

- Department of Neurology, Weill Cornell Medicine,
- Department of Radiology, Memorial Sloan Kettering Cancer Center, New York City, New York, United States.
Correspondence Address:
Melvin Parasram, Department of Neurology, Weill Cornell Medicine, New York City, New York, United States.
DOI:10.25259/SNI_271_2022
Copyright: © 2022 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, transform, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Melvin Parasram1, Julio Arevalo-Perez2. Cerebral toxoplasmosis in a patient with multiple myeloma. 06-May-2022;13:191
How to cite this URL: Melvin Parasram1, Julio Arevalo-Perez2. Cerebral toxoplasmosis in a patient with multiple myeloma. 06-May-2022;13:191. Available from: https://surgicalneurologyint.com/surgicalint-articles/11581/
Date of Submission
20-Mar-2022
Date of Acceptance
20-Apr-2022
Date of Web Publication
06-May-2022
Abstract
Background: Cerebral toxoplasmosis is a rare complication of relapsed/refractory multiple myeloma (MM) after autologous stem cell transplant (SCT). Imaging characteristics can be helpful in leading to rapid diagnosis and treatment.
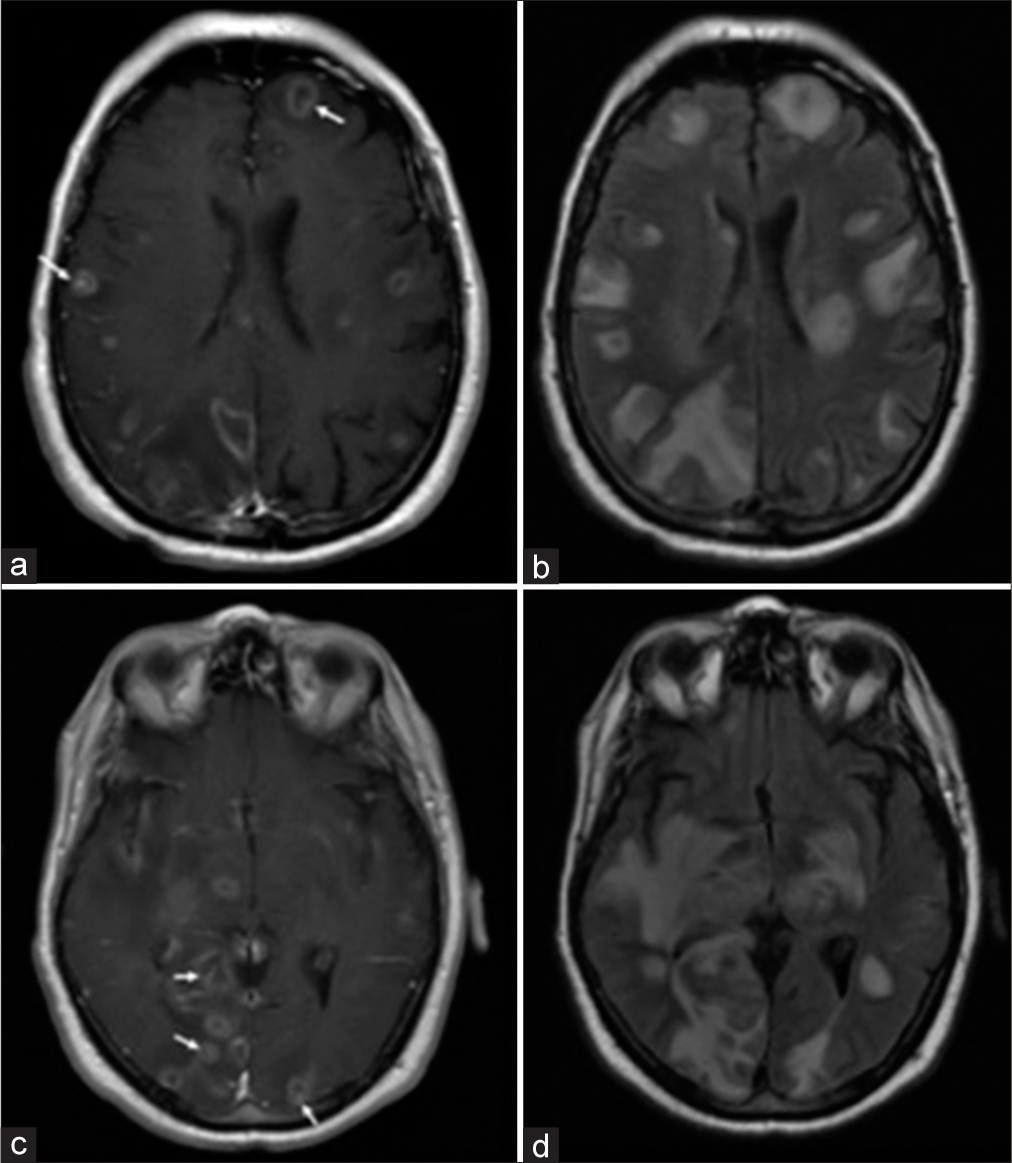
Case Description: A 76-year-old man with relapsed/refractory IgA kappa MM status post autologous SCT who presented to the hospital with altered mental status. His hospital course was complicated by rapid decompensation to obtundation requiring intubation. Magnetic resonance imaging (MRI) of the brain revealed numerous ring-enhancing lesions with eccentric target signs, which were concerning for cerebral toxoplasmosis. Diagnosis was confirmed with positive toxoplasma cerebrospinal fluid polymerase chain reaction test.
Conclusion: Cerebral toxoplasmosis should be considered in the differential diagnosis for MM patients who present with altered mental status and neurologic findings. The ring-enhancing lesion with eccentric target sign on MRI can be helpful in the diagnosis of cerebral toxoplasmosis.
Keywords: Cerebral toxoplasmosis, Eccentric target sign, Multiple myeloma, Neuroimaging, Neuroinfectious disease
IMAGE REPORT
A 76-year-old man with a 6-year history of relapsed/refractory IgA kappa multiple myeloma (MM) presented to the hospital with altered mental status. He was previously treated with chemotherapy, immunomodulating therapy, and autologous stem cell transplantation (SCT), and was actively being treated with carfilzomib, pomalidomide, and dexamethasone for MM. Examination demonstrated inattention and disorientation. Serum laboratory tests were unremarkable. His hospital course was complicated by rapid decompensation to obtundation requiring intubation. Magnetic resonance imaging of the brain (MRI) revealed numerous ring-enhancing lesions with eccentric target signs (arrow), which were radiographically concerning for cerebral toxoplasmosis [
Toxoplasma gondii is a common parasite leading to opportunistic infections in immunosuppressed hosts and is more commonly seen in HIV/AIDS patients. Patients with MM are at an increased risk for infections due to inherent dysfunction of adaptive immunity and from cytotoxic effects of treatment.[
Declaration of patient consent
Patient’s consent not required as patient’s identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Blimark C, Holmberg E, Mellqvist UH, Landgren O, Björkholm M, Hultcrantz M. Multiple myeloma and infections: A population-based study on 9253 multiple myeloma patients. Haematologica. 2015. 100: 107-13
2. Busemann C, Ribback S, Zimmermann K, Sailer V, Kiefer T, Schmidt CA. Toxoplasmosis after allogeneic stem cell transplantation--a single centre experience. Ann Hematol. 2012. 91: 1081-9
3. Kollu V, Magalhaes-Silverman M, Tricot G, Ince D. Toxoplasma encephalitis following tandem autologous hematopoietic stem cell transplantation: A case report and review of the literature. Case Rep Infect Dis. 2018. 2018: 9409121
4. Kumar GG, Mahadevan A, Guruprasad AS, Kovoor JM, Satishchandra P, Nath A. Eccentric target sign in cerebral toxoplasmosis: Neuropathological correlate to the imaging feature. J Magn Reson Imaging. 2010. 31: 1469-72
5. Nucci M, Anaissie E. Infections in patients with multiple myeloma in the era of high-dose therapy and novel agents. Clin Infect Dis. 2009. 49: 1211-25
6. Theologides A, Osterberg K, Kennedy BJ. Cerebral toxoplasmosis in multiple myeloma. Ann Intern Med. 1966. 64: 1071-4
7. Yeung J, van Hal S, Ho PJ. Prolonged immunosuppression in relapsed, refractory multiple myeloma leading to cerebral toxoplasmosis and progressive multifocal leukoencephalopathy. Clin Lymphoma Myeloma Leuk. 2019. 19: e625-8

