



INTRODUCTION
The rapid growth of women’s football (soccer) participation is bringing about increasing rates and earlier occurrence of primary Anterior Cruciate Ligament (ACL) injury.1,2 Several authors have demonstrated that female footballers are at overall higher risk of ACL injury than their male counterparts1,3,4 and are less responsive to targeted preventative interventions e.g., the FIFA 11+ program.1,5,6
Therefore, a deeper comprehension of modifiable risk factors, such as ACL injury biomechanics, has been advocated to mitigate the injury risk in female football academies.7,8 Standardized methodologies are crucial to obtain objective measurements of players’ movement quality and identify ACL injury predictors in a user- and athlete-friendly fashion.
The 3D motion capture is the gold standard for biomechanical assessment of high-demanding tasks and has been used in prospective investigations of ACL injury predictors.7,9 Recently, 2D video-analysis has been proposed as a cost-effective alternative to 3D motion capture for high-demand tasks. Promising results have reported regarding the association between 2D angles (frontal plane knee, pelvis, and trunk angle; limited knee and hip flexion) and scoring systems (Movement Analysis Test, Cutting Movement Assessment Score) based on video-analysis and well-known ACL risk factors such as the knee abduction moment (KAM) and high vertical and posterior ground reaction forces (GRF).10–13 Such 2D scoring systems allow for simpler movement analysis for the raters and quicker feedback to the athletes, making them an attractive solution to implement large screenings in young population.12–14
However, the efficacy of 2D video-analysis in determine the risk of the occurrence of ACL injury has never been assessed prospectively in male nor female football players. The efficacy of 2D video-analysis and its agreement with 3D motion capture would support the use of dedicated methodologies to test female football players in primary ACL injury prevention.
The purpose of the present pilot study was to prospectively investigate the biomechanical predictors of ACL injury during a COD task in female football players using both gold standard 3D motion capture and a qualitative scoring system based on 2D video-analysis. The hypothesis was that both the 3D motion capture and the 2D scoring system would detect clinically-relevant biomechanical differences between non-injured and ACL-injured players such as shallower lower limb flexion and dynamic valgus.
MATERIALS AND METHODS
The study was approved by the Institutional Review Board (IRB approval ID number: 555/2018/Sper/IOR of 12/09/2018) of Area Vasta Emilia Romagna Centro (AVEC, Bologna, Italy) and registered on ClinicalTrials.gov (Identifier: NCT03840551). Signed informed consent were collected from all participants before enrollment.
Participants
This represents a secondary analysis of a larger cross-sectional study aimed to investigate the concurrent validity of different methodologies (wearable inertial sensors and 2D video-analysis) for examining high-demand motion tasks for ACL injury prevention and rehabilitation.10,15 The analysis was conducted in the Education and Research Department of the Isokinetic Medical Group during the regular football season (February 2019). Sixteen young competitive (first-to-third Italian Football division) female football (soccer) players (age 21.4 ± 4.3, range 18-31) were enrolled in the study. Exclusion criteria were: evidence of previous severe injury (> 28 days recovery time); previous surgery to the lower limbs; body mass index (BMI) > 35; and cardiopulmonary or cardiovascular disorders.
Data Collection
Each player performed a series of pre-planned 90° COD tasks at maximum speed possible in a specialized laboratory equipped with artificial turf. The players wore their own running shoes and clothes. The COD task consisted of a 6-meter frontal sprint followed by a 90° sidestep cut with foot strike on a force platform and a further 3-meter sprint. The complete acquisition setting was previously described.10 In brief, a 10-minute dynamic warm-up and few unrecorded repetitions of the movement were performed by each player to get confident with the setting. The players were instructed by a single sport & exercise medicine physician specialized in sports biomechanics (F.D.V.), who also verified the validity of each trial. Full foot contact on the force platform was required to consider a trial valid. Each player performed six valid trials with three right and three left strikes.
3D motion data and 2D video-analysis data were collected simultaneously. 3D Motion data were recorded through a set of 10 stereophotogrammetric cameras (VICON Nexus, Vicon Motion Systems Ltd, Oxford, UK) and a force platform embedded in the floor (AMTI 400*600, Watertown, MA USA), and three high-speed cameras placed frontally and bilaterally towards movement direction to capture 2D data. The systems were synchronized for direct data comparison. The sampling rate was 120 Hz for cameras and force platform, and 100 Hz for the high-speed cameras.
The system calibration was performed at the beginning of the acquisition and repeated periodically during the session. Forty-two retroreflective markers were placed on each participant by a single expert user according to the full-body Plug-in Gait protocol. Anthropometric data were collected for each participant and model calibration was performed before data acquisition.
Data Processing – 3D Motion Capture
Marker trajectories were collected through the stereophotogrammetric cameras and interpolated through a spline-based algorithm. The lower limb and pelvis kinematics were computed through VICON Nexus software using the Cardan angles. The frontal, transverse and sagittal plane kinematics waveforms were extracted for the stance phase of the foot on the force platform. The positively defined rotations (+) were: knee varus and internal rotation, hip adduction and internal rotation, ankle inversion and internal rotation, and pelvis contralateral drop and rotation.
Data Processing – 2D Video Analysis
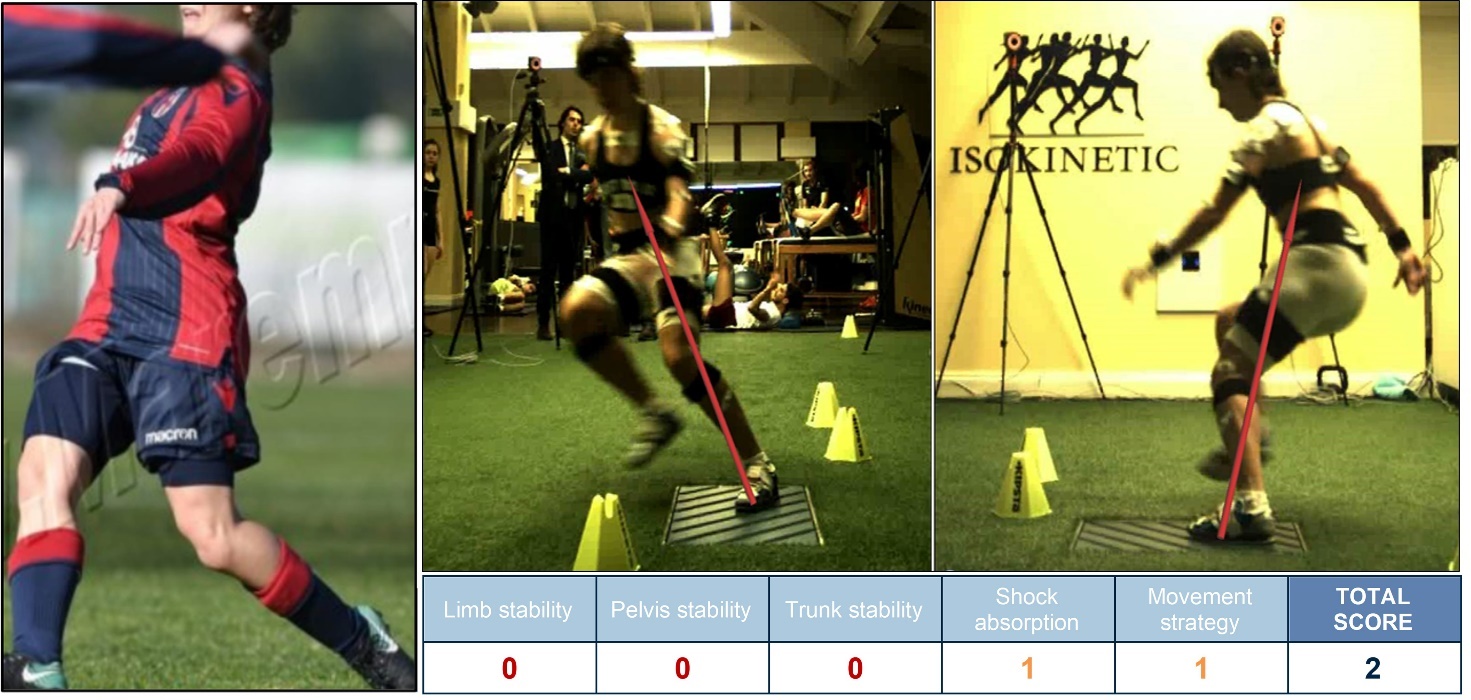
The 2D frontal and transverse plane joint kinematics was computed through video-analysis. The evaluation was performed in a specific VICON software environment through the recordings of the three high-speed cameras. Joint kinematics was evaluated at the frame of maximal knee flexion angle after the foot contact on the force platform. For each trial, the following 2D angles were calculated: Foot Projection Angle (FPA), Frontal Plane Knee Projection Angle (FPKPA), Pelvis tilt Angle (PA), and Trunk tilt Angle (TA). Furthermore, a scoring system was adopted based on the 2D kinematics.10,16 Five scoring criteria were used to evaluate each COD trial: limb stability (LS), pelvis stability (PS), trunk stability (TS), shock absorption (SA), and movement strategy (MS). The detailed description of each criteria was reported in a previous study.10 In brief, a score from 0/2 to 2/2 (non-adequate to adequate) was attributed to the trial for each criterion based on objective 2D measurements by a single sports physician. The total score was computed as the sum of each criterion sub-score (maximum total score: 10/10).
Prospective Follow-up
The players were prospectively followed for the next two consecutive football seasons through regular phone calls. The occurrence of severe knee injuries (> 28 days recovery time) was registered. In case of an ACL injury, an MRI and a clinical examination were carried out to confirm the presence of the ACL tear. Additional information, e.g., the nature of the injury mechanism (non-contact, indirect contact, contact) and the context (training, match), were retrieved.
Statistical Analysis
Based on the occurrence of an ACL injury during the follow-up period, the players were divided into two groups: “No injury” and “ACL injury”. Kinematic data were retrieved for the injured and dominant leg for the latter and former group, respectively.17 The normal distribution of the data was verified through the Shapiro-Wilk test. The categorical variables were presented as a percentage over the total, while the continuous variables were presented as mean ± standard deviation (95% Confidence Interval – CI).
For the 3D kinematics waveforms, the two-tailed Student’s t-test with Statistical Parametric Mapping (SPM) was used to investigate the difference between the two groups.18
For the 2D analysis, the two-tailed Student’s t-test was used to compare continuous 2D kinematics variables, and Cohen’s d effect size was reported. Effect size was considered small, medium, and large for Cohen’s d value of 0.2, 0.5, and 0.8, respectively. Furthermore, the Chi-square test for 3x2 (3 scores x 2 groups) contingency tables was computed to investigate the differences in the 2D scoring system percentage between the two groups for each of the five criteria. The Mann-Whitney U test was used to investigate the differences in the total score and in non-normally distributed variables, and Rank Biserial Correlation was reported as effect size measure. Differences were considered statistically significant for p<0.05. The statistical analyses were conducted in Matlab (The MathWorks, Natick, MA, US) and SPSS (IBM, Armonk, NY, US).
Given the pilot nature of the present study, no a-priori power-analysis was performed. However, the present cohort of 16 participants is consistent with previous pilot studies with similar purpose and methodological accuracy showing a minimum power of 0.80 for the analysis of frontal and sagittal plane knee and hip kinematics.19,20
RESULTS
Overall, four players out of 16 (25% of the cohort) experienced an ACL injury during the two football seasons following the data collection. All injuries occurred during football matches with a non-contact mechanism. A complete ACL rupture in all injured athletes was confirmed through MRI examination. No other severe joint/muscle injuries were reported. Age at the time of data collection was significantly lower (p=0.009) in the ACL-injured group, while no differences (p<0.05) were found in demographics and approaching COD speed between ACL-injured and non-injured players (Table 1).
3D Motion Capture
The ACL-injured players showed greater knee valgus (p=0.029) and internal rotation (p=0.017) during the early stance phase and lower knee flexion (p=0.023) during the late stance phase (Figure 1, first row). Less hip flexion (p=0.042) coupled with greater external rotation (p=0.003) were also noted in the ACL-injured group (Figure 1, second row). Furthermore, ACL-injured players showed greater ankle eversion tendency and contralateral pelvic drop (p<0.001, Figure 1, third and fourth row).

2D Video Analysis
ACL-injured players showed greater internal foot rotation, pelvic contralateral drop, lower knee flexion (moderate effect size), and contralateral trunk tilt (large effect size, Table 2, Figure 2). Pelvis stability and trunk stability scores showed the highest predictive value towards ACL injury (significantly more 0/2 scores in ACL-injured players, Table 3, Figure 3). Total score was significantly lower in ACL-injured players (moderate effect size), that never scored greater than 7/10 (Table 3, Figure 4).



DISCUSSION
The main finding of the present study was that both the 3D motion capture and 2D analysis of the COD technique offered predictive insights towards the ACL injury risk in female football players. Significant differences between players experiencing an ACL injury in the two seasons after testing and non-injured players were consistent with the current literature on non-contact ACL injury biomechanics.21–24 Moreover, the 2D scoring system successfully identified the ACL-injured players, that showed a lower total score (Figure 4). Thus, such a scoring system has the potential to identify female footballers at high risk for ACL injury in a cost-effective fashion.
A video-analysis study by Lucarno et al. recently described the ACL situational patterns and injury mechanism of professional female footballers, highlighting the frequent occurrence of non-contact or indirect contact injuries with multiplanar biomechanics.23 Injury biomechanics included knee dynamic valgus, limited lower limb flexion, pelvis and trunk tilt and rotation, and ankle rotation, consistently with the one of male counterparts.25 In the present study, all the differences found between ACL-inured and non-injured players agreed with the typical biomechanical profile for non-contact ACL injury described by Lucarno et al. and Della Villa et al.23,25
The ACL-injured players exhibited greater knee valgus and internal rotation and hip external rotation (Figure 1). These patterns have been shown to increase the KAM and the load on knee ligaments.24,26,27 In LS score, none of the ACL-injured players’ tasks was rated as 2/2. However, no differences in FPKPA were found and the overall rating was shifted towards the 0/2 score (Figure 2). These findings suggest a good sensitivity but a lower specificity of the LS score and the FPKPA for the ACL injury risk, in line with previous literature on other functional tests.28,29
Lower hip and knee flexion angles were also observed in the ACL-injured players in both 3D and 2D joint angles. Though not happening in the early stance phase, these results suggest a stiffer kinematic strategy adopted by the ACL-injured players.23,30,31
Pelvic drop was detected during the whole stance phase in the players that sustained an ACL injury (Figure 1). Pelvic drop and trunk lean in the ACL-injured players were also detected through the PA and TA 2D angles with a moderate-to-large effect. The PS and TS criteria strongly were the best predictors of ACL injury in the 2D scoring system: the percentage of trials rated 0/2 in the ACL-injured players was double than the non-injured players in the PS, and triple in the TS. Moreover, ACL-injured players were never rated 2/2 in PS. The association between poor core stability and the risk of knee overloading has been proposed in literature.12,13 The video-analysis studies on professional athletes clearly identified that ACL injuries happen with pelvis and trunk in non-neutral position.23,25 Donelon et al. recently listed the maintenance of an upright pelvis and trunk position among the actions aimed to modify the COD technique and mitigate the ACL injury risk.22 The results of the present study suggest that the analysis of pelvis and trunk frontal plane kinematics in 2D could effectively detect core imbalance during the COD task and that the scoring system described could have a strong predictive power towards the risk of ACL injury.
Greater ankle eversion was noted in the players that sustained an ACL injury in the second half of the stance phase (Figure 1). The 2D analysis revealed a more internal foot progression angle at peak knee flexion. Both aspects of the foot position indicate that ACL-injured players landed on the force platform adopting a more anticipatory strategy than the non-injured players. An anticipatory strategy with a greater internal foot progression angle has been associated with faster cutting but in conflict with a safe mechanism.32 Foot eversion and rotation are also common in the professional football players that sustain an ACL injury.23,25 The analysis of foot progression angle could give valuable insights on the attitude of players COD technique and strongly influence joint loading propagation on the kinetic chain.
The 2D total score proposed in the present study distinguished the players that sustained an ACL injury from the non-injured ones. Average total score was lower in the ACL-injured players (4.6 vs 2.4, moderate effect, Table 3) and none of the ACL-injured players’ trials were rated more than 7/10 (Figure 4). The total score is an intuitive measure that can be used by the professionals to track a player’s overall movement quality during the COD task and her progression over a prevention (or rehabilitation) program. From the results of the present pilot study, a total score of 4/10 or lower could be indicative or higher risk for ACL injury, while a score higher than 7/10 could be indicative of a protective COD technique.
The multiplanar risk factors detected in the players that sustained an ACL after testing were extremely congruent with the injury mechanism proposed in video-analysis studies on professional female footballers (Figure 5).23 Both the 3D motion capture and 2D video-analysis detected and agreed on most of the clinically-relevant differences. In the 2D video-analysis, frontal plane was indicative of a higher injury risk, but both frontal and sagittal view would be required to obtain a comprehensive measure of COD movement quality. Knee abduction angle, frequently used in multiple 2D assessments for this and other tasks (e.g., drop vertical jump, squats, and single-leg landings), might be not sufficient to explain the movement complexity and the relation with the ACL injury risk.28,29,33 Furthermore, approaching and landing strategies such as penultimate foot contact deceleration, anticipatory cut, flatfoot or heel strike, should be taken into account to finetune the assessment.11,12,22,34

In the present study, 25% of the cohort experienced an ACL injury. Previous larger prospective studies reported an injury rate of 7-11%.29,35,36 In the present study, the tests were performed in late February, thus close to one of the two peaks of injury occurrence identified in professional football players.23 All injuries occurred during matches and without a direct contact with an opponent. This is again in line with the predominance of non-contact/indirect contact mechanisms found in professional female footballers (88%23). The fact that ACL-injured players were younger (p=0.009) than the rest of the cohort is consistent with the data reporting earlier occurrence (younger age) of the first ACL injury in female football.37 All these aspects deserve awareness from the football medicine community and highlight the urgent need for dedicated tools to counteract such a high injury risk since more and more female players turn professional earlier.
The present study has some limitations. First, the present pilot investigation involved a small cohort; thus, inferences should be interpreted with caution and are far from being conclusive. Despite the sample size, the results of both the 2D and 3D analyses were consistent with current literature on ACL injury risk biomechanics.21–24 Prospective studies with larger cohorts are necessary to set a benchmark for objective measurements in ACL injury prevention in football. Second, the 90° COD task assessed in the present study was pre-planned. Recent studies suggest that unanticipated sidestepping tasks could offer important insights on ACL injury risk.38 Preventative testing should consider the use of both pre-planned and unplanned tasks to get a wider understanding of players’ injury risk. No muscular strength data were collected. Such data could have increased the level of detail of the players’ comparison. The data collection was performed in a single session and no post-operative investigation was performed on those who were injured. The longitudinal analysis of the ACL-injured players could be used to quantitatively inform the ACL rehabilitation programs.
The clinical relevance of the present work is that the adoption of a 2D video-analysis scoring system based on quantitative measurements has the potential to identify female football players at higher risk for ACL injury in a cost-effective fashion. The players could therefore benefit from additional preventative neuromuscular training. Given the rapid growth of female football and their greater predisposition to the ACL injury,4,39 dedicated methodologies assessing players’ movement quality and injury risk are fundamental to mitigate the injury rates in early football careers.
CONCLUSION
Significant kinematic differences during a planned COD task were identified between ACL injured and non-injured players with both the 3D and 2D methodologies. The biomechanical pattern of the ACL-injured players was strongly consistent with the video-analysis of ACL injured elite players.23 Both the 3D and 2D methodologies offered precious predictive insights to assess and mitigate the ACL injury risk in women’s football.
LIST OF ABBREVIATIONS
Anterior cruciate ligament (ACL)
Body Mass Index (BMI)
Body Weight (BW)
Change of Direction (COD)
Confidence intervals (CI)
Foot Projection Angle (FPA)
Frontal Plane Knee Projection Angle (FPKPA)
Ground Reaction Force (GRF)
Knee Abduction Moment (KAM)
Limb Stability (LS)
Movement strategy (MS)
Pelvis tilt angle (PA)
Pelvis stability (PS)
Shock absorption (SA)
Statistical Parametric Mapping (SPM)
Trunk tilt angle (TA)
Trunk stability (TS)
Conflict of interest
Each author certifies that he or she has no commercial associations (e.g., consultancies, stock ownership, equity interest, patent/licensing arrangements, etc) that might pose a conflict of interest in connection with the submitted article.
Funding
None.
Acknowledgments
The authors want to thank GPEM s.r.l. for the support in data collection.