
Abstract
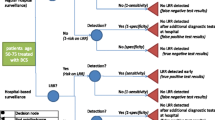
OBJECTIVE: Increased recall rates in the Dutch breast cancer screening program call for a new assessment strategy aiming to reduce unnecessary costs and anxiety. Diagnostic work-up (usual care) includes multidisciplinary hospital assessment and is similar for all recalled women, regardless of the radiologist’s suspicion of breast cancer. This is similar in many Canadian settings. We developed a novel assessment strategy that offers women with a low suspicion of breast cancer a quick and non-invasive assessment by a screening radiologist (intervention). We compared these two strategies in a cost-effectiveness analysis based on a randomized controlled trial: multicentre randomized controlled trial (MASS trial, Netherlands National Trial Register: NTR1480).
METHODS: Participants were enrolled between August 2010 and December 2012 and were randomly assigned to either the intervention or control group (allocation ratio 2:1). Fourteen assessment centres participated in the study. Questionnaires were used to record quality of life (EuroQol-5D), health care use and costs after recall.
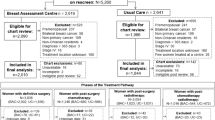
RESULTS: Our study comprised 366 women, of whom 288 were randomly assigned to the intervention group and 88 to the control group. The mean difference in cost was €153/CAD $226 (95% confidence interval €107–199/CAD $158–294, p<0.001). We found no significant differences in quality of life. The bootstrapped incremental cost-effectiveness ratios in the cost-effectiveness plane showed that the intervention was the efficient, cost-saving modality.
CONCLUSION: Our data show the benefits of tailoring diagnostic assessment to the screening radiologist’s suspicion of breast cancer. Scenarios of implementing such a strategy in the Dutch screening or health care system are currently being discussed with various stakeholders.
Résumé
OBJECTIF : Les taux de rappel accrus dans le programme néerlandais de dépistage du cancer du sein requièrent une nouvelle stratégie d’évaluation des patientes pour réduire les coûts et l’anxiété inutiles. L’investigation diagnostique (les soins habituels) inclut une évaluation multidisciplinaire à l’hôpital; le processus est le même pour toutes les femmes rappelées, peu importe si le radiologiste soupçonne ou non un cancer du sein. Il en va de même dans de nombreux établissements au Canada. Nous avons élaboré une stratégie d’évaluation novatrice qui offre aux femmes pour lesquelles la présomption de cancer du sein est faible une évaluation rapide et non invasive par un médecin radiologiste (intervention). Nous avons comparé ces deux stratégies à la faveur d’une analyse coût-avantage fondée sur un essai comparatif randomisé multicentrique (essai MASS, registre national d’essais des Pays-Bas: NTR1480).
MÉTHODE : Les participantes ont été recrutées entre août 2010 et décembre 2012 et réparties de façon aléatoire entre le groupe d’intervention et un groupe témoin (ratio de répartition 2:1). Quatorze centres d’évaluation ont participé à l’étude. Des questionnaires ont été administrés pour enregistrer la qualité de vie (EuroQol-5D), l’utilisation des soins de santé et les coûts après le rappel.
RÉSULTATS : Notre étude comprenait 366 femmes, dont 288 ont été affectées de façon aléatoire au groupe d’intervention et 88 au groupe témoin. La différence moyenne de coût était de 153 €/226 $CAN (intervalle de confiance de 95%: 107-199 €/158-294 $CAN, p<0,001). Nous n’avons trouvé aucune différence significative dans la qualité de vie. Les ratios coût-efficacité incrémentiels (selon la méthode bootstrap) indiquent que l’intervention est la méthode la plus efficiente et économique.
CONCLUSION : Nos données montrent les avantages d’adapter l’évaluation diagnostique selon que le médecin radiologiste qui effectue le dépistage soupçonne ou non un cancer du sein. On discute actuellement avec divers acteurs du milieu de scénarios de mise en œuvre d’une telle stratégie dans le système néerlandais de dépistage ou de soins de santé.
Similar content being viewed by others

References
Statistics Netherlands. Access to StatLine: Make your own tables. 2010/12/01/2010. Available at: http://www.cbs.nl/nl-NL/menu/cijfers/statline/zelf-tabellen-maken/default.htm (Accessed October 1, 2014).
Canadian Cancer Society, Statistics Canada. Canadian Cancer Statistics 2013. Toronto, ON, 2013.
Canadian Partnership Against Cancer. Organized Breast Cancer Screening Programs in Canada: Report on Program Performance in 2007 and 2008. Toronto, 2013.
The benefits and harms of breast cancer screening: An independent review. Lancet 2012;380(9855):1778–86.
Nationaal Borstkanker Overleg Nederland. National Guideline “Breast Cancer”. Amsterdam, 2011.
Statistics Netherlands. Population Pyramid - Age composition in the Netherlands. 2012. Available at: http://www.cbs.nl/nl-nl/menu/themas/ bevolking/cijfers/extra/piramide-fx.htm (Accessed August 1, 2012).
National Evaluation Team for Breast Cancer Screening. National evaluation of breast cancer screening in the Netherlands (1990-2011/2012), thirteenth evaluation report. Rotterdam: NETB, 2014.
Timmers JM, den Heeten GJ, Adang EM, Otten JD, Verbeek AL, Broeders MJ. Dutch digital breast cancer screening: Implications for breast cancer care. Eur J Public Health Epub 2011 Dec 8..
Borugian MJ, Kan L, Chu CC, Ceballos K, Gelmon KA, Gordon PB, et al. Facilitated “fast track” referral reduces time from abnormal screening mammogram to diagnosis. Can J Public Health 2008;99(4):252–56.
Holland R, Rijken HJ, Hendriks JH. The Dutch population-based mammography screening: 30-years experience. Breast Care 2007;2:12–18.
Otten JD, van Dijck JA, Peer PG, Straatman H, Verbeek AL, Mravunac M, et al. Long term breast cancer screening in Nijmegen, The Netherlands: The nine rounds from 1975–92. J Epidemiol Community Health 1996;50(3):353–58.
Fracheboud J, de Koning HJ, Boer R, Groenewoud JH, Verbeek AL, Broeders MJ, et al. Nationwide breast cancer screening programme fully implemented in The Netherlands. Breast 2001;10(1):6–11.
American College of Radiology. ACR practice guideline for the performance of screening and diagnostic mammography (2008). Preston, VA, 2008.
American College of Radiology. ACR BI-RADS®-Mammography: Breast Imaging Reporting and Data System, Breast Imaging Atlas. Preston, 2003.
Timmers JM, van Doorne-Nagtegaal HJ, Zonderland HM, van Tinteren H, Visser O, Verbeek AL, et al. The Breast Imaging Reporting and Data System (BI-RADS) in the Dutch breast cancer screening programme: Its role as an assessment and stratification tool. Eur Radiol 2012;22(8):5.
EuroQol Group. EuroQol-a new facility for the measurement of health-related quality of life. Health Policy 1990;16(3):9.
The Social and Economic Council of the Netherlands. Costs and benefits of healthcare renewal, 2006. Available at: http://www.seo.nl/uploads/media/916_Kosten_en_baten_van_zorgvernieuwing.pdf (Accessed October 6, 2014).
Statistics Netherlands. Statline, consumer price index. 2013. Available at: http://statline.cbs.nl/StatWeb/publication/?VW=T&DM=SLNL&PA=71311ned&D1=0-1,4-5&D2=0&D3=a&HD=080521-1622&HDR=G1,T&STB=G2 (Accessed June 20, 2013).
Lamers LM, Stalmeier PF, McDonnell J, Krabbe PF, van Busschbach JJ. [Measuring the quality of life in economic evaluations: the Dutch EQ-5D tariff]. Ned Tijdschr Geneeskd 2005;149(28):1574–78.
Atkinson KE. An Introduction to Numerical Analysis, 2nd ed. New York: John Wiley & Sons, 1989.
Moher D, Hopewell S, Schulz KF, Montori V, Gotzsche PC, Devereaux PJ, et al. CONSORT 2010 explanation and elaboration: Updated guidelines for reporting parallel group randomised trials. Int J Surg 2012;10(1):28–55.
Blane CE, Pinsky RW, Joe AI, Pichan AE, Blajan MR, Helvie MA. Costs of achieving high patient compliance after recall from screening mammography. AJR Am J Roentgenol 2007;188(4):894–96.
Sherman KA, Winch CJ, Borecky N, Boyages J. Psychological distress and streamlined BreastScreen follow-up assessment versus standard assessment. Med J Aust 2013;199(9):599–603.
Author information
Authors and Affiliations
Corresponding author
Additional information
Acknowledgements: This study was supported by a grant from the Dutch Organization for Health Research and Development (ZonMw). ZonMw had no influence on the study design, collection of data, data analysis, interpretation, writing of the manuscript or the decision to submit the manuscript for publication. We thank all participating women for taking the time to complete our questionnaires during a most distressing period. We also acknowledge all screening radiologists, research assistants, assessment centres and hospitals for their valuable contribution to this study.
Conflict of Interest: None to declare.
Rights and permissions
About this article

Cite this article
Timmers, J.M., Damen, J.A., Pijnappel, R.M. et al. Cost-effectiveness of non-invasive assessment in the Dutch breast cancer screening program versus usual care: A randomized controlled trial. Can J Public Health 105, e342–e347 (2014). https://doi.org/10.17269/cjph.105.4463
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.17269/cjph.105.4463