


A 37-year-old woman with an obstetric history of classical cesarean delivery presented for antenatal care. Ultrasound at 17 weeks showed an invasive placenta at the incision site of the prior classical cesarean. Serial ultrasounds every two weeks confirmed a stable appearance up until 31 weeks. Magnetic resonance imaging (MRI) then showed progression to percreta with possible invasion into the abdominal wall (Figure 1). We performed a scheduled cesarean hysterectomy at 33 weeks to reduce the potential for further organ invasion. At the time of hysterectomy, the placenta protruded through the previous classical cesarean incision site (Appendix 1, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.171411/-/DC1). We delivered the neonate below the level of invasion, through a lower segment incision, before hysterectomy.
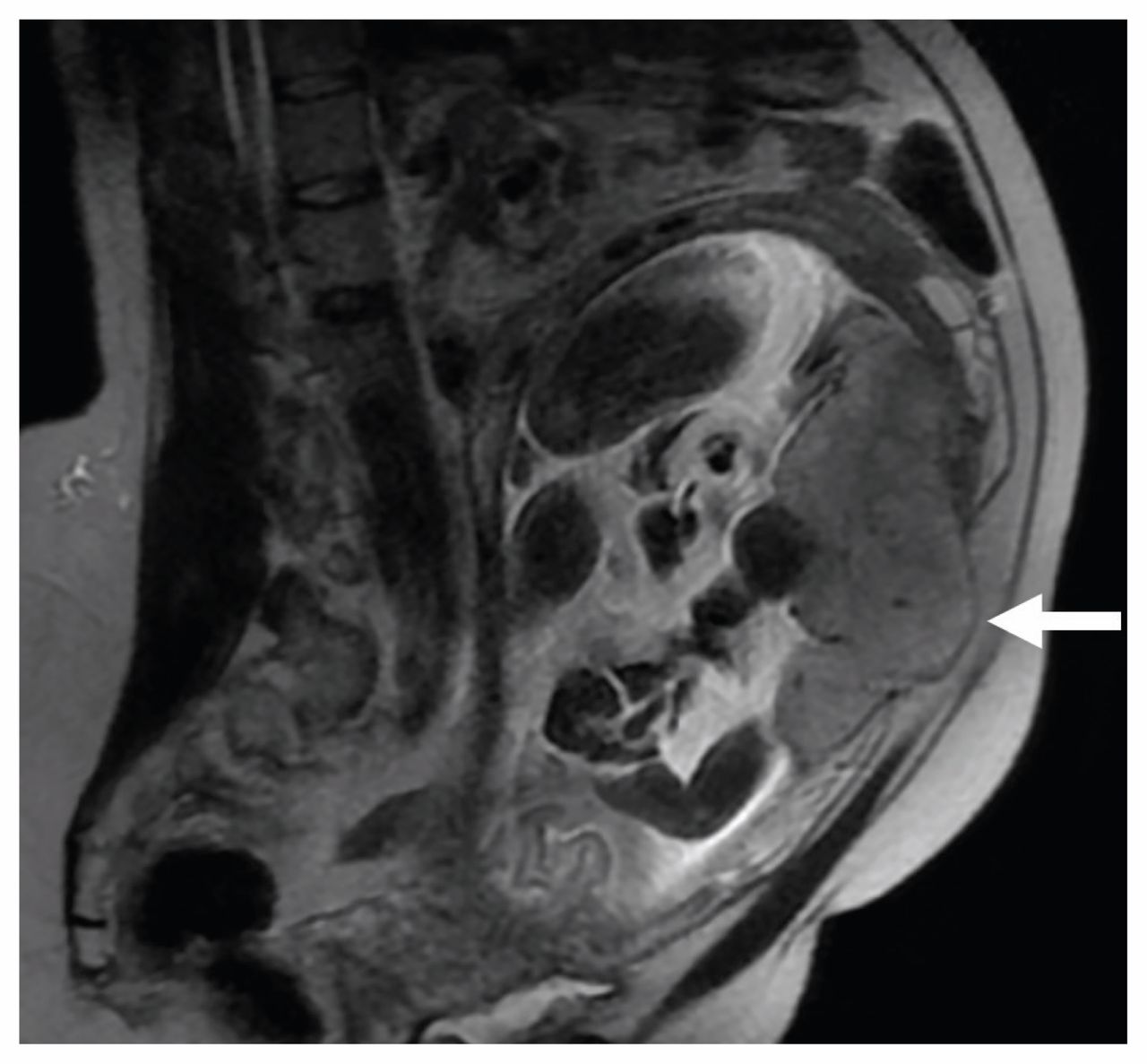
Noncontrast magnetic resonance imaging in a 37-year-old woman at 31 weeks, showing an area of placental invasion through the upper anterior uterus (arrow) and possibly into the anterior abdominal wall. The fetus is not shown entirely in this plane.
Placenta accreta syndromes occur when chorionic villi abnormally invade the uterine myometrium. Placenta percreta involves invasion to the uterine serosa or surrounding structures.1 Antenatal diagnosis optimizes delivery planning, reducing maternal morbidity and mortality secondary to hemorrhage. Incidence ranges from 0.04% to 0.9% of all deliveries.2 One of the most important risk factors is previous uterine surgery, including cesarean delivery;3 however, there does not seem to be a substantially increased risk of accreta syndromes in classical versus lower segment cesareans.4 Ultrasonography and MRI can detect accreta syndromes with sensitivity of 77% to 88% and specificity of 67% to 100%.5
Because of this patient’s previous classical cesarean, the level of placental invasion was higher than in most cases, where the placenta typically invades the lower uterine segment and risks bladder involvement. Unique management challenges in our case included performing the cesarean hysterectomy though a midline abdominal skin incision and careful inspection of the upper abdomen and abdominal wall for extra-uterine disease. Management of accreta syndromes includes a scheduled cesarean delivery and then hysterectomy, requiring the involvement of a multidisciplinary surgical team.1 Timing of delivery is individualized, but many authors suggest 34–36 weeks.1
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
The authors have obtained patient consent.
In this issue

{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

