Introduction
Surgical removal of impacted mandibular third molars is one of the most commonly performed oral surgical procedure worldwide. The expected morbidities of this operation are pain, edema, trismus, and dry socket, which cause postoperative discomfort and impair the patient's quality of life [1]. Pain resulting from this type of surgery is used as one of the main parameters for assessing the pharmacological effectiveness of various methods of analgesia. Pain usually begins after the anesthesia wears off and reaches peak levels 6 to 12 hours postoperatively. It is usually moderate and of short duration for the first 24-48 hours [2]. Postoperative pain is caused by injury-induced release of cyclooxygenase-2, which triggers prostaglandins activity, that sensitize nociceptors [3].
After surgical extraction, inflammatory mediators are released and an increased vasodilation and permeability leads to postoperative edema. Postoperative edema reaches its peak intensity after 48 hours and markedly regress on the fourth day, with resolution 7 days after extraction [4], Like edema, trismus usually reaches its peak on the second day and resolves by the end of the first week [5].
It has been reported that the incidence of dry socket after lower third molar surgery is greater than 30%. Dry socket causes severe throbbing pain, one to three days after extraction, exposed bone cavity, and smelly odor [6]. A dry socket is caused by the disintegration of the blood clot which can be caused both by the activation of the fibrinolytic system in the socket and by mechanical stimulation. Hyperactivity of the fibrinolytic system is associated with local inflammation and bacterial invasion [7].
To control the postextraction morbidity, several therapies have been used, including medical and nonmedical therapy. Local or systemic corticosteroids and nonsteroidal anti-inflammatory drugs are commonly used, nevertheless they are associated with side effects such as gastric irritation, hypertension, and impairment of platelets function [8]. The nonmedical treatment include cryotherapy [9], photodynamic and low-level laser therapy [10], platelet rich fibrin [11], surgical drain [12], and kinesiologic tape [13].
Low level laser therapy (LLLT) demonstrates analgesic, anti-edematous, and healing promoting effects. LLLT has been shown to induce analgesia by stimulating the body's synthesis of endorphins (-endorphin), reducing the activity of bradykinin and C-fibers, and altering the pain threshold [14]. LLLT reduces mitochondrial metabolism and rapidly block pain transmission [15]. The anti-inflammatory effect occurs due to the increased phagocytic activity, the number and diameter of the lymph vessels, the reduced permeability of blood vessels and the restoration of microcapillary blood flow, the normalization of blood vessel permeability [16]. The LLLT also decrease the expressions of IL1-β, IL-6 and TNF-α mRNA [17]. These cytokines are important in neutrophil proliferation, recruitment and activation [18].
LLLT has been used in various oral conditions including lichen planus [19], burning mouth syndrome [20], recurrent herpes labialis [21], postherpetic neuralgia [22], temporomandibular joint disorders [23], accelerating orthodontic tooth movement [24], dry socket [25] and controlling postoperative pain after lower third molar extraction [26].
The therapeutic effect of the laser is influenced by the power output, the dose, the pulse frequency and the treatment frequency. The therapeutic wavelength range for low-level lasers is between 630 nm and 980 nm. Wavelengths between 600-700 nm are preferred for superficial tissue; Wavelengths between 780-950 nm can achieve deeper optical penetration and are preferred for treating deep tissues [27]. Pulse wave (PW) laser radiation offers additional advantages over continuous wave (CW) lasers. The high momentary power flows in PW ensure efficient energy transfer and the interval between the pulses enables heat to be dissipated in order to avoid thermal ablation [28].
The objective of this study was to investigate the effect of low-level laser therapy using 940 nm on postoperative inflammatory sequеlae following surgical removal of impacted lower third molars by clinically measuring the postoperative pain, swelling, and trismus.
Material and Methods
Study design and sample
This randomized, single-blinded, split-mouth prospective clinical and biochemical study was carried out on patients presented for surgical removal of bilateral impacted mandibular third molars. The study was conducted at a university affiliated hospital, Erbil- Iraq, between December 2016 and March 2018. The study has been approved by the board ethics committee and has been performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments. Written informed consent was taken from all the patients. The quality assessment was conducted according to the CONSORT Statement RCT checklist and Figure 1 shows the patient flow diagram. Inclusion criteria were age 18-35years, symmetrical bilateral impacted mandibular third molars classified as Class 2 and Class B according to the Pell-Gregory classification and mesioangular position, according to the Winter’s classification. Patients should have good health status, and clinical and or radiologic indications for third molar extraction were included in the study. There was no gender preference.
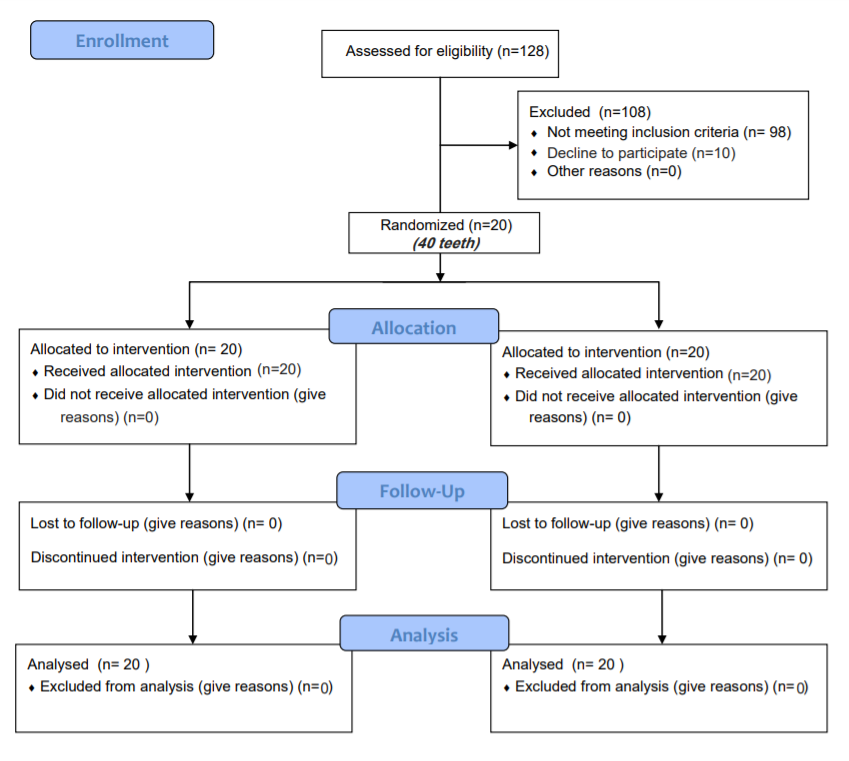
Figure 1. Patient flow chart.
Inclusion and exclusion criteria
The exclusion criteria were as follows: a systemic disease, acute pericoronitis and periodontal disease, pregnancy, breastfeeding, contraceptive use, smoking, consumption of analgesic or anti-inflammatory drugs prior to the study and apparent asymmetry between the left and right mandibular third molars. Patients who developed postoperative dry socket, who did not attend the follow up visits, and who required more than 30 minutes to remove the tooth were excluded.
The teeth were randomly assigned (www.random.org) into two groups: group I (20 teeth) received laser application, while group 2 (20 teeth) served as a control.
Low-level laser therapy
Immediately after completion of surgery, the experimented side received low-level laser therapy using BIOLASE laser (BIOLASE, INC, USA). The patient and the operator wore safety glasses during irradiation. The following parameters were used: wavelength (940 nm), power (0.5W), density (10 J/cm2). The fiber tip was placed close to the soft tissue, approximately 1 cm from the target area (noncontact mode), and the laser beam applied continuously for 30 s at the center of the extraction socket and at one cm distant from the wound on the buccal, lingual, and distal aspect, with a total time of 120 s and a total energy density of 40 J/3 cm2. In the control side, only the fiber tip was applied without exposure. The surgery between the two sides was performed one month apart. Following surgery, the patients were prescribed 625-mg amoxicillin-clavulanic acid tablet every 12 hours for 5 days along with oral ibuprofen 400 mg every 8 h for a 3-day period.
Measurement of pain, swelling, and trismus
The pain intensity was assessed daily, for one week, by the patient using a Visual Analogue Scale (VAS), which is an 11 cm scale from 0-10. (Zero as pain-free, and 10 as the worst pain).
The degree of swelling was evaluated by using the method of Feslihan and Eroğlu [29]. The baseline facial distance was calculated, using a flexible tape, immediately before surgery as the arithmetic mean of three facial linear measurements: the labial commissure – tragus, the gonion – lateral canthus, and the gonion – labial commissure. The degree of mouth opening was also evaluated, immediately before surgery, by measuring the maximal inter-incisal distance in millimeters using a digital caliper. Remeasurement of facial distances and degree of mouth opening was repeated on the 1st, 3rd, and 7th postoperative days.
Statistical analysis
Data analysis was performed using IBM SPSS Statistics for Windows, version 23 (IBM Corp., Armonk, NY). Difference in pain score was evaluated by Mann–Whitney U test. Unpaired t -test was used to measure the significant difference in the amount of facial swelling and the degree of mouth opening. A p-value of ≤ 0.05 was considered significant.
Results
Twenty patients, 13 males and 7 females, were enrolled in this clinical study. The average age of the participants was 26.3 years (standard deviation, 7.4 years). The mean operation time was 17.22±4.77 min in Group 1, 19.03±5.49 min in Group 2. The difference in the operation time was not significant (p=0.272). All patients completed the study period, with no losses. None of the patients showed any adverse reactions to the laser treatment.
The VAS pain score of the two groups is shown in Table 1. The laser group showed a lower VAS score than the control group. The difference was significant during the first three days (p<0.05); however, it was not significant during the last 4 days (P>0.05). The VAS of the laser group at the first three days was 4.46(±1.45), 4.00, (±1.36) and 3.35(2.33), respectively. For the control group, the VAS was 6.58 (±1.83), 5.82(±2.15), and 5.17(±1.97), respectively.
Table 1. Pain score of the two groups during the first postoperative week
|
Postoperative days |
VAS Scores Laser sides |
VAS Scores Control sides |
P-value |
||
|
Mean |
±SD |
Mean |
±SD |
||
|
1sth |
4.46 |
1.45 |
6.58 |
1.83 |
0.002* |
|
2nd |
4.00 |
1.36 |
5.82 |
2.15 |
0.023* |
|
3rd |
3.35 |
2.33 |
5.17 |
1.97 |
0.019* |
|
4th |
3.05 |
2.51 |
4.64 |
2.14 |
0.078 |
|
5th |
2.39 |
1.76 |
3.11 |
1.85 |
0.202 |
|
6th |
1.70 |
1.29 |
2.35 |
1.72 |
0.268 |
|
7th |
0.47 |
0.51 |
0.82 |
0.95 |
0.361 |
* Statistically significant.
The degree of facial swelling is shown in Table 2. The swelling was less in the laser group than the control group. The difference was significant at the first and third postoperative days (P<0.05) and not significant at the seventh postoperative day (P>0.05). At the first postoperative day, the facial measurements were 113.57 mm (±4.54mm) in the control group vs. 108.72 mm (±6.01mm) in the laser group. At the third postoperative day, the measurements were 118.43mm (±3.48mm) in the control group vs. 114.77mm (±5.63mm) in the laser group.
Table 2. Facial measurements of the two groups during the 1st, 3rd, and 7th postoperative days
|
Timing of measurement |
Facial Measurements (mm) |
t-value |
P-value |
|
|
Laser side Mean ±SD |
Control Side Mean ±SD |
|||
|
Preoperative |
104.34±4.36 |
102.58±6.29 |
1.028 |
0.310 |
|
1st postoperative day |
108.72±6.01 |
113.57±4.54 |
2.879 |
0.006* |
|
3rd postoperative day |
114.77±5.63 |
118.43±3.48 |
2.473 |
0.018* |
|
7th postoperative day |
105.39±5.32 |
104.15±2.63 |
0.934 |
0.356 |
* Statistically significant
The degree of mouth opening is shown in Table 3. The mouth opening of the laser group was less than the control group. The difference was significant at the first and third postoperative days (P<0.05) and not significant at the seventh postoperative days (P>0.05). At the first postoperative day, the mouth opening was 27.93mm (±3.12mm) in the control group vs. 33.48mm (±4.66mm) in the laser group. At the third postoperative day, the mouth opening was 25.58mm (±2.94mm) in the control group vs. 30.37mm (±2.71mm) in the laser group.
Table 3: Mouth opening of the two groups during the 1st, 3rd, and 7th postoperative days
|
Timing of measurement |
Mouth opening (mm) |
t-value |
P-value |
|
|
Laser side Mean ±SD |
Control Side Mean ±SD |
|||
|
Preoperative |
41.23 ±6.34 |
40.69 ±7.12 |
0.253 |
0.801 |
|
1st postoperative day |
33.48 ±4.66 |
27.93± 3.12 |
4.425 |
0.000* |
|
3rd postoperative day |
30.37 ±2.71 |
25.58 ±2.94 |
5.357 |
0.000* |
|
7th postoperative day |
39.14 ±4.22 |
37.78 ±6.34 |
0.798 |
0.429 |
* Significant
Discussion
The aim of this study was to evaluate the effect of low intensity laser photobiomodulation on postoperative inflammatory sequеlae after surgical removal of impacted lower third molars. The use of anti-inflammatory drug and analgesic to control inflammatory complications is complicated by the adverse effects associated with their use, such as gastrointestinal irritation, systemic bleeding or allergic reactions [30]. Therefore, attempting a noninvasive nonmedication and comfortable treatment modality for controlling postsurgical sequеlae is important. LLLT offers a safe therapeutic medical modality that is generally free from side effects. The FDA has classified the most commonly used LLLTs as class III: no-significant-risk medical devices.
A split-mouth design is used to prevents interpersonal variations of pain intensity. Likewise, a bilateral symmetrical impacted teeth with the same angulation (mesioangular), and depth of impaction (class II, position B), are selected to standardize the complexity of surgical procedures. Furthermore, split-mouth technique provided similar laser penetration depths for both sides. However, He et al. [31] have criticized the split-mouth design, suggesting that it may be difficult to avoid selection bias in baseline equivalence control. When surgical procedures are not performed concurrently, patients' pain thresholds may change based on their initial surgical experience. In addition, tolerance to trismus can increase, leading to unequal baseline measurements. To minimize possible bias in the present study, LLLT was used at either the first or second surgical procedure. As the intensity postoperative morbidities is closely correlated to the degree of trauma and duration of surgery, any operations lasting more 30 minutes were not considered. However, no significant difference in the operation time between the two groups was noted.
The anti-edematous and analgesic effect of photobiomodulation has been proved under both experimental and clinical conditions [31]. However, the effect of LLLT photobiomodulation on the morbidities of third molar surgery and have reported conflicting controversial results. These conflicting results may be due to difficulties in the measurement of variables related to postoperative sequelae, differences in study design or methods, differences in types of lasers and handpieces used, and differences in irradiation parameters.
In the present study, VAS pain score was highest on the first postoperative day and then gradually subsides throughout the subsequent days, in both groups. Pain VAS score was lower in the laser irradiated group than in the control group and the difference was significant in the first three days. This finding is attributed to the fact that photobiomodulation increases the pain threshold, blocks nerve conduction, and stimulates the synthesis of endogenous endorphins (b-endorphin) [32, 33]. In addition, low level laser it inhibits the cascade of arachidonic acid, reduces the concentration of cyclooxygenase 2, prostaglandin ES2, and histamine [34]. The results of this study come in accordance with the study of Hadad et al. [35]. In their study, the pain was significantly reduced at the 24 and 48 hours by an intraoral diode laser application at 810 nm wavelength, 6 J (100 mW, 60 seconds/point). Momeni et al. [36] found that pain scores did not differ significantly up to the fifth postoperative day; however, on the sixth and seventh days, it was significantly lower in the laser treated sides. Santos et al. [37] also conclude that irradiation of extracted lower third molar area on the buccal, lingual and center of the socket with 780 nm soft laser significantly reduced the pain on 24-, 48-, and 72-hours post-surgery. In contrast, Eroglu and Keskin Tunc [38] did not show effectiveness with the application of 940 nm extraoral diode laser for reducing pain. Ahrari et al. [39] also did not found any significant effect of 660 nm and 810 nm laser (200 mW, 30 seconds radiation to lingual, buccal and occlusal surfaces of the socket, 6 J/area) for reducing pain.
Facial Swelling in the laser group was significantly lower at all time intervals than in the placebo group. This effect could be attributed to laser-induced macrophage activation, which increase protein absorption. Laser also to increase the number and diameter of lymph vessels and decreases the blood vessels’ permeability, modifies the hydrostatic and intracapillary pressure, and induces the absorption of interstitial fluid with a consequent reduction of edema [40].
The findings of this study are in consensus with many studies that have reported a significant effect of low-density laser in reducing postoperative swelling after third molar surgery. Singh et al. [41], Bianchi de Moraes et al. [42], and Mohajerani et al. [43] showed the effectiveness of LLLT in reducing swelling after surgical removal of impacted lower mandibular third molars. In a systematic review and meta-analysis, Domah et al. [44] and Duarte de Oliveira at al. [45] found that LLLT has a positive outcome in the reduction of postoperative swelling after mandibular third molar surgery. In contrast to the findings of our study, López-Ramírez et al. [46] and Pedreira et al. [47] have failed to show a beneficial effect of laser on swelling.
Mouth opening in the laser group was significantly greater than the control group during the three-time intervals of this study. Improvement of mouth opening may be attributed to analgesic and anti-inflammatory effects of low-level laser, as well as the minimum thermal effects occurring during laser radiation that consequently, diminishes trismus. Since the internal pterygoid, masseter, and tendon of the temporalis muscle are exposed to the radiation field, relaxation of the muscle may occur due to the thermal effect. Our findings come in accordance with the conclusions of Landucci et al. [48], who found a significantly better mouth opening after irradiation wit laser energy of 7.5 J/cm2, with a power output of 10 mW and at an infrared wavelength of 780 nm. In the study of Aras and Güngörmüş [49], a Ga-Al-As diode laser with a continuous wavelength of 808 nm was effective in reducing trismus after third molar surgery, when applied intra- and extraorally. In contrast to our results, Singh et al. [41] found no significant effects of laser on trismus. In addition, in their systematic review and meta-analysis, Domah et al. [44] Duarte de Oliveira et al. [45], didn’t found any significant effects of laser on the maximum mouth opening after third molar surgery.
This variation in the results among different studies is the lack of standardization in studies with regard to the samples, methods and the use of lasers with a different wavelength, power, and energy. The anti-inflammatory effect may be affected by the wavelength and nature of the tissue. Hudson et al. [50] demonstrated that in bovine tissue samples, a laser beam at 880 nm penetrated 54% deeper than a laser beam at 940 nm. Brosseau, et al. [51] also found that laser at 632 nm was more effective on pain as compared to 820 nm laser. The site of application (intraoral vs. extraoral), the number of irradiation (single vs. multiple), the timing (preoperative vs. postoperative), the duration and mode of irradiation (continuous vs. pulsed), and distance of the source from the tissue, could also influence the response to laser therapy. Sierra et al. [52] found a statistically significant interaction between the irradiation site and wavelength, with swelling and trismus were smaller if the red laser was applied intra-orally or if infrared laser was applied extra-orally. Although intraoral use would allow closer application to the surgical site, the size of some laser probes precludes their intraoral use.
Conclusion
Single intraoral irradiation of the wound, with Low level laser, significantly reduces pain and facial swelling and increases the degree of mouth opening, following surgical removal of impacted lower third molar. No any side effects were noted with this treatment. It should be considered as an adjunctive modality to alleviate symptoms in oral surgical procedures.
Ethical approval
All procedures performed in this study were in accordance with the ethical standards of our institutional research committee and with the 1964 Declaration of Helsinki and its later amendments.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The author declares no conflict of interest in preparing this article.
- Eshghpour M, Ahrari F, Takallu M. Is low-level laser therapy effective in the management of pain and swelling after mandibular third molar surgery? J Oral Maxillofac Surg 2016; 74(7): 1322.e1-8. https://doi.org/10.1016/j.joms.2016.02.030.
- Osunde OD, Adebola RA, Omeje UK. Management of inflammatory complications in third molar surgery: a review of the literature. Afr Health Sci 2011; 11(3): 530-537. https://pubmed.ncbi.nlm.nih.gov/22275950.
- Samad TA, Moore KA, Sapirstein A, Billet S, Allchorne A, Poole S, et al. Interleukin-1B-mediated induction of COX-2 in the CNS contributes to inflammatory pain hypersensitivity. Nature 2001; 410(6827): 471-475. https://doi.org/10.1038/35068566.
- Darawade DA, Kumar S, Mehta R, Sharma AR, Reddy GS. In search of a better option: dexamethasone versus methylprednisolone in third molar impaction surgery. J Int Oral Health 2014; 6(6): 14–17. https://pubmed.ncbi.nlm.nih.gov/25628476.
- Shulman DH, Shipman B, Willis FB. Treating trismus with dynamic splinting: A case report. J Oral Sci 2009; 51(1): 141-144. https://doi.org/10.2334/josnusd.51.141.
- Bowe DC, Rogers S, Stassen LF. The management of dry socket/alveolar osteitis. J Ir Dent Assoc 2011; 57(6): 305-310. https://pubmed.ncbi.nlm.nih.gov/22338284.
- Catellani JE. Review of factors contributing to dry socket through enhanced fibrinolysis. J Oral Surg. 1979;37(1): 42–46. https://pubmed.ncbi.nlm.nih.gov/22338284.
- Kapugi M, Cunningham K. Corticosteroids. Orthop Nurs 2019; 38(5): 336-339. https://doi.org/10.1097/nor.0000000000000595.
- do Nascimento-Júnior EM, Dos Santos GMS, Tavares Mendes ML, Cenci M, Correa MB, Pereira-Cenci T, et al. Cryotherapy in reducing pain, trismus, and facial swelling after third-molar surgery: Systematic review and meta-analysis of randomized clinical trials. J Am Dent Assoc 2019; 150(4): 269-277.e1. https://doi.org/10.1016/j.adaj.2018.11.008.
- Fraga RS, Antunes LAA, Fialho WLS, Valente MI, Gomes CC, Fontes KBFC, et al. Do Antimicrobial Photodynamic Therapy and Low-Level Laser Therapy Minimize Postoperative Pain and Edema After Molar Extraction? J Oral Maxillofac Surg 2020; 78(12): 2155.e1-2155.e10. https://doi.org/10.1016/j.joms.2020.08.002.
- Torul D, Omezli MM, Kahveci K. Evaluation of the effects of concentrated growth factors or advanced platelet rich-fibrin on postoperative pain, edema, and trismus following lower third molar removal: A randomized controlled clinical trial. J Stomatol Oral Maxillofac Surg 2020; 121(6): 646-651. https://doi.org/10.1016/j.jormas.2020.02.004.
- Katz MS, Peters F, Elvers D, Winterhalder P, Kniha K, Möhlhenrich SC, et al. Effect of drain application on postoperative complaints after surgical removal of impacted wisdom teeth-a randomized observer-blinded split-mouth clinical trial. Clin Oral Investig 2021; 25(1): 345-353. https://doi.org/10.1007/s00784-020-03464-5.
- Yurttutan ME, Sancak KT. The effect of kinesio taping with the web strip technique on pain, edema, and trismus after impacted mandibular third molar surgery. Niger J Clin Pract 2020; 23(9): 1260-1265. https://doi.org/10.4103/njcp.njcp_23_20.
- Fávaro-Pípi E, Ribeiro DA, Ribeiro JU, Bossini P, Oliveira P, Parizotto NA, et al. Low-level laser therapy induces differential expression of osteogenic genes during bone repair in rats. Photomed Laser Surg 2011; 29(5): 311-317. https://doi.org/10.1089/pho.2010.2841.
- Holanda VM, Chavantes MC, Wu X, Anders JJ. The mechanistic basis for photobiomodulation therapy of neuropathic pain by near infrared laser light. Lasers Surg Med 2017; 49(5): 516-524. https://doi.org/10.1002/lsm.22628.
- Fabre HS, Navarro RL, Oltramari-Navarro PV, Oliveira RF, Pires-Oliveira DA, Andraus RA, et al. Anti-infammatory and analgesic effects of low-level laser therapy on the postoperative healing process. J Phys Ther Sci 2015; 27(6): 1645-1648. https://doi.org/10.1589/jpts.27.1645.
- Fazza TF, Pinheiro BV, da Fonseca LMC, Sergio LPDS, Botelho MP, Lopes GM, et al. Effect of low-level laser therapy on the inflammatory response in an experimental model of ventilator-induced lung injury. Photochem Photobiol Sci. 2020; 19(10): 1356-1363. https://doi.org/10.1039/d0pp00053a.
- Fukuda TY, Tanji MM, Silva SR, Sato MN, Plapler H. Infrared low-level diode laser on inflammatory process modulation in mice: pro- and anti-inflammatory cytokines. Lasers Med Sci 2013; 28(5): 1305-1313. https://doi.org/10.1007/s10103-012-1231-z.
- Al-Maweri SA, Kalakonda B, Al-Soneidar WA, Al-Shamiri HM, Alakhali MS, Alaizari N. Efficacy of low-level laser therapy in management of symptomatic oral lichen planus: a systematic review. Lasers Med Sci 2017; 32(6): 1429-1437. https://doi.org/10.1007/s10103-017-2233-7.
- Valenzuela S, Lopez-Jornet P. Effects of low-level laser therapy on burning mouth syndrome. J Oral Rehabil 2017; 44(2): 125-132. https://doi.org/10.1111/joor.12463.
- Al-Maweri SA, Kalakonda B, AlAizari NA, Al-Soneidar WA, Ashraf S, Abdulrab S, et al. Efficacy of low-level laser therapy in management of recurrent herpes labialis: a systematic review. Lasers Med Sci 2018; 33(7): 1423-1430. https://doi.org/10.1007/s10103-018-2542-5.
- Mukhtar R, Fazal MU, Saleem M, Saleem S. Role of low-level laser therapy in post-herpetic neuralgia: a pilot study. Lasers Med Sci 2020; 35(8): 1759-1764. https://doi.org/10.1007/s10103-020-02969-5.
- Chellappa D, Thirupathy M. Comparative efficacy of low-Level laser and TENS in the symptomatic relief of temporomandibular joint disorders: A randomized clinical trial. Indian J Dent Res 2020; 31(1): 42-47. https://doi.org/10.4103/ijdr.ijdr_735_18.
- Zheng J, Yang K. Clinical research: low-level laser therapy in accelerating orthodontic tooth movement. BMC Oral Health 2021; 21(1): 324. https://doi.org/10.1186/s12903-021-01684-z.
- Kamal A, Salman B, Ar NH, Samsudin AR. Management of dry socket with low-level laser therapy. Clin Oral Investig 2021; 25(3): 1029-1033. https://doi.org/10.1007/s00784-020-03393-3.
- de Barros DD, Dos Santos Barros Catão JS, Ferreira ACD, Simões TMS, de Vasconcelos Catão MHC. Low-level laser therapy is effective in controlling postoperative pain in lower third molar extractions: a systematic review and meta-analysis. Lasers Med Sci 2022. https://doi.org/10.1007/s10103-021-03470-3.
- Merigo E, Vescovi P, Margalit M, Ricotti E, Stea S, Meleti M, et al. Efficacy of LLLT in swelling and pain control after the extraction of lower impacted third molars. Laser Ther 2015; 24(1): 39-46. https://doi.org/10.5978/islsm.15-or-05.
- Ando T, Xuan W, Xu T, Dai T, Sharma SK, Kharkwal GB, et al. Comparison of Therapeutic Effects between Pulsed and Continuous Wave 810-nm Wavelength Laser Irradiation for Traumatic Brain Injury in Mice. PLoS One 2011; 6(10): e26212. https://doi.org/10.1371/journal.pone.0026212.
- Feslihan E, Eroğlu CN. Can Photobiomodulation Therapy Be an Alternative to Methylprednisolone in Reducing Pain, Swelling, and Trismus After Removal of Impacted Third Molars? Photobiomodul Photomed Laser Surg 2019; 37(11): 700-705. https://doi.org/10.1089/photob.2019.4696.
- Bamgbose BO, Akinwande JA, Adeyemo WL, Ladeinde AL, Arotiba GT, Ogunlewe MO. Effects of co-administered dexamethasone and diclofenac potassium on pain, swelling and trismus following third molar surgery. Head Face Med 2005; 1: 11. https://doi.org/10.1186/1746-160x-1-11.
- He WL, Yu FY, Li CJ, Pan J, Zhuang R, Duan PJ. A systematic review and meta-analysis on the efficacy of low-level laser therapy in the management of complication after mandibular third molar surgery. Lasers Med Sci 2015; 30(6): 1779-1788. https://doi.org/10.1007/s10103-014-1634-0.
- Hagiwara S, Iwasaka H, Okuda K, Noguchi T. GaAlAs (830 nm) low-level laser enhances peripheral endogenous opioid analgesia in rats. Lasers Surg Med 2007; 39(10): 797-802. https://doi.org/10.1002/lsm.20583.
- Chow RT, David MA, Armati PJ. 830 nm laser irradiation induces varicosity formation, reduces mitochondrial membrane potential and blocks fast axonal flow in small and medium diameter rat dorsal root ganglion neurons: implications for the analgesic effects of 830 nm laser. J Peripher Nerv Syst 2007; 12(1): 28-39. https://doi.org/10.1111/j.1529-8027.2007.00114.x.
- Pigatto GR, Silva CS, Parizotto NA. Photobiomodulation therapy reduces acute pain and inflammation in mice. J Photochem Photobiol B 2019; 196: 111513. https://doi.org/10.1016/j.jphotobiol.2019.111513.
- Hadad H, Santos AFP, de Jesus LK, Poli PP, Mariano RC, Theodoro LH, et al. Photobiomodulation Therapy Improves Postoperative Pain and Edema in Third Molar Surgeries: A Randomized, Comparative, Double-Blind, and Prospective Clinical Trial. J Oral Maxillofac Surg 2022; 80(1): 37.e1-37.e12. https://doi.org/10.1016/j.joms.2021.08.267.
- Momeni E, Barati H, Arbabi MR, Jalali B, Moosavi MS. Low-level laser therapy using laser diode 940 nm in the mandibular impacted third molar surgery: double-blind randomized clinical trial. BMC Oral Health 2021; 21(1): 77. https://doi.org/10.1186/s12903-021-01434-1.
- Santos PL, Marotto AP, Zatta da Silva T, Bottura MP, Valencise M, Marques DO, et al. Is Low-Level Laser Therapy Effective for Pain Control After the Surgical Removal of Unerupted Third Molars? A Randomized Trial. J Oral Maxillofac Surg 2020; 78(2): 184-189. https://doi.org/10.1016/j.joms.2019.08.029.
- Eroglu CN, Keskin Tunc S. Effectiveness of Single Session of Low-Level Laser Therapy with a 940 nm Wavelength Diode Laser on Pain, Swelling, and Trismus After Impacted Third Molar Surgery. Photomed Laser Surg 2016; 34(9): 406-410. https://doi.org/10.1089/pho.2016.4101.
- Ahrari F, Eshghpour M, Zare R, Ebrahimi S, Fallahrastegar A, Khaki H. Effectiveness of Low-Level Laser Irradiation in Reducing Pain and Accelerating Socket Healing After Undisturbed Tooth Extraction. J Lasers Med Sci 2020; 11(3): 274-279. https://doi.org/10.34172/jlms.2020.46.
- AlGhamdi KM, Kumar A, Moussa NA. Low-level laser therapy: a useful technique for enhancing the proliferation of various cultured cells. Lasers Med Sci 2012; 27(1): 237-249. https://doi.org/10.1007/s10103-011-0885-2.
- Singh V, Garg A, Bhagol A, Savarna S, Agarwal SK. Photobiomodulation Alleviates Postoperative Discomfort After Mandibular Third Molar Surgery. J Oral Maxillofac Surg 2019; 77(12): 2412-2421. https://doi.org/10.1016/j.joms.2019.06.009.
- Bianchi de Moraes M, Gomes de Oliveira R, Raldi FV, Nascimento RD, Santamaria MP, Loureiro Sato FR. Does the Low-Intensity Laser Protocol Affect Tissue Healing After Third Molar Removal? J Oral Maxillofac Surg 2020; 78(11): 1920.e1-1920.e9. https://doi.org/10.1016/j.joms.2020.05.018.
- Mohajerani H, Tabeie F, Alirezaei A, Keyvani G, Bemanali M. Does Combined Low-Level Laser and Light-Emitting Diode Light Irradiation Reduce Pain, Swelling, and Trismus After Surgical Extraction of Mandibular Third Molars? A Randomized Double-Blinded Crossover Study. J Oral Maxillofac Surg 2021; 79(8): 1621-1628. https://doi.org/10.1016/j.joms.2020.07.017.
- Domah F, Shah R, Nurmatov UB, Tagiyeva N. The Use of Low-Level Laser Therapy to Reduce Postoperative Morbidity After Third Molar Surgery: A Systematic Review and Meta-Analysis. J Oral Maxillofac Surg 2021; 79(2): 313.e1-313.e19. https://doi.org/10.1016/j.joms.2020.09.018.
- Duarte de Oliveira FJ, Brasil GMLC, Araújo Soares GP, Fernandes Paiva DF, de Assis de Souza Júnior F. Use of low-level laser therapy to reduce postoperative pain, edema, and trismus following third molar surgery: A systematic review and meta-analysis. J Craniomaxillofac Surg 2021; 49(11): 1088-1096. https://doi.org/10.1016/j.jcms.2021.06.006.
- López-Ramírez M, Vílchez-Pérez MA, Gargallo-Albiol J, Arnabat-Domínguez J, Gay-Escoda C. Efficacy of low-level laser therapy in the management of pain, facial swelling, and postoperative trismus after a lower third molar extraction. A preliminary study. Lasers Med Sci 2012; 27(3): 559-566. https://doi.org/10.1007/s10103-011-0936-8.
- Pedreira AA, Wanderley FG, Sa MF, Viena CS, Perez A, Hoshi R, et al. Thermographic and clinical evaluation of 808-nm laser photobiomodulation effects after third molar extraction. Minerva Stomatol 2016; 65(4): 213-222. https://pubmed.ncbi.nlm.nih.gov/27374361.
- Landucci A, Wosny AC, Uetanabaro LC, Moro A, Araujo MR. Efficacy of a single dose of low-level laser therapy in reducing pain, swelling, and trismus following third molar extraction surgery. Int J Oral Maxillofac Surg 2016; 45(3): 392-398. https://doi.org/10.1016/j.ijom.2015.10.023.
- Aras MH, Güngörmüş M. Placebo-controlled randomized clinical trial of the effect two different low-level laser therapies (LLLT) –intraoral and extraoral – on trismus and facial swelling following surgical extraction of the lower third molar. Lasers Med Sci 2010; 25(5): 641-645. https://doi.org/10.1007/s10103-009-0684-1.
- Hudson DE, Hudson DO, Wininger JM, Richardson BD. Penetration of laser light at 808and 980nm in bovine tissue samples. Photomed Laser Surg 2013; 31(4): 163-168. https://doi.org/10.1089/pho.2012.3284.
- Brosseau L, Welch V, Wells G, DeBie R, Gam A, Harman K, et al. Low- level laser therapy (classes I, II and III) in the treatment of rheumatoid arthritis. Cochrane Database Syst Rev 2000; (2): CD002049. https://doi.org/10.1002/14651858.cd002049.
- Sierra SO, Deana AM, Bussadori SK, da Mota AC, Ferrari RA, do Vale KL, et al. Choosing between intraoral or extraoral, red or infrared laser irradiation after impacted third molar extraction. Lasers Surg Med 2016; 48(5): 511-518. https://doi.org/10.1002/lsm.22488.
Received 1 February 2022, Revised 25 February 2022, Accepted 23 March 2022
© 2022, Russian Open Medical Journal
Correspondence to Shehab Ahmed Hamad. Address: Kurdistan Board for Medical Specialties, Ziraah Square, Po. Box: 0845/32, Erbil, Kurdistan Region, Iraq. E-mail: shehab.ahmed@hmu.edu.krd.
