


Introduction
The “Basas” Spanish Squat has been presented in literature as a recommended exercise for treatment of patients with patellar tendinopathy.1–4 A variation of the exercise which included superimposed electrical stimulation (E-stim) during the exercise was first introduced in 2014.2,3 Incorporating the Basas Spanish Squat with, and without E-stim has shown promising results for reducing pain in athletes with patellar tendinopathy.3,4 When performed correctly with the appropriate setup, the Basas Spanish Squat can be a challenging exercise for the quadriceps even when the movement is isometric and seems simple. The highest level of evidence regarding exercise therapy for tendon injuries entails heavy loaded exercises that subsequently maximize load through the tendon,1,5–8 commonly referred to as mechanotherapy,9 and the Basas Spanish Squat exercise with and without E-stim is thought to do that with a simple setup. At the biomechanical level, tendon load can be defined as a high level of tendon force,10,11 which results in higher levels of mechanical strain10,12–15 within the targeted tendon. This high level of mechanical strain is what induces therapeutic changes at the cellular and molecular level which leads to recovery.5
Evidence is clear that tendon loading is key for successful treatment of patients with patellar tendon injuries.1,5,7,16–18 What is less commonly discussed, however, is that prescribing “tendon loading exercises”, does not always equate to optimal “tendon loading”. Quadriceps inhibition is common in patients with patellar tendon injuries,19 and biomechanical analyses have quantified that patients with knee pathologies compensate by shifting load towards the contralateral limb (during bilateral tasks), and their hip and ankle joints on the ipsilateral side.20–23 This can be problematic in the clinical setting, since unless there are clear visible deviations in mechanics, there is no objective way to know if the “tendon loading exercise” prescribed is in fact loading the tendon. The mechanism by which the Basas Spanish Squat with E-stim is thought to overcome this issue, is through the additional electrically stimulated contraction of the quadriceps muscles which gives the patient no choice but to load the patellar tendon.3,24 This could mean that patients with quadriceps inhibition or with significant compensations during exercises can still optimize patellar tendon load through superimposed E-stim. This additional contraction from E-stim likely induces higher levels of mechanical strain at the patellar tendon, but this has yet to be confirmed using objective measurements of tendon load.
Ultrasound imaging technology has advanced in recent years and methods for measuring tendon strain, a surrogate to tendon forces or “load”, have been described.25,26 Specifically, Edama et al. described their methods to be near excellent (ICC = 0.804 – 0.946) in reliability when measuring patellar tendon strain during open kinetic chain knee extensions and during squatting.25 These methods are simple, timely, and can be implemented easily into clinical practice if appropriate equipment is available.27 Arampatzis et al. suggest the use of objective clinical assessments of tendon strain for targeted intervention when treating patients with tendinopathy.28 Given the importance of tendon loading for tendon rehabilitation, and the advancements in technology and recommendations for quantifying tendon strain, there is a need to evaluate exercises and methods that augment strain in the targeted tendon. The purpose of this case series was to calculate and compare patellar tendon strain using ultrasound imaging during the Basas Spanish Squat with, and without E-stim, and open kinetic chain knee extension.
Methods
Participants
Four healthy active participants29 with no history of major lower extremity injuries, surgeries, or current symptoms in their patellar tendon30 were tested (Table 1). Testing was performed unilaterally on a leg chosen using a random number generator.
Ultrasound imaging
Extended field of view ultrasound images (GE Healthcare, Logiq e, Frequency: 10MHz, Depth: 2~3 cm) were collected at rest and during exercises at 90 degrees of knee flexion31 for all exercises to calculate patellar tendon strain. Patellar tendon length was defined by the deep attachment of the patellar tendon at the tibia and at the patella.32 Strain was defined as the change in patellar tendon length (contracted – resting) divided by the resting length and expressed as a percentage (%). Each resting length and concurrent exercise images were captured three times, and an average was used to calculate strain.
Open kinetic chain knee extension
After a standardized warm-up, knee extension maximum voluntary isometric contraction (MVIC) tests were performed on an isokinetic dynamometer in 90 degrees of knee flexion (Biodex System 3, Shirley, NY). Peak MVIC was then used to calculate 60% MVIC and participants performed three trials of isometric contractions with a visual target line while simultaneous ultrasound images were collected (Figure 1 and Supplementary File 1). Sixty percent MVIC was chosen as the reference point for this study, as data presented by Edama et al.25 has established reliability of this method up to this intensity.

Basas Spanish Squat without E-stim
The Basas Spanish squat was performed by setting up a rigid strap fixation immediately below the knee joint line. The participants were asked to squat while keeping the trunk upright until they reached 90 degrees of knee flexion (Figure 2). Knee joint angle was tracked throughout the movement using a goniometer and ultrasound images were taken once the participant reached 90 degrees of flexion in the limb being tested. Resting lengths were calculated with the participants sitting upright in a chair with the quadriceps relaxed and knee at 90 degrees (same position as during the squat).

Basas Spanish Squat with E-stim
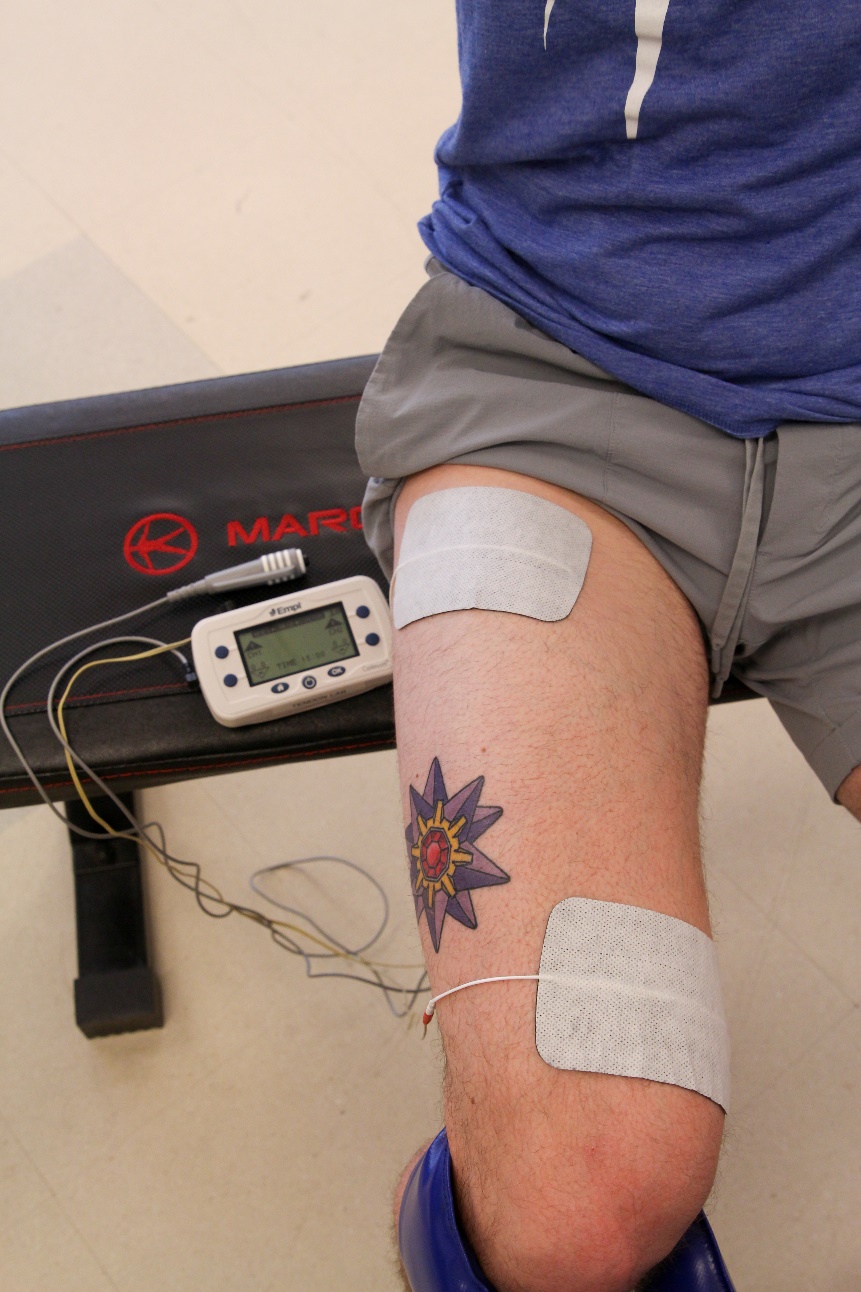
E-stim was delivered using a commercial electrical stimulator (Chattanooga, Continuum. Settings: biphasic pulse, 75Hz, 400μs, 0 second ramp, trigger activated) with a trigger and two 3 inch × 5 inch electrodes placed over the quadriceps motor points33 (Figure 3).

The stimulation was initially dosed to maximal tolerance (i.e., the highest possible level of quadriceps contraction tolerated by the participant) with the participant in the bottom position of the Basas Spanish Squat prior to the testing trials. Once maximum tolerance was identified, the participant performed the same procedure as the condition without E-stim, but this time the trigger was activated manually by the participant once the knee reached 90 degrees of flexion (Figure 4 and Supplementary File 2). Patellar tendon lengths were then collected in this position to calculate strain.

Results
Open kinetic chain knee extensions at 60% MVIC yielded higher levels of strain compared to the Basas Spanish Squat without E-stim in all four healthy participants. Once the E-stim was added, strain approximately doubled in three out of the four participants and increased seven-fold in one participant (Table 2). This one participant did, however, demonstrate minimal strain during the “without E-stim” condition which may have exaggerated the percent increase in strain once E-stim was added. This small cohort also demonstrated a large variability in strain, yet the relative relationship between each testing condition was consistent and clear amongst the four participants; lowest during the Basas Spanish Squat without E-stim, followed by the open kinetic chain knee extension at 60% MVIC, and highest during the Basas Spanish Squat with E-stim (Table 2).
Discussion
The purpose of this case series was to calculate and compare patellar tendon strain, using ultrasound imaging, during the Basas Spanish Squat with, and without E-stim, and open kinetic chain knee extension in a small healthy cohort. Even with a small cohort, a clear pattern emerged from our results; superimposition of E-stim during the Basas Spanish Squat increases tendon strain during the exercise. The findings suggest that if the target of an exercise intervention is to induce additional load (or strain) to the patellar tendon, adding E-stim during the Basas Spanish Squat is an option. The level of increase in strain varied slightly among the four participants, but this may be attributed to each participants’ tolerance to E-stim (i.e., those who tolerated higher levels of current may have demonstrated greater increase in strain).
The results from this case series may in part explain the mechanism behind the positive findings by Basas et al.3 who incorporated the Basas Spanish Squat with E-stim during rehabilitation of high-level athletes with chronic patellar tendinopathy (over multiple seasons) to manage symptoms throughout competition. The additional strain the patellar tendon experienced from superimposition of E-stim may affect tendon remodeling and recovery in ways not achieved with voluntary muscle contraction alone. Further investigation, however, on the effects of additional strain from the E-stim on tendon properties34 and clinical outcomes19 are necessary. Superimposition of E-stim during a slow sit-to-stand exercise has also shown similar improvements for strength and symptoms in a cohort of 32 patients with patellar tendinopathy while limiting the pain experienced during exercise compared with heavy, slow resisted exercise.24 A similar effect of E-stim on patellar tendon strain may occur during exercises other than the Basas Spanish Squat, thus, clinicians may consider application of E-stim during other patellar tendon loading exercises.
While results presented are from a small healthy cohort, quadriceps inhibition, or the inability to fully activate all motor units in the muscle,35 is common after knee injuries.36 Patients with patellar tendon injuries who produce weaker voluntary quadriceps contraction to load the patellar tendon may see further benefit of using superimposition of E-stim in their care. Quadriceps inhibition and disuse can lead to subsequent underloading of the patellar tendon, meaning forced contraction of the muscle through E-stim may be necessary to appropriately provide mechanical strain. Patients with patellar tendinopathy commonly shift load towards their hip and ankle joints during exercise,20–23 which can lead to performing prescribed exercises while subconsciously shifting load away from the targeted muscle and tendon even if appropriate instruction is given. This alteration is not specific to the performance of the Basas Spanish Squat, and E-stim can be used during open kinetic chain knee extension exercises or other closed kinetic chain exercises as well, depending on the needs of each patient. If dosed appropriately, superimposition of E-stim bypasses quadriceps weakness and inhibition that limits voluntary quadriceps force production, as this method provides additional involuntary contraction at the quadriceps and induces higher levels of patellar tendon strain.
The appropriate dose and settings for superimposition of E-stim to manage patellar tendon injuries varies within the literature,2,3,24 and clinicians considering the use of this modality may question what parameters they should be using for their patients. The authors believe that the exact stimulation parameters and dosing is likely not the most important, given that the literature in treatment of tendinopathy continues to suggest that the type of loading (eccentric vs concentric vs isometric) does not influence outcomes.37 Tendons respond to mechanical load, so parameters and repetition schemes that can achieve the highest level of strain while minimizing discomfort at the quadriceps and pain at the patellar tendon, is likely the best to use. Information on optimal E-stim parameters has been documented in the neuromuscular electrical stimulation (NMES) literature that has traditionally targeted recovering quadriceps strength after traumatic knee injuries such as anterior cruciate ligament injuries.38,39 Available evidence and clinical recommendations40 were considered in choosing the parameters used for this study. The authors recommend that clinicians use these parameters as guidelines, but also modify parameters as necessary to individualize for comfort and maximize knee extension torque output. The other key component for appropriate dosing is the ability to measure patellar tendon strain25 and/or knee extensor torque41 during the exercises. If imaging modalities are available, it is beneficial to quantify and confirm the amount of strain the patellar tendon experiences during exercises to appropriately dose the exercise.
Some limitations must be considered. Given the small cohort and explorative nature of this case series, further investigation with a larger sample is necessary, however, clear effects using reliable methods were found. There is also a need to compare clinical and functional outcomes following implementation of this exercise as part of a protocol treating a cohort of patients with patellar tendon injuries.
Conclusion
The Basas Spanish Squat with E-stim should be considered as a key exercise in optimizing rehabilitation of athletes with patellar tendon injuries through maximizing tendon strain and promoting tendon recovery and remodeling.
Corresponding Author
Karin Grävare Silbernagel
540 S. College Ave, Newark, DE 19713, USA
Email: kgs@udel.edu; Phone: 302-831-4808; Fax: 302-269-8011
CONFLICTS OF INTEREST
The authors report no conflicts of interest.
ACKNOWLEDGEMENTS
This study is based on a collaboration that began when Carlos Basas was visiting the Delaware Tendon Research lab and shared the Basas protocol, developed by his father Ángel Basas, that was utilized in Spain to treat athletes with patellar tendinopathy. During the manuscript preparation Ángel and Carlos Basas passed away in a tragic accident. The publication of this manuscript is in honor of their hard work in pursuing excellence in their profession to help those with tendon injuries recover and perform at their best.