

- Department of Neurological Surgery, Juntendo University Urayasu Hospital, Urayasu, Japan.
Correspondence Address:
Satoshi Tsutsumi, Department of Neurological Surgery, Juntendo University Urayasu Hospital, Urayasu, Japan.
DOI:10.25259/SNI_364_2022
Copyright: © 2022 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, transform, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Hiroki Sugiyama, Satoshi Tsutsumi, Hisato Ishii. Oculomotor nerve palsy presumably caused by cisternal drain during microsurgical clipping. 02-Sep-2022;13:398
How to cite this URL: Hiroki Sugiyama, Satoshi Tsutsumi, Hisato Ishii. Oculomotor nerve palsy presumably caused by cisternal drain during microsurgical clipping. 02-Sep-2022;13:398. Available from: https://surgicalneurologyint.com/surgicalint-articles/11844/
Date of Submission
20-Apr-2022
Date of Acceptance
18-Aug-2022
Date of Web Publication
02-Sep-2022
Abstract
Background: Oculomotor nerve palsy can be caused by diverse etiologies, but no report has yet documented its association with a cisternal drain.
Case Description: A 35-year-old woman presented with severe headache. The patient did not exhibit oculomotor nerve palsy at presentation. Cranial computed tomography (CT) revealed diffuse subarachnoid hemorrhage. The patient underwent open microsurgical clipping of a ruptured middle cerebral artery aneurysm. During surgery, a cisternal drain was placed in the basal cistern at the medial aspect of the clinoidal portion of the internal carotid artery. The patient presented with the left oculomotor nerve palsy immediately after surgery. CT revealed displacement of the cisternal drain to the lateral aspect of the anterior clinoid process. The patient’s mydriasis and sluggish light reaction recovered after 7 days, while extraocular movements persisted for 50 days. The constructive interference steady-state sequence detected the left oculomotor nerve coursing adjacent to the clinoidal internal carotid artery.
Conclusion: Oculomotor nerve palsy can be caused by collision with a thin silastic tube placed during surgery for aneurysmal subarachnoid hemorrhage. Withdrawal of the drain as early as possible is recommended when drain-associated oculomotor nerve palsy is suspected.
Keywords: Cisternal drain, Compressive neuropathy, Functional outcome, Oculomotor nerve palsy
INTRODUCTION
Cisternal drainage is a common neurosurgical procedure performed during microsurgical clipping of an aneurysmal subarachnoid hemorrhage, with the aim of continuous removal of subarachnoid clots lodged in the basal cistern.[
The oculomotor nerve, the third cranial nerve, initially arises from the medial aspect of the cerebral peduncle at the midbrain level. This then courses forward in the interpeduncular fossa and basal cistern, passes through the oculomotor triangle, and courses in the cavernous sinus. The nerve, then, passes through the central superior orbital fissure and enters the orbit.[
Here, we report a unique case of oculomotor nerve palsy, presumably caused by compression of a cisternal drain placed during surgery for aneurysmal subarachnoid hemorrhage.
CASE PRESENTATION
A 35-year-old, previously healthy woman, presented with severe headache and was transferred to the hospital. At presentation, the patient was drowsy, but did not show any focal neurological deficits. Her ocular position was neutral on both sides, and she presented with isochoric pupils. Ptosis was not found. Cranial computed tomography (CT) revealed a diffuse subarachnoid hemorrhage with a subtle ventriculomegaly. No abnormal findings were observed in the midbrain [

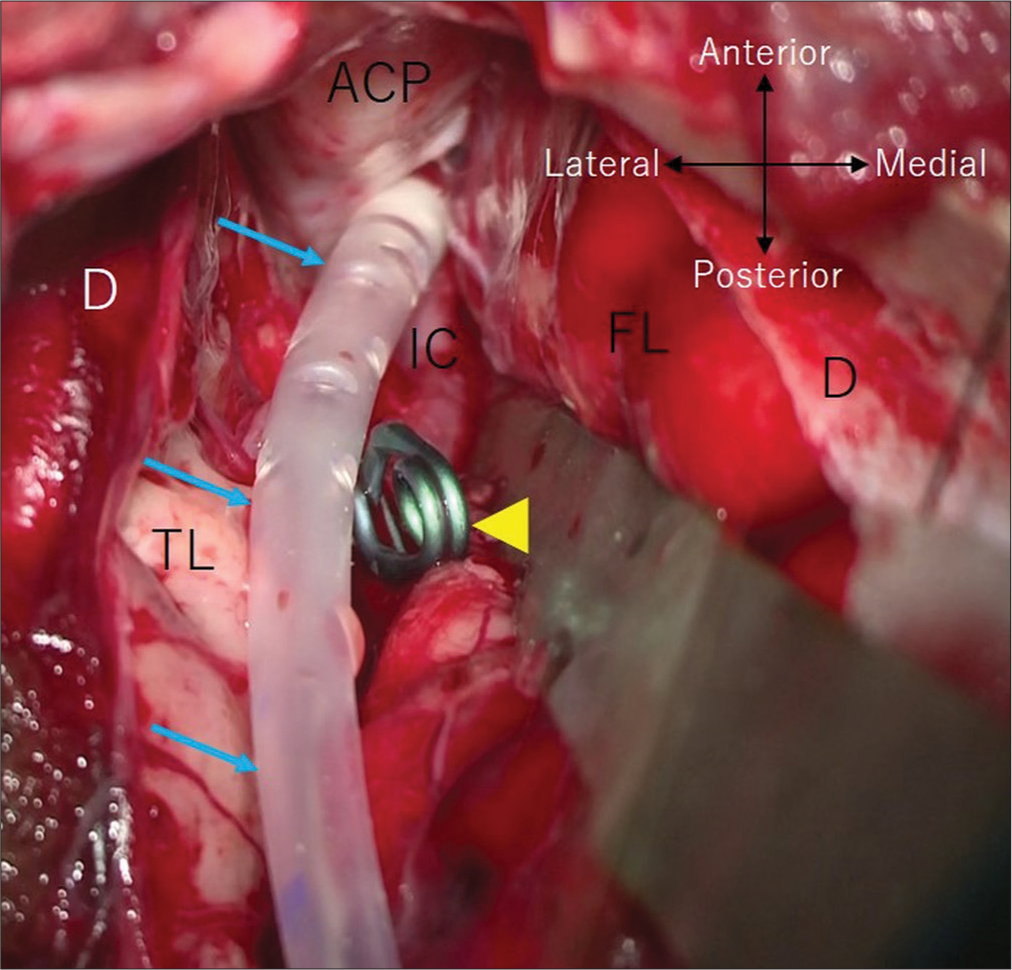
Figure 2:
Intraoperative photo showing a cisternal drain (arrows), placed with the tip at the medial aspect of the internal carotid artery and anterior clinoid process following application of a clip (arrowhead) to the neck of the middle cerebral artery aneurysm. D: Dura mater, FL: frontal lobe, and TL: temporal lobe. ACP: Anterior clinoid process; IC: Internal carotid artery.

Figure 3:
Axial (a and b) and coronal (c and d) computed tomography performed immediately after surgery showing the tip of the cisternal drain (a, c, d, arrows) displaced to the lateral aspect of the anterior clinoid process (ACP). DS: Dorsum sellae; Arrowhead: A clip applied to the ruptured middle cerebral artery aneurysm; Dashed arrow: ventricular catheter.

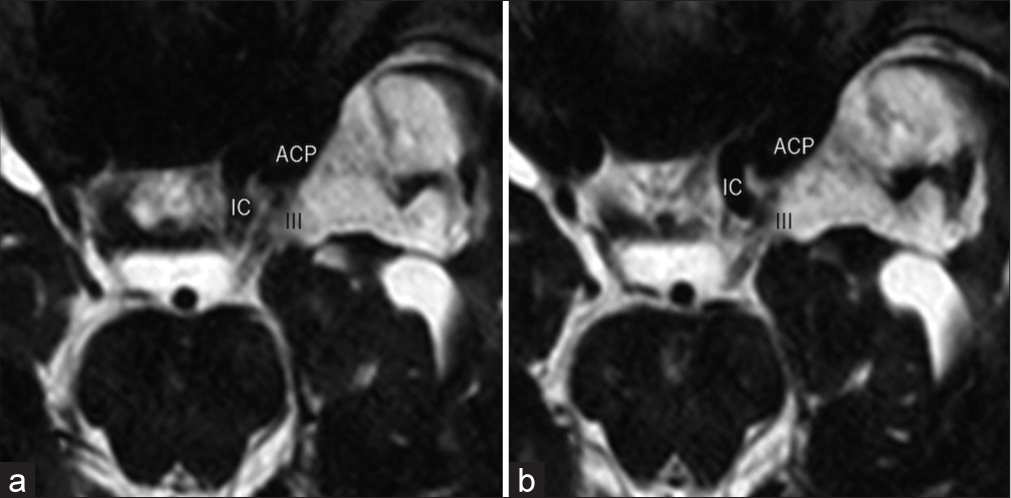
Figure 5:
(a and b) Adjacent images of the axial constructive interference steady-state sequence performed on postoperative day 30, showing the cisternal portion of the left oculomotor nerve (III) coursing adjacent to the lateral wall of the clinoidal internal carotid artery (IC). ACP: Anterior clinoid process.
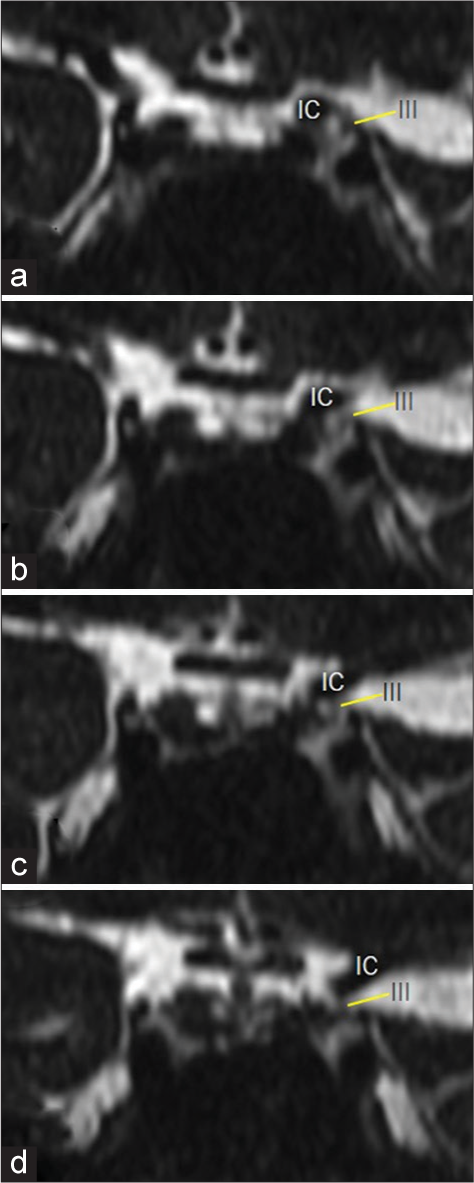
Figure 6:
(a-d) Serial images of the coronal constructive interference steady-state sequence performed on postoperative day 30, showing the cisternal portion of the left oculomotor nerve (III) coursing adjacent to the lateral wall of the clinoidal internal carotid artery (IC). a (anterior)→ d (posterior).
DISCUSSION
In the present patient, oculomotor nerve palsy was initially not found, but developed on the ipsilateral side immediately after surgery. CT performed immediately after surgery showed displacement of the tip of the cisternal drain, initially placed to the medial aspect of the anterior clinoid process, to the lateral aspect. No other significant CT findings associated with oculomotor nerve palsy were found. Furthermore, on the CISS sequence, the cisternal portion of the left oculomotor nerve was found to course adjacent to the lateral wall of the clinoidal internal carotid artery. Therefore, we assumed that the oculomotor nerve palsy was caused by collision with the displaced cisternal drain. Displacement of the drain probably occurred when releasing the retraction to the left frontal lobe at the final stage of the microsurgery, combined with the tight intracranial cavity of a young patient sustaining subarachnoid hemorrhage.
Few reports have documented cases of traumatic oculomotor nerve palsy.[
Cisternal drainage is a common neurosurgical procedure performed during microsurgical clipping of an aneurysmal subarachnoid hemorrhage but can cause neurovascular complications.[
CONCLUSION
Oculomotor nerve palsy can be caused by collision with a thin silastic tube placed during surgery for aneurysmal subarachnoid hemorrhage. Withdrawal of the drain as early as possible is recommended when drain-associated oculomotor nerve palsy is suspected.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Aoun SG, Welch BG, Cortes M, Stutzman S, MacAllister MC, El Ahmadieh TY. Objective pupillometry as an adjunct to prediction and assessment for oculomotor nerve injury and recovery: Potential for practical applications. World Neurosurg. 2019. 121: e475-80
2. Fujiwara S, Fujii K, Nishio S, Matsushima T, Fukui M. Oculomotor nerve palsy in patients with cerebral aneurysms. Neurosurg Rev. 1989. 12: 123-32
3. Gupta PK, Arif M, Shaik L, Singh R, Shah K. Solitary sign of third nerve palsy in a conscious patient with epidural hemorrhage. Cureus. 2020. 12: e10003
4. Horiuch T, Yamamoto Y, Kuroiwa M, Rahmah NN, Hongo K. Pontine infarction caused by medial branch injury of the basilar artery as a rare complication of cisternal drain placement. J Clin Neurosci. 2012. 19: 592-3
5. Kawakami Y, Shimamura Y. Cisternal drainage after early operation of ruptured intracranial aneurysm. Neurosurgery. 1987. 20: 8-14
6. Kim T, Nam K, Kwon BS. Isolated oculomotor nerve palsy in mild traumatic brain injury. Am J Phys Med Rehabil. 2020. 99: 430-5
7. Kinouchi H, Ogasawara K, Shimizu H, Mizoi K, Yoshimoto T. Prevention of symptomatic vasospasm after aneurysmal subarachnoid hemorrhage by intraoperative cisternal fibrinolysis using tissue-type plasminogen activator combined with continuous cisternal drainage. Neurol Med Chir (Tokyo). 2004. 44: 569-75
8. Kuo LT, Huang AP, Yang CC, Tsai SY, Tu YK, Huang SJ. Clinical outcome of mild head injury isolated oculomotor nerve palsy. J Neurotrauma. 2010. 27: 1959-64
9. Kurokawa Y, Ishizaki E, Inaba K. Incomplete oculomotor nerve palsy caused by an unruptured internal carotid-anterior choroidal artery aneurysm--case report. Neurol Med Chir (Tokyo). 2005. 45: 143-7
10. Lin C, Dong Y, Lv L, Yu M, Hou L. Clinical features and functional recovery of traumatic isolated oculomotor nerve palsy in mild head injury with sphenoid fracture. J Neurosurg. 2013. 118: 364-9
11. Natori Y, Rhoton AL. Microsurgical anatomy of the superior orbital fissure. Neurosurgery. 1995. 36: 762-75
12. Ogura K, Hara M, Tosaki F, Hirai N. Effect of cisternal drainage after early operation for ruptured intracranial aneurysms. Surg Neurol. 1988. 30: 441-4
13. Otawara Y, Ogasawara K, Kubo Y, Sasoh M, Ogawa A. Effect of continuous cisternal cerebrospinal fluid drainage for patients with thin subarachnoid hemorrhage. Vasc Health Risk Manag. 2007. 3: 401-4
14. Sasaki T, Kodama N, Kawakami M, Sato M, Asari J, Sakurai Y. Urokinase cisternal irrigation therapy for prevention of symptomatic vasospasm after aneurysmal subarachnoid hemorrhage: A study of urokinase concentration and the fibrinolytic system. Stroke. 2000. 31: 1256-62
15. Schietroma JJ, Tenzel RR. The effects of cautery on the optic nerve. Ophthalmic Plast Reconstr Surg. 1990. 6: 102-7
16. Tsunoda S, Inoue T, Ono H, Naemura K, Akabane A. Paramedian thalamic infarction caused by cisternal drain placement in open clipping for aneurysmal subarachnoid hemorrhage: Two case reports. Surg Neurol Int. 2020. 11: 164
17. Uberti M, Hasan S, Holmes D, Ganau M, Uff C. Clinical significance of isolated third cranial nerve palsy in traumatic brain injury: A detailed description of four different mechanisms of injury through the analysis of our case series and review of the literature. Emerg Med Int. 2021. 2021: 5550371

