

- Department of Neurosurgery, Takashimadaira Central General Hospital, Itabashiku, Tokyo, Japan.
Correspondence Address:
Nobuhiko Arai, Department of Neurosurgery, Takashimadaira Central General Hospital, Itabashiku, Tokyo, Japan.
DOI:10.25259/SNI_252_2022
Copyright: © 2022 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, transform, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Nobuhiko Arai, Kazunari Yachi, Ryutaro Ishihara, Takao Fukushima. Adenomyosis-associated recurrent acute cerebral infarction mimicking Trousseau’s syndrome: A case study and review of literature. 29-Apr-2022;13:179
How to cite this URL: Nobuhiko Arai, Kazunari Yachi, Ryutaro Ishihara, Takao Fukushima. Adenomyosis-associated recurrent acute cerebral infarction mimicking Trousseau’s syndrome: A case study and review of literature. 29-Apr-2022;13:179. Available from: https://surgicalneurologyint.com/surgicalint-articles/11565/
Date of Submission
14-Mar-2022
Date of Acceptance
12-Apr-2022
Date of Web Publication
29-Apr-2022
Abstract
Background: Adenomyosis is a common and benign uterine disease. Acute cerebral infarction (CI) associated with adenomyosis is rarely reported and difficult to treat. We experienced successful treatment for this disease.
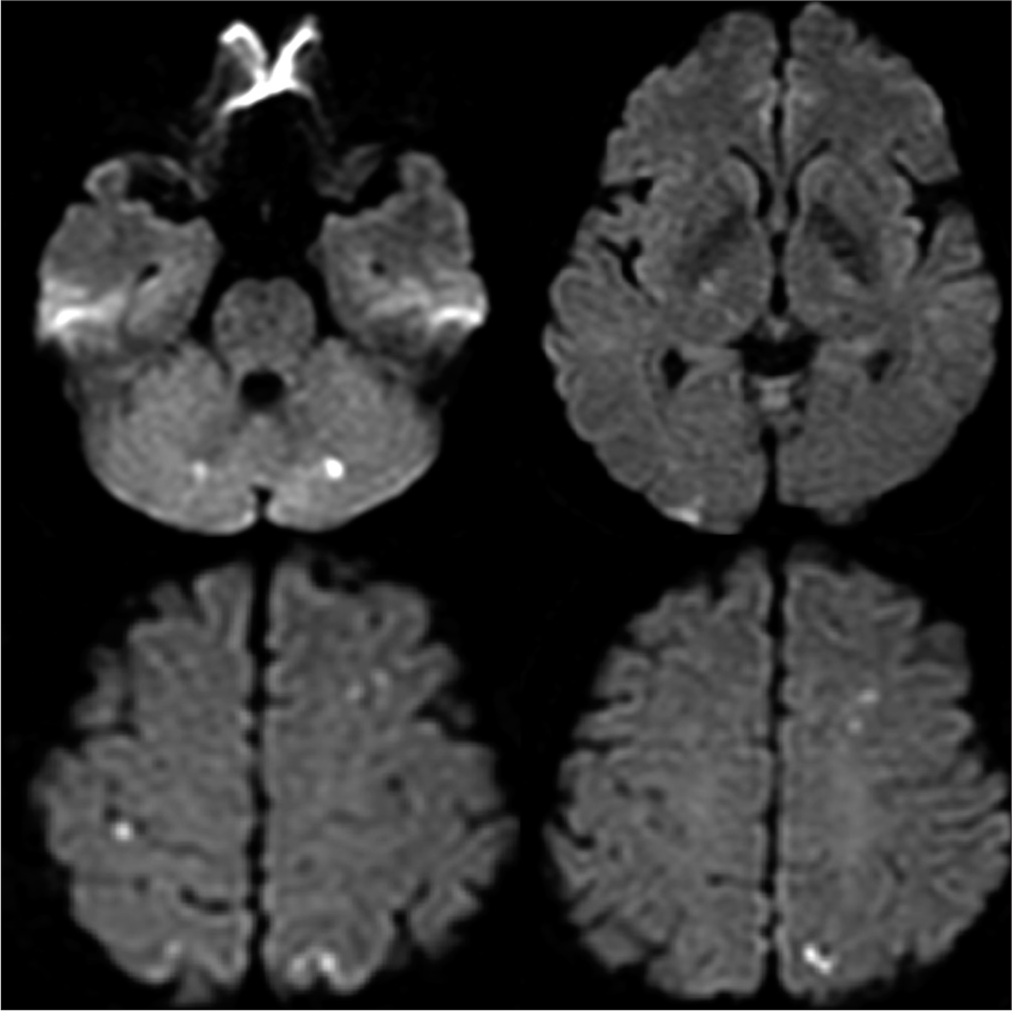
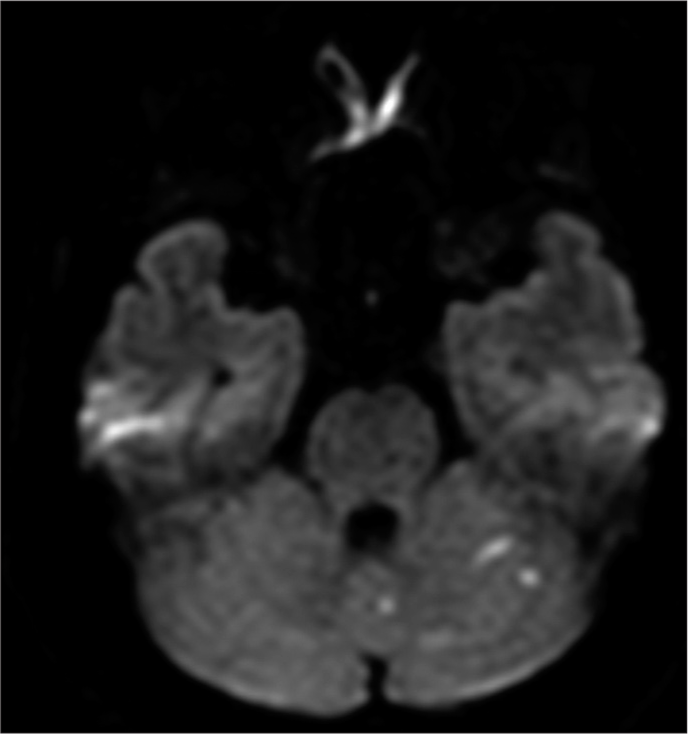
Case Description: A 50-year-old woman presented with a 2-day history of visual disturbance. Magnetic resonance imaging showed multiple tiny diffusion-weighted high-density spots on several lobes. No common risk factors for stroke were detected. Cancer antigen 125 level was 999 U/mL, along with massively expanded uterus and adnexa. Based on the diagnosis of benign adenomyosis, Xa inhibitor and GnRH agonists were administered for CI and adenomyosis, respectively. Acute CI recurred 7 days after admission. We suspected a relationship between infarction and adenomyosis and concluded hysterectomy as a proper treatment strategy based on the literature. Eighteen months after hysterectomy, no recurrence of CI without anti-thrombus medications has been detected.
Conclusion: Hysterectomy is a radical therapy that is effective in preventing acute CI due to adenomyosis associated with ischemic symptoms.
Keywords: Acute cerebral infarction, Adenomyosis, CA125, Hysterectomy, Trousseau’s syndrome
INTRODUCTION
Adenomyosis is a common and benign uterine disease. The formation of uterine glands and stroma in the endometrial membrane is the pathological trait of this disease. This disease presents with abnormal uterine bleeding, pelvic pain, and uterine growth in volume with a prevalence of 20–35% in women.[
CASE REPORT
A 50-year-old woman presented with a 2-day history of visual disturbance that was later identified as left-sided hemianopsia. Magnetic resonance imaging (MRI) revealed multiple acute CIs in almost all lobes [

DISCUSSION
In this case, we experienced acute CI associated with adenomyosis which recurs as early as 7 days after the initial attack under the Xa inhibitor. From this case, we found that Xa inhibitor is not potent enough to prevent recurrence of CI and hysterectomy which assumed to be radical treatment for CI and adenomyosis should be performed within 7 days after the first symptom.
Adenomyosis is relatively common female disease, from which around 20–30% of all woman have suffered in the world.[
The radical treatment for adenomyosis associated with acute CIs must be hysterectomy. The present case showed recurrent CI under the anti-coagulant agents which is Xa inhibitor which would be ideal theoretically. In the past two cases presented recurrent CI under the anti-thrombus medication with GnRH agonists for adenomyosis.[
CONCLUSION
Adenomyosis can lead to the recurrent acute CIs. Hysterectomy could be a radical and appropriate treatment for those condition.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Aiura R, Nakayama S, Yamaga H, Kato Y, Fujishima H. Systemic thromboembolism including multiple cerebral infarctions with middle cerebral artery occlusion caused by the progression of adenomyosis with benign gynecological tumor: A case report. BMC Neurol. 2021. 21: 14
2. Aso Y, Chikazawa R, Kimura Y, Kimura N, Matsubara E. Recurrent multiple cerebral infarctions related to the progression of adenomyosis: A case report. BMC Neurol. 2018. 18: 119
3. Hijikata N, Sakamoto Y, Nito C, Matsumoto N, Abe A, Nogami A. Multiple cerebral infarctions in a patient with adenomyosis on hormone replacement therapy: A case report. J Stroke Cerebrovasc Dis. 2016. 25: e183-4
4. Ishikawa M, Nakayama K, Ishibashi T, Sato E, Nakamura K, Katagiri H. Case series of cerebral infarction with Trousseau’s syndrome associated with malignant gynecological tumors. Mol Clin Oncol. 2016. 5: 138-42
5. Kan YY, Yeh SH, Ng HT, Lou CM. Effect of menstruation on serum CA125 levels. Asia Oceania J Obstet Gynaecol. 1992. 18: 339-43
6. Kim B, Kim SH, Kim T. Cerebral infarcts by nonbacterial thrombotic endocarditis associated with adenomyosis: A case report. J Stroke Cerebrovasc Dis. 2018. 27: e50-3
7. Kim B, Park Y, Kim B, Ahn HJ, Lee KA, Chung JE, Han SW. Diagnostic performance of CA 125, HE4, and risk of ovarian malignancy algorithm for ovarian cance. J Clin Lab Anal. 2019. 33: e22624
8. Okazaki K, Oka F, Ishihara H, Suzuki M. Cerebral infarction associated with benign mucin-producing adenomyosis: report of two cases. BMC Neurol. 2018. 18: 166
9. Raffone A, Seracchioli R, Raimondo D, Maletta M, Travaglino A, Raimondo I. Prevalence of adenomyosis in endometrial cancer patients: A systematic review and meta-analysis. Arch Gynecol Obstet. 2021. 303: 47-53
10. Uchino K, Shimizu T, Mizukami H, Isahaya K, Ogura H, Shinohara K. Nonbacterial thrombotic endocarditis complicated by cerebral infarction in a patient with adenomyosis with high serum CA125 level: A case report. J Stroke Cerebrovasc Dis. 2018. 27: e42-5
11. Varki A. Trousseau’s syndrome: Multiple definitions and multiple mechanisms. Blood. 2007. 110: 1723-9
12. Yamanaka A, Kimura F, Yoshida T, Kita N, Takahashi K, Kushima R. Dysfunctional coagulation and fibrinolysis systems due to adenomyosis is a possible cause of thrombosis and menorrhagia. J Obstet Gynecol Reprod Biol. 2016. 15: 811-24
13. Yamashiro K, Tanaka R, Nishioka K, Ueno Y, Shimura H, Okuma Y. Cerebral infarcts associated with adenomyosis among middle-aged women. J Stroke Cerebrovasc Dis. 2012. 21: 910.e1-5
14. Yasuda M, Yamanaka Y, Kano H, Araki N, Ishikawa H, Ikeda JI. Recurrent cerebral infarcts associated with uterine adenomyosis: Successful prevention by surgical removal. Intern Med. 2022. 1;61: 735-8
15. Yin X, Wu J, Song S, Zhang B, Chen Y. Cerebral infarcts associated with adenomyosis: A rare risk factor for stroke in middle-aged women: A case series. BMC Neurol. 2018. 18: 213
16. Zhao Y, Zhang Y, Yang Y. Acute cerebral infarction with adenomyosis in a patient with fever: A case report. BMC Neurol. 2020. 20: 210

