


Abstract
Background/Aim: Curing local recurrence of rectal cancer (LRRC) is difficult with conventional photon radiotherapy. Proton beam therapy (PBT) on the other hand, has unique physical characteristics that permit higher doses to LRRC while minimizing side effects on surrounding organs. However, the efficacy of PBT on controlling rectal cancer recurrence has not yet been reported. This study aimed to evaluate clinical outcomes and toxicities of PBT for LRRC. Patients and Methods: Clinical outcomes were retrospectively evaluated for 12 patients with 13 total lesions that had received PBT for LRRC at our institute. Results: The median follow-up period from the initiation of PBT was 42.9 months. The 3-year local control, progression-free survival and overall survival rates were 80.2%, 12.1% and 71.3%, respectively. Median survival time was 67.1 months. There were no severe acute or late adverse events. Conclusion: PBT could be a safe and effective treatment method for LRRC.
- Rectal cancer
- local recurrence
- proton beam therapy
- dose escalation
- chemoradiotherapy
- particle beam therapy
In Japan, colorectal cancer was the most common malignancy in 2017 and the second-leading cause of death in 2018 (1). Rectal cancer accounted for about one-third of these, with 51,238 patients in 2017 and 15,244 deaths in 2018 (1). Advances in surgical techniques have decreased the frequency of postoperative local recurrence (LR); however, LR persists in 5-1% of patients even after curative resection of rectal cancer (2). Surgery, especially complete surgical resection (R0 resection), is the only curative treatment for LR of rectal cancer (LRRC) but there are severe complications during and after resection, meaning that few patients with LRRC can undergo R0 resection (3-5). In Japan, surgery for resection is recommended for LRRC only when R0 resection is possible (6).
Some LRRC patients who do not qualify for surgical resection therefore receive radiotherapy, especially for symptoms like bleeding and pain. However, conventional photon radiotherapy at 50.0 Gray (Gy) and 25 fractions is palliative, not curative, as LRRC has very low radiosensitivity (7). In these cases, dose escalation may improve clinical outcomes but close proximity of these tumors to radiosensitive organs like the colon, bladder and small intestine prevent this approach for conventional photon radiotherapy (8).
Proton beam therapy (PBT), on the other hand, has unique physical characteristics, such as the Bragg-Peak, in which the proton beam creates a localized peak in a deep part of the body according to the input energy. Because of this feature, PBT can provide higher doses to LRRC, while minimizing unnecessary irradiation of the surrounding, radiosensitive organs. In recent decades, the efficacy and feasibility of PBT has been reported for diverse cancers such as the liver, esophagus, or pancreas (9-15).
We treated 12 patients with curative PBT in our institute and we report here the results demonstrating the potential effectiveness of PBT for patients with LRRC.
Patients and Methods
Patients. PBT for LRRC was conducted for 12 patients with 13 total lesions between 2003 and 2018 at our institute. Before beginning treatment, LRRC without distant metastasis was verified by computed tomography (CT), magnetic resonance imaging (MRI) and F-18-2-Fluoro-2-deoxy-D- glucose (FDG) positron emission tomography (PET). After curative resection of the primary tumor and regional lymph nodes, rectal adenocarcinoma without gross or microscopic residual disease was confirmed. After the examinations were completed, all cases in which complete resection was difficult were evaluated by surgeons on the cancer board.
As exclusion criteria, patients with an ECOG Performance Status (PS) >2, who had received prior photon or particle radiation therapy to the same site, who had another primary malignancy, or who had an infection at the tumor site were not included in this study.
Proton beam therapy. Before making a treatment plan, CT images without intravenous contrast agent were taken at 2.5 mm intervals for planning. We defined the gross tumor volume as the primary tumor while the clinical target volume (CTV) was judged to be an additional 5 mm margin around the gross tumor volume. Beam-dependent margins, such as a 0.5-1 cm margin around the CTV, were directly added.
Irradiation was performed daily during weekdays and at least 4 days a week, even on holidays. During treatment, all patients were treated with 155-230 MeV proton beams, using a passive spreading method, shaped with ridge filters, double scattering sheets, multi-collimators and a custom-made bolus to ensure that the beams conformed to the planning data. Spinal bones and 2 sets of orthogonal digital radiographs were used for daily positional confirmation.
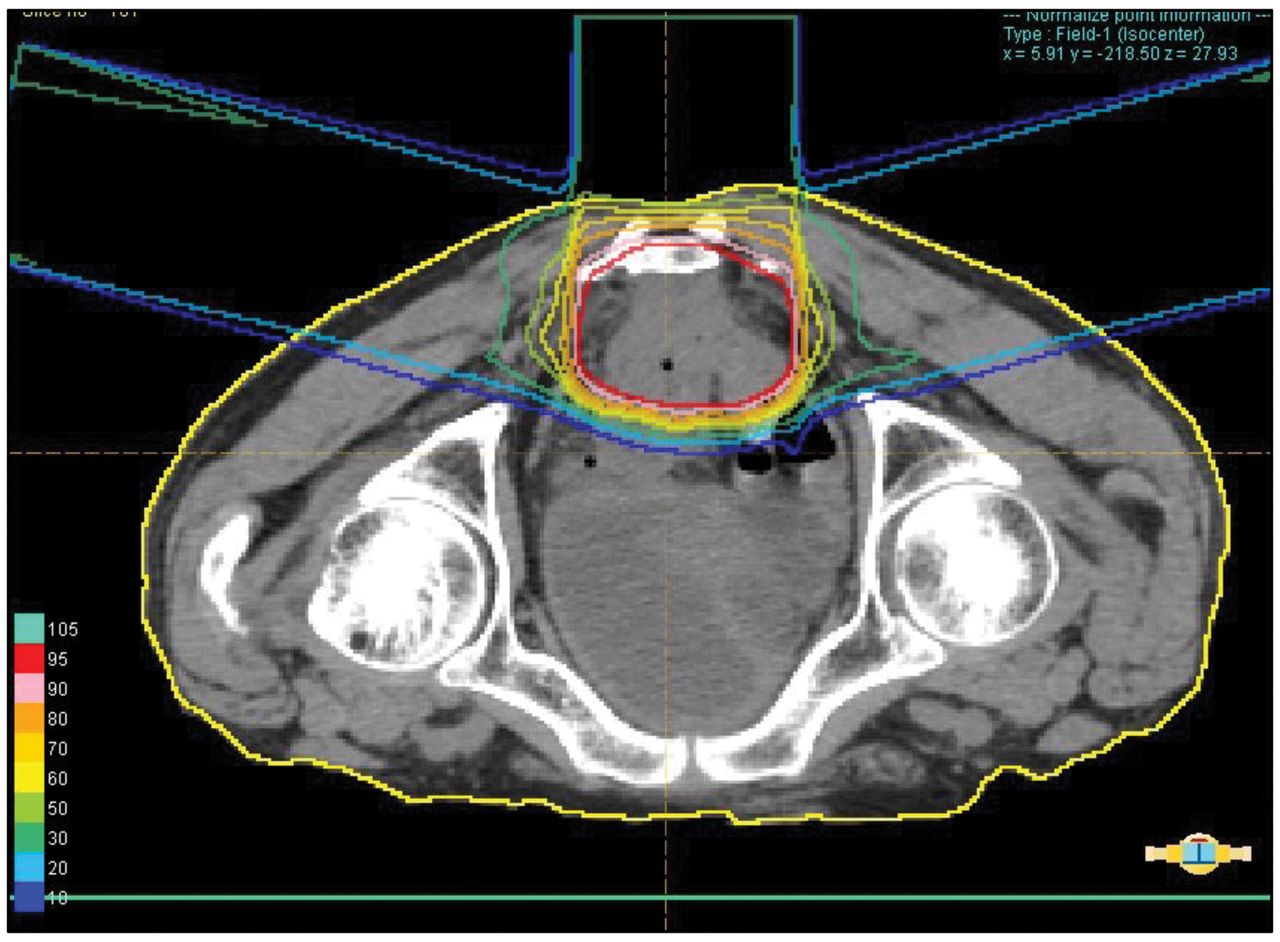
We selected beam fractionations by tumor location, distance between tumors and organs at risk. When the tumors were in the vicinity of high-risk organs, fractional doses were reduced to avoid severe adverse effects. Irradiated doses were calculated by assuming the RBE to be 1.1. Figure 1 depicts a representative case of a LRRC patient and dose distribution of PBT at a total dose of 75 GyE in 25 fractions.
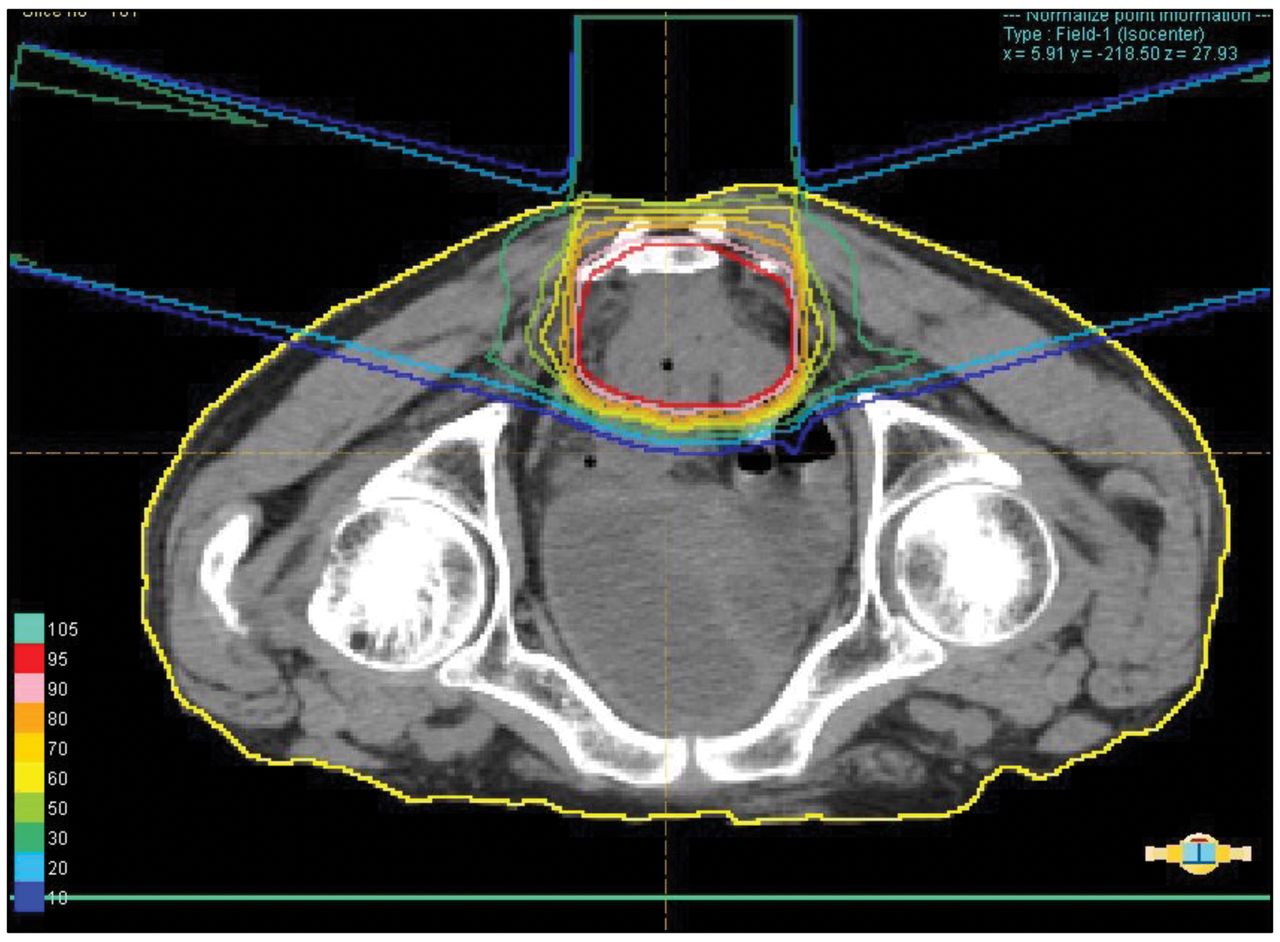
Dose distribution of proton beam therapy for sacral anterior LRRC at a total dose of 75 GyE in 25 fractions. The supine position resulted in the gantry being closer to the lesion and further improved the dose distribution.
Concurrent chemotherapy. Six of 13 patients in this analysis received concurrent S-1 (combination of Tegafur, Gimeracil and Oteracil). Oral S-1 was prescribed twice daily, but only on the day of irradiation, according to body-surface area (<1.25 m2, 80 mg/day; >1.25 to <1.5 m2, 100 mg/day; >1.5 m2, 120 mg/day), and was skipped when the absolute granulocyte count was less than 2,000/mm3 or the platelet count was less than 70,000/mm3 on a scheduled dosage day, in cases of poor performance status, abnormal biochemical data, or in the presence of any diagnosed condition that contraindicated administration.
Others were treated solely by PBT if S-1 or fluorouracil was ineffective in a previous treatment cycle or the gastrointestinal tract was in close proximity.
Follow-up procedure. During PBT treatment, acute treatment-related toxicities and treatment efficacies were evaluated once or twice per week in all patients. All patients were scheduled for examination every 3 months and physical condition, blood sampling and imaging were conducted prior to their visits if their physical condition was good after completing PBT. If the patients were unable to visit our institute due to the traveling distance or a poor general condition, follow up of imaging and blood tests was performed at a nearby institute and the results were sent to our hospital. Adjuvant therapy after PBT was done at the discretion of the attending physician in accordance with individual physical condition.
Evaluation and stastical analysis. Acute and late toxicities were evaluated according to the National Cancer Institute Common Terminology Criteria for Adverse Events (CTCAE, version 4.0) (16) while relapse was evaluated according to the Response Evaluation Criteria in Solid Tumors (RECIST, version 1.1) (17). We examined overall survival (OS), progression free survival (PFS), and local control (LC) rates using the Kaplan–Meier method. All analyses were performed using SPSS version 25.0 (IBM Inc. Armonk, NY, USA).
Ethics. All procedures involving human participants, including case reviews of treatments, were conducted in accordance with the ethical standards of the 1964 Declaration of Helsinki and its later amendments and approved by the University of Tsukuba Institutional Research Committee (Approval #R01-230). All treatments were discussed at an in-hospital conference consisting of surgeons, internists and radiologists; informed consent was obtained from all participants included in the study. We got informed consent from either living patients themselves or legally designated next-of-kin where appropriate.
Results
Patient characteristics. From 2001 to 2018, 12 patients with 13 total LRRC lesions were included. Six of 13 patients in this analysis were treated by curative chemotherapy concurrent with PBT while the remaining 7 received only PBT and all patients completed their scheduled treatments. Patient characteristics are summarized in Table I. The median age was 69 years (range=38-77 years) and all patients were male. Relapse locations included the presacral region (n=12) and pelvic side walls (n=1). The median tumor size was 63 mm (range=20-131 mm). The median time from surgery to LR was 23.5 months (range=2.1-89.3 months). Total irradiated doses and fractionations are summarized in Table II.
Characteristics of patients and tumors.
Characteristics of treatment plans.
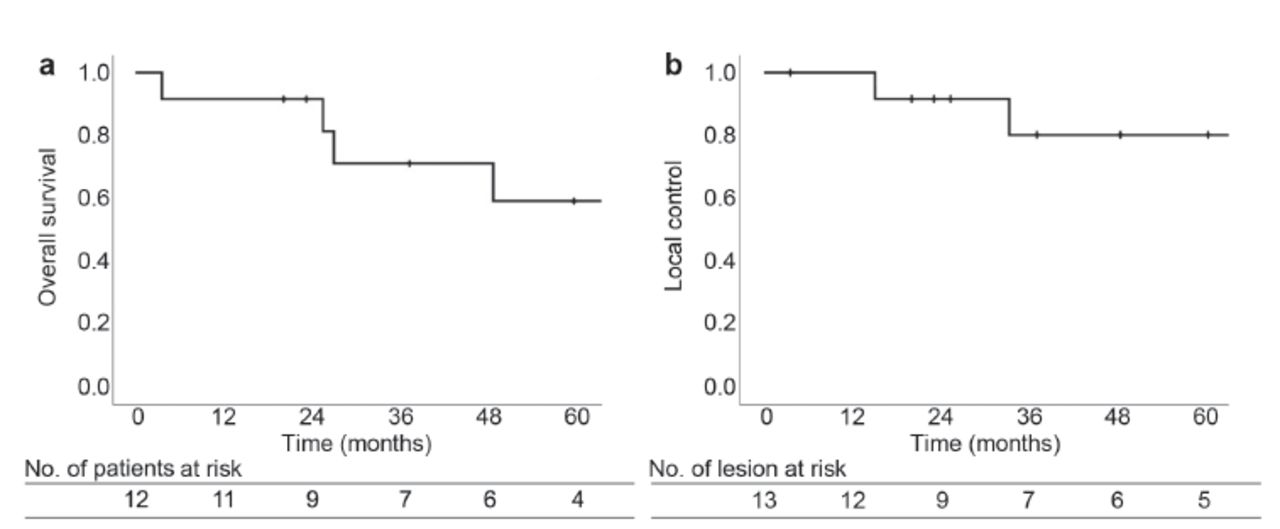
Treatment outcomes. The median follow-up period from the initiation of PBT was 42.9 months (range=3.6-102.6 months). As of November 2020, a total of 6 patients had died of rectal cancer. Recurrence after PBT was observed in 10 patients (83.3%), of whom 2 (16.7%) had a LR, 7 (58.3%) had distant metastasis and 1 (8.3%) had both. The 3-year LC, PFS and OS rates were 80.2% [95% confidence interval (CI)=55.1-100%], 12.1% (95% CI=0-33.7%) and 71.3% (95% CI=43.7-98.9%), respectively. Median survival time was 67.1 months (95% CI=24.0-110.2 months) (Figure 2).
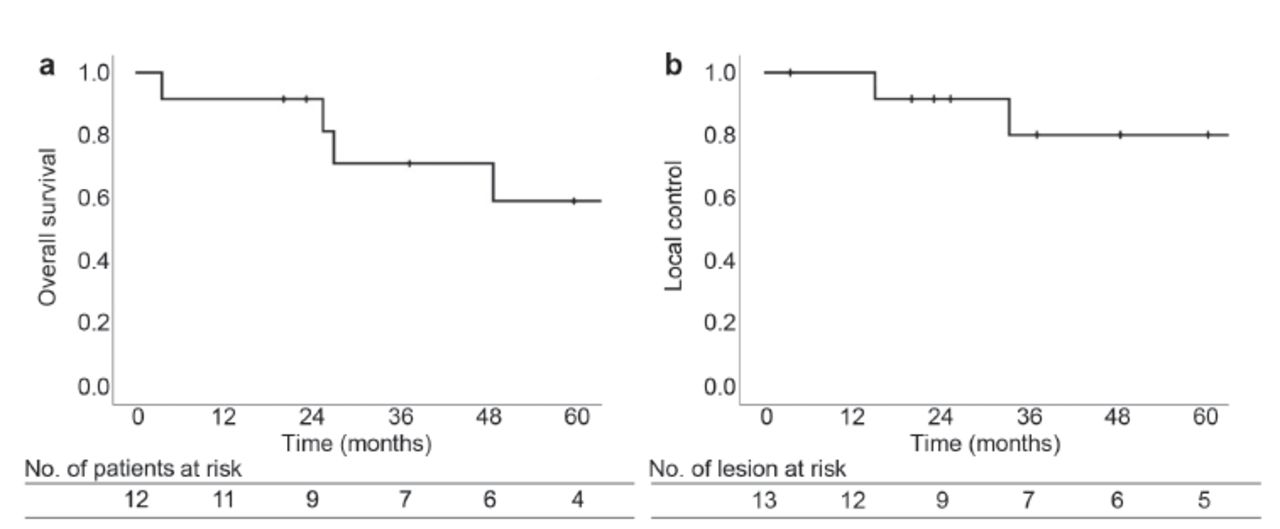
Kaplan-Meier estimates of (a) overall survival (OS) and (b) local control (LC) rates from the initiation of proton beam therapy.
Toxicities. Treatment-related toxicities are described in Table III. No grade >2 acute or late adverse events were observed over the follow-up time period.
Treatment-related acute and late adverse events.
Discussion
In our study, the 3-year OS and LC rates were 71.3% and 80.2%. Although from a small population, these results were encouraging since the enrolled patients were not suitable for radical resection.
Westberg et al. showed some factors that influence death risk after curative treatment for LRRC from a large population-based national patient cohort with long follow up (18). They reported that patients aged 80 years and over, with stage III primary tumors, symptoms, hydronephrosis, or a non-central LRRC were at a significant high risk with regards to curative surgery. In our study, 8 of 12 patients were at a primary tumor stage of more than III and this fact suggests that particle beam therapy may be safe and effective in some of these cases.
It could be hard to achieve R0 resection in LRRC that have infiltrated the pelvic side or posterior wall as centrally located LRRC, because they tend to invade organs at risk such as the gastrointestinal tract and bladder. As a result, centrally located LRRC with a good indication for surgery tends to not be recommended for PBT in order to limit dose escalation around organs at risk. On the other hand, since a non-centrally located LRRC tends to be distant from organs at risk, this may be a good indication for PBT when taking into account the risks of mortality and morbidity following curative surgery. In our study, although 11 of 13 lesions were located centrally, there were no serious acute or late adverse events. We tried to administer treatment plans that had been redesigned several times to deliver the highest possible dose to the LRRC while suppressing exposure to at-risk organs, thereby helping to alleviate severe adverse events.
Photon radiotherapy is sometimes suggested for patients who are not suitable for surgical resection, but radiosensitive organs around the tumor make sufficient curative doses difficult even with high-precision radiotherapy techniques such as intensity modulated radiotherapy (IMRT). Tanaka et al. reported that 3-year OS and LC rates with 3-dimensional conformal radiotherapy were 45.2% and 19.6% and found that doses higher than the biological effective dose (BED) of 75Gy brought better clinical outcomes (7). However, this exceeds the tolerable dose for risk organs, such as the gastrointestinal tract, and would increase the frequency of serious adverse events like perforation. Although achieving therapeutically sufficient doses is sometimes difficult for photon radiotherapy, particle beam therapy may more easily achieve clinical goals due to the Bragg Peak effect. In fact, no serious adverse effects were observed in all 10 patients given at > BED of 75 Gy in our study.
Proton beam therapy for LRRC has been reported in a small number of cases; Lee et al. performed PBT on 4 of 67 LRRC patients (19). Although there are no reports on the results of PBT, they noted that they were able to prescribe high doses for patients with very close to organs at risk, such as small bowel. Hamauchi et al. reported the results of PBT in 13 LRRC patients with 70 GyE (20). With median LC and PFS of 504 and 404 days, respectively, and only one patient with a Grade 3 adverse event, they suggested that PBT may be a treatment option for LRRC due to good local control and low incidence of serious adverse events. Berman et al. reported the outcomes of PBT in 7 LRRC patients with prior irradiation and the dose distribution compared to IMRT (21). The average prescribed dose of PBT was 61.2 GyE, with complete response and progressive disease in 1 patient each and partial response in 7 patients. In terms of dose distribution, PBT was significantly better than IMRT, especially in avoiding the small intestine. All these reports with PBT are consistent with the present report, as they safely delivered high doses to the LRRC while lowering the dose delivered to the gastrointestinal tract.
There are some reports of carbon-ion radiation therapy (CIRT) for LRRC. CIRT is a particle beam therapy and is characterized by high BED (22). Yamada et al. reported a phase 1/2 dose escalation study (23) where the 3-year and 5-year OS rates were 72% and 53%. In phase I, they demonstrated that 73.6 Gy (RBE: Relative Biological Effect weighted absorbed dose) in 16 fractions was better and carried this over to a phase 2 study. Shinoto et al. reported a multi-institutional study of CIRT on LRRC in which three CIRT institutions in Japan were included (24). From a total number of 224 patients, they reported 3-year and 5-year OS of rates 73% and 51%. They also reported that grade 3 acute toxicities were observed in 3 (1%) of the 224 patients (1 gastrointestinal reaction and 2 pelvic abscesses) while grade 3 late toxicities were observed in 12 patients (5%) (2 skin reactions, 2 gastrointestinal reactions, 1 peripheral nerve reaction and 7 pelvic abscesses). Most patients received 73.6 Gy (RBE) in 16 fractions and, as their results were very similar to the study by Yamada et al., these reports point to better clinical outcomes and lower toxicity than conventional photon radiotherapy.
With regard to biological effects, PBT is similar to photon beam therapy (25) in that more dose escalation may result in better clinical outcomes, as seen in CIRT studies; however, even PBT may face positioning difficulties between tumor and gastrointestinal tract locations. To improve clinical outcomes, local hyperthermia is an option as it is known to heat tumors, increasing the blood supply and improving delivery of large doses of oxygen and drugs to tumors and enhancing the effects of radiotherapy (26, 27). It also has a function as a radiation- and chemo-sensitizer while inhibiting transcription factors (28). Because LRRC is characterized by chemo-and radio- resistance and hypoxia, these patients are presumably well adapted for combination of hyperthermic therapy with lower linear energy transfer radiation such as PBT (29). Thus, we have recently started concomitant use of hyperthermia in PBT for LRRC to improve outcomes. Due to the short accumulation period and the small number of patients, reports from our institute on this promising effect remain forthcoming.
Another solution to improve clinical outcomes is a surgical spacer. The method of using a tissue expander for the spacer has been reported for a long time, but these need to be removed after irradiation. Kemmochi et al. reported on experiences of surgical spacer placement using polytetrafluoroethylene and polyurethane (30), pointing out that artificial objects adhere to the digestive tract and damage it due to friction after a long insertion period. Akasaka et al. reported on the efficacy and safety of making distance between the tumor and the at-risk organ by using a nonwoven spacer produced with a biocompatible, synthetic polymeric material called polyglycolic acid (PGA) (31). The characteristic of these spacers is that the size does not change for 8 weeks and is gradually absorbed from about 12 weeks with no toxicity, including no C-reactive protein (CRP) elevation and no liver or renal dysfunction. Since 2019, this spacer can be used for particle beam therapy within the national insurance system of Japan and it is expected that spacer-enabled higher doses can be administered, thereby increasing the number of treatable LRRC patients.
There are some limitations to this study, including the retrospective design, small patient population and possible selection bias. Additionally, we did not compare PBT with photon radiotherapy and CIRT directly; therefore, it is unclear how much better PBT actually is. However, we found good local control and overall survival without severe adverse effects by using PBT for LRRC. These results suggest that PBT could be an effective and safe definitive therapy for LRRC.
Conclusion
Our result showed that PBT for LRRC resulted in longer survival and better local control than previously reported photon radiotherapy without any severe adverse events. Therefore, PBT could be a safe and effective treatment method for LRRC.
Acknowledgements
The Authors would like to thank Dr. Bryan J. Mathis of the University of Tsukuba Medical English Communications Center for language revision. This work was partially supported by Grants-in-Aid for Scientific Research (B) (19H03596) from the Ministry of Education, Culture, Sports, Science and Technology of Japan.
Footnotes
This article is freely accessible online.
Authors’ Contributions
Conceptualization, Y.H. and H.S.; methodology, Y.H.; formal analysis, M.M. (Motohiro Murakami); investigation, Y.H. and H.I.; resources, M.N.; data curation, S.S.; writing—original draft preparation, Y.H.; writing – review and editing, H.I. and M.M. (Masashi Mizumoto); visualization, K.N.; supervision, T.O. (Toshiyuki Okumura) and T.E.; project administration, H.S. and T.O. (Tatsuya Oda). All authors have read and agreed to the published version of the manuscript.
Conflicts of Interest
The Authors declare no conflicts of interest.
- Received February 4, 2021.
- Revision received May 24, 2021.
- Accepted May 26, 2021.
- Copyright © 2021 International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved.





{kind=link}
{kind=link}