
Summary
The costs of digoxin toxicity to the US healthcare system have not been previously reported. Therefore, the 1994 database of the US University Health-System Consortium (UHC) was searched for cases of digoxin toxicity using the International Classification of Diseases (9th edition) [ICD-9] codes. In addition, the medical records of 17 patients admitted to the University of Illinois Hospital from September 1994 to July 1995 with a diagnosis of digoxin toxicity were also reviewed.
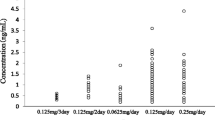
Of the 17 patients, 14 were admitted with a primary diagnosis of digoxin toxicity. Causes of digoxin toxicity were worsening renal function (6 patients), excessive dosage prescribed (4 patients), excessive dosage self-administered (2 patients), multiple prescriptions (2 patients), accidental ingestion (1 patient), drug-drug interaction (1 patient) and unknown (1 patient). Digoxin toxicity could have been prevented in 9 (53%) of the 17 patients.
The mean length of stay in the hospital as a result of digoxin toxicity was 3.3 ± 1.2 days. The mean laboratory cost associated with digoxin toxicity was $US275.54 ± $US106.57 and the mean hospital bed cost was $US3781.92 ± $US2572.22. The mean overall cost associated with digoxin toxicity was $US4087.05 ± $US2659.76. There was a significant correlation between the total cost associated with digoxin toxicity and the serum digoxin concentration on admission (r = 0.73, p < 0.01).
From the UHC database, a total of 836 cases of digoxin toxicity in 56 hospitals were identified. This represented the occurrence of digoxin toxicity in 0.07% of all patients admitted to these US academic hospitals.
Digoxin toxicity results in considerable costs to the healthcare system. Most cases can be considered readily preventable with proper patient counselling and education.
Similar content being viewed by others
References
Hurwitz N, Wade OL. Intensive hospital monitoring of adverse reactions to drugs. BMJ 1969; 1: 531–6
Litovitz TL, Feiberg L, White S, et al. 1995 annual report of the American Association of Poison Control Centers toxic exposure surveillance system. Am J Emerg Med 1996; 14: 487–537
Ekins BR, Watanabe AS. Acute digoxin poisonings: review of therapy. Am J Hosp Pharm 1978; 35: 268–77
Bootman JL, Townsend RJ, McGhan WF, editors. Principles of pharmacoeconomics. Cincinnati (OH): Harvey Whitney Books Co., 1991
International Classification of Diseases (ICD.9.CM). Clinical modification. 5th ed. Los Angeles (CA): Practice Management Information Corp., 1996
Jelliffe RW. An improved method of digoxin therapy. Ann Intern Med 1968; 69: 703–17
Cockcroft DW, Gault MH. Prediction of creatinine clearance from serum creatinine. Nephron 1976; 16: 31–41
Kernan WN, Castellsague J, Perlman GD. Incidence of hospitalization for digitalis toxicity among elderly Americans. Am J Med 1994; 96: 426–31
Roberts SA, Diaz C, Nolan PE, et al. Effectiveness and costs of digoxin treatment for atrial fibrillation and flutter. Am J Cardiol 1993; 72: 567–73
Mauskopf JA, Wenger TL. Cost-effectiveness analysis of the use of digoxin immune Fab (ovine) for the treatment of digoxin toxicity. Am J Cardiol 1991; 68: 1709–14
Mahdyoon H, Battilana G, Rosman H, et al. The evolving pattern of digoxin intoxication: observations at a large urban hospital from 1980 to 1988. Am Heart J 1990; 120: 1189–94
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Gandhi, A.J., Vlasses, P.H., Morton, D.J. et al. Economic Impact of Digoxin Toxicity. Pharmacoeconomics 12, 175–181 (1997). https://doi.org/10.2165/00019053-199712020-00007
Published:
Issue Date:
DOI: https://doi.org/10.2165/00019053-199712020-00007