificity to performance. Investigations in the 2020s have shown many patients following injuries/surgeries oftentimes still have residual strength and power deficits rendering them unable to return to their previous levels of performance. Due to these issues with difficulty returning to unrestricted participation, the current trend is heading back to performing objective isokinetic testing to assess the performance capabilities of associated muscle groups, in conjunction with a battery of other functional tests to both guide rehabilitation and determine readiness to resume higher-level activities.
The proven effectiveness of isokinetics and the large number of patients unable to return to pre-injury levels of activity because of significant strength, power and endurance deficits are why we advocate a “Test, Don’t Guess!” approach that makes the data derived from isokinetics a critical part of the return to play methodology. There are 2 imperatives employed when using isokinetic testing. First, it assists in providing objective data to help guide progression through a rehabilitation program, particularly in the advanced phases. Second, isokinetic testing assists the assessment of readiness for discharge aimed at ensuring a successful return to sport (RTS). RTS readiness frequently includes a number of assessments, including patient reported outcomes (PROs) impairment measurements, muscular strength, power and endurance tests, functional performance tests, neuro-cognitive reactive tests,1 and finally sport specific tests.
Recently there have been several articles which have reported a quadriceps strength value of 90% or better when compared to the contralateral (uninjured) knee as one of the four or five criteria to reduce the risk of reinjury to the knee following anterior cruciate ligament (ACL) surgery.2,3 Furthermore, anecdotally clinicians and researchers have repeatedly stated they are looking for limb symmetry of the quadriceps and hamstrings before returning individuals to a running program or sports participants. With these important criteria stated by many – clinicians require an accurate, objective, and reproducible method of testing to ensure these parameters are met prior to returning anyone back to unrestricted athletic participation.
The focus of this clinical commentary is to address testing of muscle strength, power, and endurance. Using the knee as a model, muscle performance testing can be performed using a variety of methods including manual muscle testing (MMT), handheld dynamometry (HHD), isotonic progressive resistive exercise (PREs) testing using knee extensions and/or leg press movements, squatting, and isokinetics. Multi-joint isotonic tests like the leg press or squat may demonstrate a performance weakness, but because multiple muscle groups are being used in the movement the actual point of weakness and degree of deficit within the kinetic chain are difficult to truly isolate.
Objective muscle performance testing using isokinetics has numerous advantages. (Table 1) It can be used for pre-participation screening to identify potential deficits and allow for preventive interventions to reduce injury risk. Isokinetic testing can be used to assess a patient’s status during rehabilitation to guide program progression. The objective documentation provided from isokinetic testing can be used in the development of criteria-based treatment plans. Despite the benefits the trend over the last few decades has been away from isokinetic testing. The movement away from isokinetics has by in large not been replaced with another form of dynamic muscle performance assessment. This lack of objective muscle performance data is partly responsible for the unfavorable RTS4–7 and high reinjury rates8–10currently prevalent following ACL surgery. The criteria needed for an accurate RTS determination are multi-factorial but muscular strength, power, rate of force development, and endurance are critical metrics that should be routinely tested as part of this decision-making process.1 Numerous studies have demonstrated the reliability of isokinetic muscle performance testing.11–14 Additionally, several studies have demonstrated that although the patient is strapped into the isokinetic testing device, it has good validity, and several studies have demonstrated a correlation between isokinetic performance and functional skills.15–17 For these reasons, isokinetic testing is still the “Gold Standard” for measuring dynamic muscle performance.
In contrast, performing isometric knee testing at a 90-degree angle with the patient in the seated position has become a popular assessment for quadriceps strength. There are several limitations to this technique: 1) the 90 degree angle pre-stretches the distal quads, but shortens the rectus femoris, 2) if this position is used, perhaps it should replicate the functional position of the hips with standing, walking or running by having the patient laying supine on the table, 3) the 90-degree position of the knee does not replicate the functional angle of the knee during most sporting activities and certainly not the position of the knee for the mechanism of injury with ACL injuries, and 4) the isometric contraction is not a dynamic motion, therefore, the measure is not a functional movement pattern and only has limited translation to strength beyond the 90-degree position of knee flexion.
Isokinetics has the ability to perform dynamic velocity spectrum testing to sample muscle performance at multiple speeds. Because sporting activities occur during multiple speeds of movement there is a need to assess the muscles involved in multiple ways that can mimic acceleration, deceleration, and speed of movement. Moreover, by testing and strengthening muscles at various speeds, the patient should be better prepared to successfully progress through their rehabilitation program and ultimately RTS. The uniqueness of isokinetics is predicated on the concept of accommodating resistance. As the biomechanics of the joint and the length of the muscle-tendon unit changes throughout the range of motion, the forces will change and isokinetics allows for specificity of testing or rehabilitation by providing accommodation as the range of movement changes. Isokinetic testing allows for dynamic muscle performance testing which has been shown to correlate with functional movements.19–25 Isokinetics have been used for 56 years,26 the first book dedicated to isokinetics was published 40 years ago,27 an entire journal was developed that was dedicated to isokinetics (Isokinetics & Exercise Science) and there have been thousands of articles demonstrating the effectiveness for testing, training, and rehabilitation, with a PubMed search in January of 2024 returning 9,381 articles in Index Medicus journals including isokinetics.
The decline in use of isokinetics noted previously was not solely related to shifting trends in rehabilitation philosophy. The 4 most cited barriers to isokinetics are accessibility, unit size, device complexity and most importantly cost. Not everyone has access to an isokinetic device, generally for the other 3 reasons and they are becoming less and less available. As clinic size has decreased from the once extravagantly large facilities of the 1980’s and 1990’s, the overall footprint of the current large devices are no longer practical. The device systems are terribly complex owing to the attempt to test as many joints and movements as possible, despite the practical clinical need for most of this complexity (Figure 1). Finally, cost has become the driving factor in so many healthcare decisions and the ability to afford an isokinetic testing system is no different. To address all these barriers a prototype isokinetic knee dynamometer system has been developed (Figure 2). This device has a very small footprint, only tests knee extension/flexion, and promises to provide a lower cost method of isokinetic knee testing.


Isokinetic Testing and Interpretation
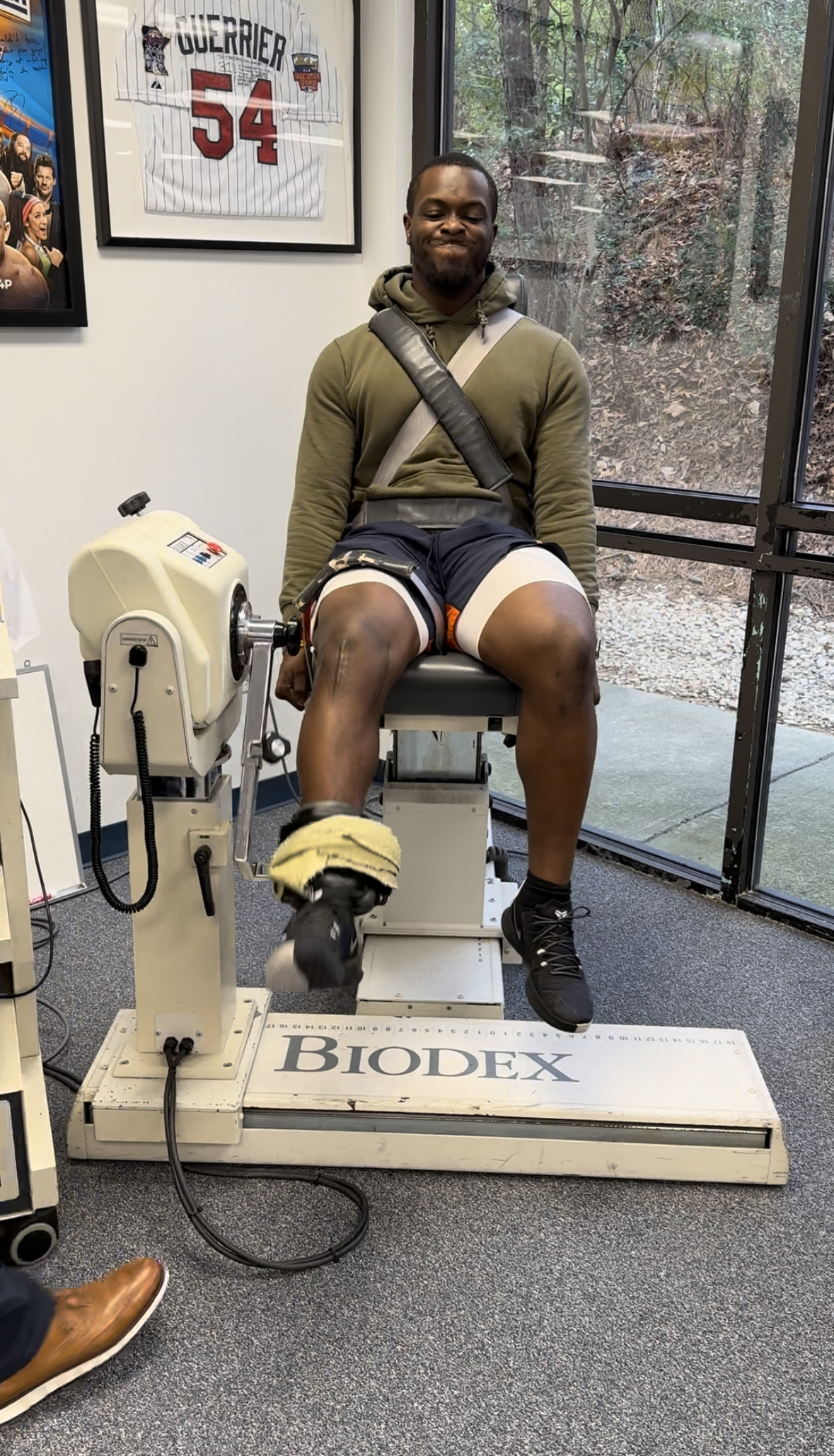
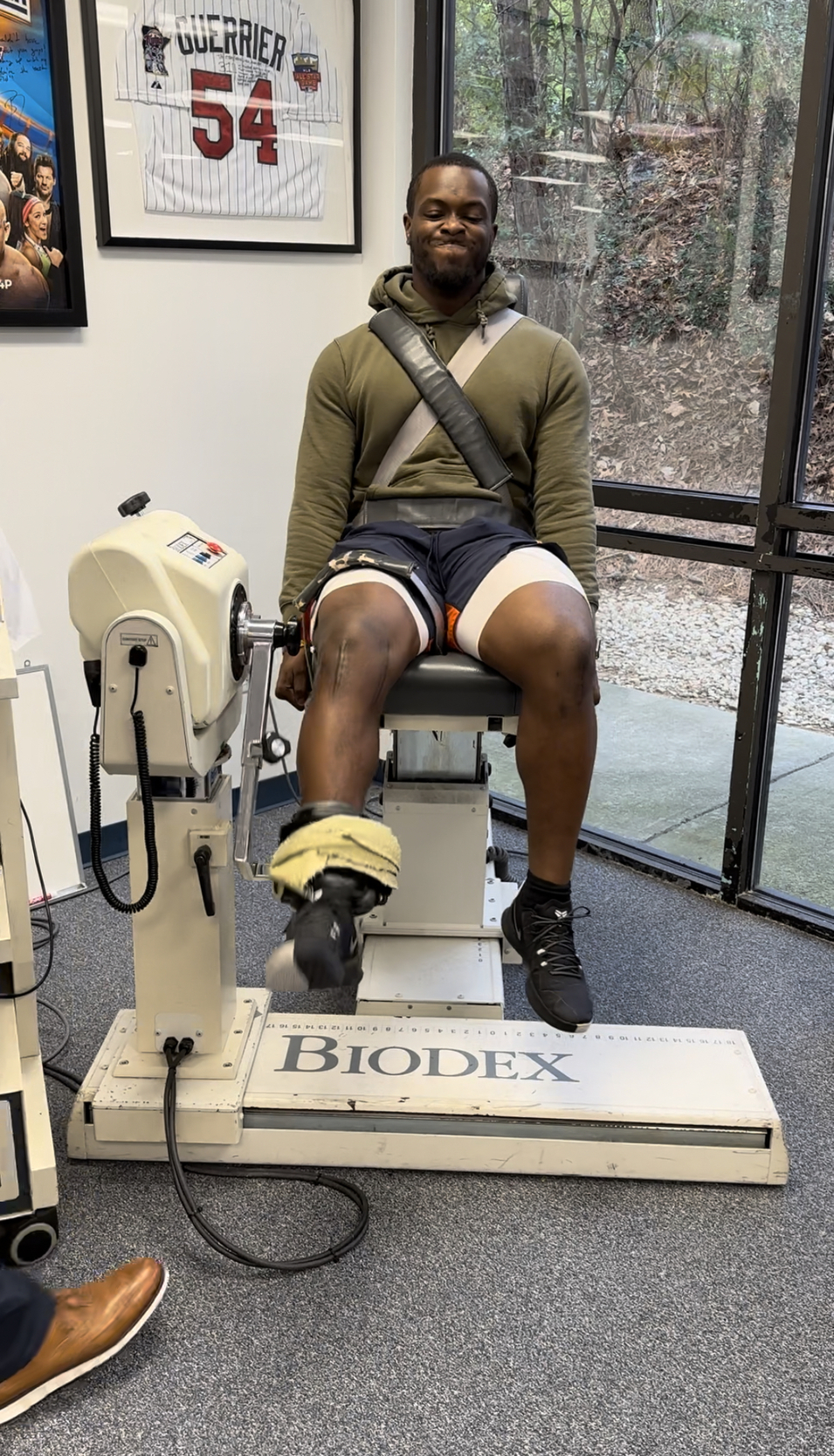
Isokinetic testing of the knee flexors and extensors is performed in a seated position using a dynamometer to measure the muscle performance parameters of strength, power, rate of force development, work, and endurance (Figure 3a and 3b). Testing can be performed at multiple angular velocities but is most commonly performed at 180 and 300 degrees/second, as these speeds have been shown to closely approximate functional activity.16,17,28

It is worth mentioning here that one of the persistent criticisms against isokinetics is creating large patellofemoral compression forces and tibial sheer during testing. This is attributable to the early use of testing at 60 degrees/second. Historically, the measurement of peak torque was determined by manually measuring the value on thermal graph paper. Sixty degrees/second was adopted because it was the simplest way to generate a force curve that could be easily measured and interpreted with the testing methods available. Unfortunately, not only is 60 degrees/second not functional or ideal for testing, the practice of using this speed in testing has persisted despite advancements in the computerized software used to assess a test which make the need for manual measurement unnecessary. In Addition, testing at 60 degrees/second produces significantly higher patellofemoral reaction forces and greater anterior tibial translation than the faster speeds of 180 and 300 degrees/second.29 Conversely, speeds beyond 300 degrees/second have been shown to be too fast for many but the highest functioning athlete to be able to “catch” the dynamometer and register values during testing.30
Key isokinetic testing parameters to evaluate include quadriceps torque to body weight ratio at 180 degrees/second, hamstring/quadriceps ratios, bilateral comparisons (Limb Symmetry Index-LSI) of the quadriceps and hamstrings, acceleration rate at 0.2 seconds of knee extension, and endurance values for both the quadriceps and hamstrings musculature. The complete isokinetic testing parameters evaluated and their goals for RTS assessment are outlined in Table 2. While a comprehensive assessment of all parameters and their correlation of other functional testing measures is imperative for an overall picture of the patient as a whole, the testing parameters that have been found to be most beneficial in a battery of test assessments are: T-shuttle run, hop testing, force plate data, and neurocognitive reactive functional testing.
Summary
It is important to perform a battery of tests for pre-participation screening, assessing a patient’s progress through a rehabilitation program, and criterion-based subjective and objective testing protocols for RTS. Isokinetic testing allows for dynamic velocity spectrum testing of multiple muscle groups, although this clinical commentary only focused on knee testing. There is ample research to demonstrate quadriceps deficits last for prolonged periods of time following ACL injuries and after reconstructions. Therefore, it is important to assess the muscle’s performance in each link of the kinetic chain to determine if any isolated weaknesses exist. Despite the limitations of cost and availability isokinetics remains an integral part of the successful formula to assess muscular strength, power, and endurance in an objective manner. Because of the compelling arguments in favor of isokinetics and the need to solve the current re-injury and readiness in return to play issues perhaps the future lies in a dedicated isokinetic knee testing and rehabilitation system.31 This type of dedicated isokinetic knee system may provide the solution to cost effective objective muscle testing. The authors of this article look forward to the future direction of objective muscle assessment, return to play testing, and reducing the incidence of ACL injuries and reinjuries. We feel that isokinetics remains the best method to objectively determine dynamic muscle strength, power, rate of force development, and endurance.