

- Department of Neurosurgery, Aga Khan University, Karachi, Sindh, Pakistan.
- Department of Radiology, Aga Khan University, Karachi, Sindh, Pakistan.
- Department of ENT, Aga Khan University, Karachi, Sindh, Pakistan.
Correspondence Address:
Karim Rizwan Nathani
Department of Neurosurgery, Aga Khan University, Karachi, Sindh, Pakistan.
DOI:10.25259/SNI_59_2021
Copyright: © 2021 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Karim Rizwan Nathani1, Komal Naeem1, Hamid Hussain Rai1, Muhammad Danish Barakzai2, Haissan Iftikhar3, Saad Akhtar Khan1, Fatima Mubarak2, S. Ather Enam1. Role of redundant nerve roots in clinical manifestations of lumbar spine stenosis. 10-May-2021;12:218
How to cite this URL: Karim Rizwan Nathani1, Komal Naeem1, Hamid Hussain Rai1, Muhammad Danish Barakzai2, Haissan Iftikhar3, Saad Akhtar Khan1, Fatima Mubarak2, S. Ather Enam1. Role of redundant nerve roots in clinical manifestations of lumbar spine stenosis. 10-May-2021;12:218. Available from: https://surgicalneurologyint.com/surgicalint-articles/10796/
Date of Submission
22-Jan-2021
Date of Acceptance
15-Apr-2021
Date of Web Publication
10-May-2021
Abstract
Background: Redundant nerve roots (RNRs) are defined as elongated, thickened, and tortious appearing roots of the cauda equina secondary to lumbar spinal canal stenosis (LSCS). The study compared the clinical and radiological features of patients with LSCS with versus without RNR.
Methods: This retrospective study was performed on 55 patients who underwent decompressive surgery for degenerative LSCS. Patients were divided into two groups based on the presence of RNR in their preoperative magnetic resonance imaging, as evaluated by a radiologist blinded to the study design. Medical records were reviewed for basic demographic, clinical MR presentation, and outcomes utilizing Japanese Orthopaedic Association (JOA) scores.
Results: The mean age of enrolled patients was 57.1, with mean follow-up of 4.0 months. RNR was found in 22 (40%) of patients with LSCS. These patients were older than those patients without RNR (62.2 vs. 53.7). Interestingly, there were no statistically significant differences in clinical presentations, duration of symptoms, and outcomes using JOA scores between the two groups.
Conclusion: RNR is a relatively common radiological finding (i.e., 40%) in patients with LSCS. It is more likely to be observed in older patients. However, no significant differences were noted in clinical presentation and functional outcomes with respect to the presence or absence of RNR.
Keywords: Degenerative spine disease, Elongated nerve roots, Lumbar spine stenosis, Redundant nerve root
INTRODUCTION
Redundant nerve root (RNR) of the cauda equina is a radiological observation characterized by elongated, enlarged, tortuous nerve roots in patients with lumbar spinal canal stenosis (LSCS).[
Although the management of LSCS remains the same for patients with/without RNR, some consider RNR a poor prognostic factor.[
MATERIALS AND METHODS
Patient selection
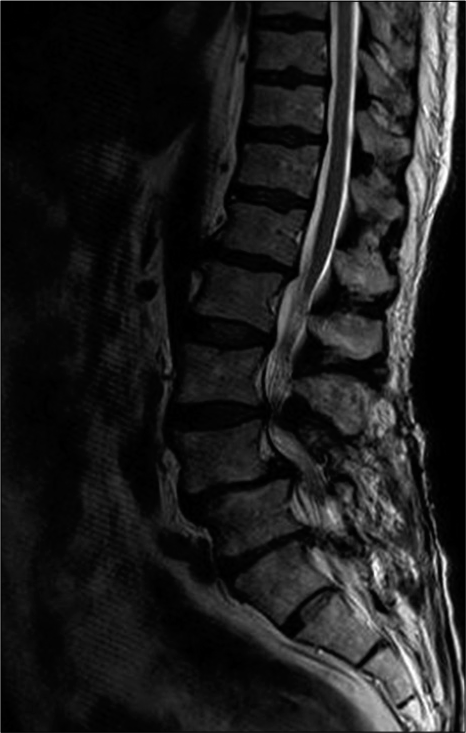
A total of 55 patients were over the age of 18 and averaged 57.1 ± 12.1 years of age. Thirty-two (58.2%) females and 23 (41.8%) males were enrolled in the study. This was a retrospective cohort study in neurosurgery. Patients had MR documented LSCS, and all had undergone surgical decompressive procedures (2015). Patients were diagnosed with/without RNR based on preoperative sagittal magnetic resonance imaging (MRI) studies as shown in
Patients in both groups exhibited similar preoperative modified total Japanese Orthopaedic Association (JOA) score (7.4 ± 2.3 vs. 7.3 ± 2.9; P > 0.05) [


Medical record review included an assessment of patients’ clinical, radiographic, and outcome data; low back pain (i.e., all had low back pain), neurogenic claudication/neurological deficits (i.e., motor, sensory, and sphincteric-urinary incontinence), and outcome analysis (i.e., based on JOA score) [



All individual preoperative JOA scores, except straight leg raise (SLR) test and urinary bladder function, were observed to be higher in the non-RNR group with none being statistically significant. Unforeseen, mean SLR test and bladder function scores were higher in the RNR group, 1.5 ± 0.7 and 5.4 ± 1.6, respectively, compared to non-RNR group, 1.2 ± 0.6 and 4.9 ± 1.8, respectively, but the differences were not significant (P > 0.05).
The follow-up ranged from 0 to 23.1 months (average 4.0 ± 4.5 months).
Statistical analysis
Continuous data were presented as mean, standard deviation for normally distributed variables or shown as frequency/percentages. Linear regression was used to assess difference in means between continuous data, and Pearson Chi-square test was used to assess difference between categorical data. Logistic regression was used to assess differences between categorical and continuous variables. Data were analyzed on Stata version 12 (StataCorp LLC, College Station, TX, USA).
RESULTS
Preoperative MR documentation of RNR
RNR was present on preoperative lumbar MRI studies in 22 (40.0%) patients (RNR group) and absent in the remaining 33 (60.0%) patients (non-RNR group).
Clinical features of RNR patients
Patients with RNR were older, averaging 62.2 ± 8.9 years of age versus non-RNR group patients averaging 53.7 ± 12.9 years old (P = 0.015).
The differences in symptoms present at discharge and at last follow-up were not statistically significant for either group (P > 0.05) (i.e., sensory disturbances and urinary incontinence at discharge were less common in the RNR group, but they exhibited more motor deficits all of which did not achieve “significance”) [
Intraoperative dural tears occurred in five patients with and five patients without RNR, but this difference was not significant (P > 0.05).
DISCUSSION
This study assessed the clinical presentation and functional outcomes of patients with LSCS with/without RNR. We found that RNR was present in 40.0% (22 of 55) of cases, consistent with the prior literature (range 33.8–42.3%).[
Although some have argued that RNR is a poor prognostic factor; we found no significant differences in outcomes in this study in patients with/without RNR.[
Although greater motor deficits and urinary dysfunction were found in patients with RNR at the time of preoperative assessment and discharge, along with a higher incidence of intraoperative dural tears, these findings were not statistically significant.
CONCLUSION
The present study demonstrated that 40% of MR studies document RNR in patients with LSCS on preoperative MR studies. Nevertheless, this finding does not appear to have any significant impact on the clinical presentation and neurological outcomes for these patients.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Chen J, Wang J, Wang B, Xu H, Lin S, Zhang H. Post-surgical functional recovery, lumbar lordosis, and range of motion associated with MR-detectable redundant nerve roots in lumbar spinal stenosis. Clin Neurol Neurosurg. 2016. 140: 79-84
2. Duncan AW, Kido DK. Serpentine cauda equina nerve roots. Radiology. 1981. 139: 109-11
3. Hakan T, Celikoğlu E, Aydoseli A, Demir K. The redundant nerve root syndrome of the Cauda equina. Turk Neurosurg. 2008. 18: 204-6
4. Hur JW, Hur JK, Kwon TH, Park YK, Chung HS, Kim JH. Radiological significance of ligamentum flavum hypertrophy in the occurrence of redundant nerve roots of central lumbar spinal stenosis. J Korean Neurosurg Soc. 2012. 52: 215-20
5. Min JH, Jang JS, Lee SH. Clinical significance of redundant nerve roots of the cauda equina in lumbar spinal stenosis. Clin Neurol Neurosurg. 2008. 110: 14-8
6. Ono A, Suetsuna F, Irie T, Yokoyama T, Numasawa T, Wada K. Clinical significance of the redundant nerve roots of the cauda equina documented on magnetic resonance imaging. J Neurosurg Spine. 2007. 7: 27-32
7. Ozturk AK, Gokaslan ZL. Clinical significance of redundant nerve roots of the cauda equina. World Neurosurg. 2014. 82: e717-8
8. Poureisa M, Daghighi MH, Eftekhari P, Bookani KR, Fouladi DF. Redundant nerve roots of the cauda equina in lumbar spinal canal stenosis, an MR study on 500 cases. Eur Spine J. 2015. 24: 2315-20
9. Steurer J, Roner S, Gnannt R, Hodler J. Quantitative radiologic criteria for the diagnosis of lumbar spinal stenosis: A systematic literature review. BMC Musculoskelet Disord. 2011. 12: 175
10. Suzuki K, Ishida Y, Ohmori K, Sakai H, Hashizume Y. Redundant nerve roots of the cauda equina: Clinical aspects and consideration of pathogenesis. Neurosurgery. 1989. 24: 521-8
11. Suzuki K, Takatsu T, Inoue H, Teramoto T, Ishida Y, Ohmori K. Redundant nerve roots of the cauda equina caused by lumbar spinal canal stenosis. Spine (Phila Pa 1976). 1992. 17: 1337-42
12. Tsuji H, Tamaki T, Itoh T, Yamada H, Motoe T, Tatezaki S. Redundant nerve roots in patients with degenerative lumbar spinal stenosis. Spine (Phila Pa 1976). 1985. 10: 72-82
13. Yokoyama K, Kawanishi M, Yamada M, Tanaka H, Ito Y, Hirano M. Clinical significance of postoperative changes in redundant nerve roots after decompressive laminectomy for lumbar spinal canal stenosis. World Neurosurg. 2014. 82: e825-30
14. Zheng F, Farmer JC, Sandhu HS, O’Leary PF. A novel method for the quantitative evaluation of lumbar spinal stenosis. HSS J. 2006. 2: 136-40

