
Abstract
Background: Atomoxetine is a highly specific presynaptic inhibitor of the noradrenaline (norepinephrine) transporter that was recently approved in the US for the treatment of patients with attention-deficit/hyperactivity disorder (ADHD). Adverse effects on the cardiovascular system, including abnormalities in heart rate, blood pressure, or cardiac rhythm have been associated with several noradrenergic medications.
Objective: To further elucidate the magnitude and impact of blood pressure and pulse elevations in patients taking atomoxetine.
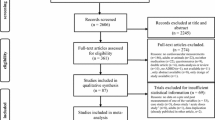
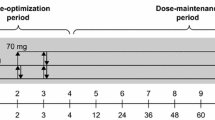
Study Design: Short-term cardiovascular safety in children, adolescents, and adults with ADHD was assessed in five randomised, double-blind trials (duration up to 10 weeks) with atomoxetine (n = 612) or placebo (n = 474). Long-term cardiovascular safety in children and adolescents (n = 169) was assessed in patients who entered an open-label extension or a blinded continuation following short-term treatment.
Methods: Adverse events, blood pressure, sitting pulse, and electrocardiograms (ECGs) were collected throughout the trials. QT intervals were corrected for heart rate by a data-specific correction factor (QTcD; derived from baseline ECGs) as well as standard methods.
Results: Atomoxetine treatment was associated with small but statistically significant increases in mean systolic blood pressure in adults and diastolic blood pressure in children and adolescents. Mean pulse rate increased for all atomoxetine treatment groups. The increases in blood pressure and pulse tended to occur early in therapy, stabilised, and returned toward baseline upon drug discontinuation. There was no significant difference between atomoxetine and placebo treatment groups in change in QTcD interval for all study populations. Palpitations in the adult patient population were the only significant cardiovascular adverse event (p = 0.037) occurring more frequently in the atomoxetine treatment group (3.7%) than in the placebo group (0.8%). Discontinuations due to cardiovascular-related events were very uncommon in the adult group, and did not occur in the child/adolescent group.
Conclusion: While atomoxetine has noradrenergic activity, increases in pulse and blood pressure were small and of little, if any, clinical significance. Atomoxetine was not associated with QT interval prolongation. Cardiovascular effects of atomoxetine were minimal, and atomoxetine was well tolerated in short- and long-term studies.











Similar content being viewed by others

References
Michelson D, Faries DE, Wernicke J, et al. Atomoxetine in the treatment of children and adolescents with attention-deficit/hyperactivity disorder: a randomized, placebo-controlled, dose-response study. Pediatrics 2001; 108(5): e83
Michelson D, Allen AJ, Busner J, et al. Once-daily atomoxetine treatment for children and adolescents with attention-deficit/hyperactivity disorder: a randomized, placebo-controlled study. Am J Psychiatry 2002; 159(11): 1–6
Spencer T, Heiligenstein J, Biederman J, et al. Results from 2 proof-of-concept, placebo-controlled studies of atomoxetine in children with attention-deficit/hyperactivity disorder. J Clin Psychiatry 2002; 63(12): 1140–7
Newcorn J. Efficacy trials of atomoxetine for ADHD in children, adolescents and adults [abstract 40B]. 49th Annual Meeting American Academy of Child and Adolescent Psychiatry; 2002 Oct 25: San Francisco (CA): 66
Michelson D, Adler L, Spencer T, et al. Atomoxetine in adults with ADHD: two randomized, placebo-controlled studies. Biol Psychiatry 2003; 53: 112–20
Biederman J, Faraone SV, Mick E, et al. Clinical correlates of ADHD in females: findings from a large group of girls ascertained from pediatric and psychiatric referral sources. J Am Acad Child Adolesc Psychiatry 1999; 38(8): 966–75
Wernicke JF, Allen AJ, Faries D, et al. Safety of tomoxetine in clinical trials [abstract]. In: 56th Society of Biological Psychiatry Annual Meeting; 2001 May 3-5; New Orleans (LA). Biol Psychiatry 2001; 49(8 Suppl.): 159S
Thase ME. Effects of venlafaxine on blood pressure: a metaanalysis of original data from 3744 depressed patients. J Clin Psychiatry 1998; 59(10): 502–8
Haller CA, Benowitz NL. Adverse cardiovascular and central nervous system events associated with dietary supplements containing ephedra alkaloids. N Engl J Med 2000; 343(25): 1833–8
Bravo EL. Phenylpropanolamine and other over-the-counter vasoactive compounds. Hypertension 1988; 11(3 Pt 2): II7–10
Angrist B, Sanfilipo M, Wolkin A. Cardiovascular effects of 0.5 milligrams per kilogram oral d-amphetamine and possible attenuation by haloperidol. Clin Neuropharmacol 2001; 24(3): 139–44
Brauer LH, Ambre J, De Wit H. Acute tolerance to subjective but not cardiovascular effects of d-amphetamine in normal, healthy men. J Clin Psychopharmacol 1996; 16(1): 72–6
National High Blood Pressure Education Program Working Group. Update on the task force report (1987) on high blood pressure in children and adolescents: a working group report from the national high blood pressure education program. Bethesda (MD): National Institutes of Health, National Heart, Lung, and Blood Institute; 1996 Sep. Report no.: 96–3790
Committee for Proprietary Medicinal Products. The assessment of the potential for QT interval prolongation by non-cardiovascular medicinal products. London: The European Agency for the Evaluation of Medicinal Products, Human Medicines Evaluation Unit; 1997 Dec 17. Report no.: CPMP/986/96
Funck-Brentano C, Jaillon P. Rate-corrected QT interval: techniques and limitations. Am J Cardiol 1993; 72(6): 17B–22B
Acknowledgements
Research was funded by Eli Lilly and Company.
Drs Girod, Lipetz, and Quintana, have acted as paid consultants and/or investigators for studies sponsored by Eli Lilly and Company. Drs Wernicke, Michelson, Faries, Gao, Kelsey, Heiligenstein and Mr Brown are employees and shareholders of Eli Lilly and Company.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Wernicke, J.F., Faries, D., Girod, D. et al. Cardiovascular Effects of Atomoxetine in Children, Adolescents, and Adults. Drug-Safety 26, 729–740 (2003). https://doi.org/10.2165/00002018-200326100-00006
Published:
Issue Date:
DOI: https://doi.org/10.2165/00002018-200326100-00006