
Inferior pole of patella fracture with tibial tuberosity avulsion and longitudinal patella tendon split is almost never reported and should be kept in mind when an adolescent comes with pre-trauma anterior knee pain.
Dr. Nrupam Mehta, Department of Orthopaedics, Dr. DY Patil Medical College and Hospital, Mumbai, Maharashtra, India. E-mail: nrupam.m@hotmail.com
Introduction: Distal pole of patella avulsion fracture with tibial tuberosity avulsion has been frequently reported as a bifocal patellar tendon injury. However, an osteochondral lateral patella facet fracture with a longitudinal split in the patella tendon in addition to these avulsion fractures has never been documented previously. Hence, we now report this trifocal patellar tendon injury.
Case Report: An adolescent with a trifocal patella tendon injury underwent a fixation with a combination of transosseous pull- through sutures, suture tape, and knotless anchor. The patient was rehabilitated with gradual increase in 30° of knee flexion weekly and has now attained full knee range of motion.
Conclusion: Fixation of the small avulsion fracture can be challenging using conventional methods such as cannulated cancellous screws especially in an immature skeleton as it can crush the fragments. Suture tape, transosseous tunnels, and knotless suture anchors have more flexibility, they avoid the physis and provide adequate strength in such situations compared to metallic implants.
Keywords: Inferior pole of patella avulsion, tibial tuberosity fracture, knotless suture anchor, suture tape.
The infrequent occurrence of acute avulsion of the tibial tubercle, particularly in the context of a rare bifocal disruption of the knee extensor mechanism. This injury, involving the detachment of the tibial tubercle and the patellar tendon from their respective bony attachments, is not commonly observed in adults. The reported incidence rates underscore the unusual nature of this injury, with a higher propensity for it to happen in individuals who are skeletally immature, such as children and adolescents. The tendency for avulsion fractures at tendon attachment sites rather than actual tearing of the tendon itself in this age group is a noteworthy observation [1]. The necessity for precise external force acting simultaneously on both ends of the patellar tendon further contributes to its rarity. The suggested mechanisms of injury, including a direct impact on the distal patella with forceful flexion of the lower leg, a central blow to the patellar tendon with divergent forces against the bony insertions, or a quadriceps overload leading to eccentric muscle contraction during knee flexion, provide valuable insights into potential causes [2]. Repeated trauma immediately one after the other can also be considered now. Understanding these mechanisms is crucial for accurate diagnosis and the implementation of preventive measures. It emphasizes the importance of meticulous clinical assessment, appropriate imaging studies, and a comprehensive understanding of the injury mechanisms to inform effective treatment strategies. Furthermore, the limited existing literature on this topic highlights the need for additional research.
A 14-year-old male came to the outpatient department with swelling over the right knee, with an inability to bear weight following a fall while running on the ground. He also gives a history of anterior knee pain before the trauma ongoing since 4 . On physical examination, he was noted to have an effusion over the affected knee with tenderness over the patella and tibial tuberosity (Fig. 1). 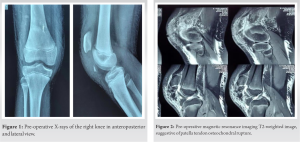 Radiographs obtained demonstrated patella alta and a tibial tuberosity avulsion fracture. He was placed in a long knee brace for immediate management. Further investigations were done, where the magnetic resonance imaging reported an associated inferior pole non-bony tendinous avulsion fracture (Figs. 2 and 3). The patient was scheduled for surgery the next day.
Radiographs obtained demonstrated patella alta and a tibial tuberosity avulsion fracture. He was placed in a long knee brace for immediate management. Further investigations were done, where the magnetic resonance imaging reported an associated inferior pole non-bony tendinous avulsion fracture (Figs. 2 and 3). The patient was scheduled for surgery the next day.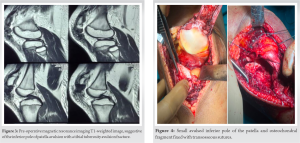
Intraoperative exploration revealed an osteochondral fracture of lateral patellar facet size 10mm, complete avulsion of the patella tendon from the tibial tubercle with longitudinal split in the patellar tendon along with inferior pole of patella avulsion fracture. Repair of the proximal avulsion was performed using transosseous sutures on the anterior patellar cortex (Fig. 4). The longitudinal patellar tendon rupture was sutured by the Krakow method (Fig. 5). Once the two injuries were fixed, the tibial tuberosity avulsion was then secured with a combination of transosseous suture tape and a knotless anchor by double row fixation with the knee in complete extension position (Fig. 6). Medial and lateral retinaculum tears were sutured back. There was no laxity of the tendon intraoperatively. Closure was done. A diagrammatic representation has been shown below (Fig. 7).
Medial and lateral retinaculum tears were sutured back. There was no laxity of the tendon intraoperatively. Closure was done. A diagrammatic representation has been shown below (Fig. 7).
Postoperatively, X-rays were done (Fig. 8) and the patient was placed in a long knee brace and rehabilitated with a gradual increase in knee range of motion by 30° of flexion every week with nil weight-bearing walk for the initial 4 weeks following surgery. The Insall–Salvati Index of both knees was compared and found to be almost the same, suggesting there is no more patella alta postoperatively (Fig. 9).  Follow-up at 6 weeks after surgery displayed radiological improvement. Full range of motion had been achieved at 12 weeks follow-up (Fig. 10).
Follow-up at 6 weeks after surgery displayed radiological improvement. Full range of motion had been achieved at 12 weeks follow-up (Fig. 10).
Looking at the xray the inferior pole of patella with fracture area is rounded as if it is chronic old ffracture rather than acute?explain please? The fracture fragment seen on lateral xray shows a tibial tuberosity avulsion fracture of patella tendon and and a non bony avulsion fracture from the lower pole of patella in 50% of the lateral tendon. Hence there is no bony fragment or acute fracture visible on the inferior pole of patella.
Trifocal injuries involving the avulsion of the patellar tendon and occurring in the absence of definitive radiographic signs are quite rare [2]. Typically, in young patients, injuries affecting the inferior pole of the patella and tuberosity are of the avulsion type. This is because the growth plates in these areas are relatively weaker compared to the robust patellar tendon at that stage of development. These injuries are often associated with high-velocity trauma or repeated trauma [3]. Trifocal injuries which entail a combination of distal patella avulsion, tibial tuberosity avulsion, and osteochondral lateral patella facet fracture with longitudinal tendon rupture are exceptionally uncommon and have scant documentation. [Two common conditions suspected to be linked with avulsion style fractures are Osgood–Schlatter syndrome at the tibial tuberosity and Sinding-Larsen-Johansson (SLJ) syndrome at the inferior pole of the patella. Osgood–Schlatter disease is more prevalent and often occurs in males, frequently coinciding with the rapid growth observed in adolescents [4, 5]. SLJ is more commonly noted in younger individuals, typically between the ages of 10 and 12, and patients frequently report of experiencing pre-trauma anterior knee pain [6, 7]. Previous literature has suggested that the inferior pole of patella fractures can be treated with a cannulated cancellous screw [8, 9]. However, in instances where the avulsed fragment is too small, fixation can be accomplished using suture tape sutures. A similar challenge can be encountered during the fixation of the tibial tuberosity, but due to the high risk of avulsion in that region, a knotless double-row anchor can be utilized [10]. This approach can provide the requisite stability and sufficient compression needed for the injury.
Complex injuries of the patella involving three focal points, referred to as trifocal injuries, are rarely encountered in young children, especially when the injury results from a high-velocity mechanism. In such cases, it is imperative to conduct thorough intraoperative exploration. Surgeons should have various fixation devices readily available, including suture tape and knotless suture anchors. Due to the presence of a small avulsed fragment, traditional methods of fixation may not be suitable for addressing these injuries.
Apart from the conventional cancellous screws, avulsed fragments which are very small can be attempted to be fixed with suture tape or anchors, which are more viable.
References
- 1.Hermansen LL, Freund KG. Bifocal osseous avulsion of the patellar tendon from the distal patella and tibial tuberosity in a child. Knee Surg Sports Traumatol Arthrosc 2016;24:712-4. [Google Scholar]
- 2.Atzmon R, Iohanes E, Dubin J, Rosenthal A, Drexler M, Sherman SL. Bifocal avulsion fracture and fixation of the patellar tendon: A case report. J ISAKOS 2023;8:497-501. [Google Scholar]
- 3.Kang S, Chung PH, Kim YS, Lee HM, Kim JP. Bifocal disruption of the knee extensor mechanism: A case report and literature review. Arch Orthop Trauma Surg 2013;133:517-21. [Google Scholar]
- 4.Woolnough T, Lovsted G, MacDonald A, Johal H, Al-Asiri JA. Combined tibial tubercle fracture with patellar tendon avulsion in an adult: A rare case and novel fixation technique. Cureus 2020;12:e7929. [Google Scholar]
- 5.Frey S, Hosalkar H, Cameron DB, Heath A, David Horn B, Ganley TJ. Tibial tuberosity fractures in adolescents. J Child Orthop 2008;2:469-74. [Google Scholar]
- 6.Kunis GW, Berko JA, Shogan JC, Sharan JB, Jones D. Tibial tubercle avulsion fractures in adolescents: A narrative review and case report. J Orthop Orthop Surg 2021;2:12-8. [Google Scholar]
- 7.Gottsegen CJ, Eyer BA, White EA, Learch TJ, Forrester D. Avulsion fractures of the knee: Imaging findings and clinical significance. Radiographics 2008;28:1755-70. [Google Scholar]
- 8.Yoon JR, Kim TS, Kim HJ, Noh HK, Oh JK, Yoo JC. Simultaneous patellar tendon avulsion fracture from both patella and tibial tuberosity: A case report. Knee Surg Sports Traumatol Arthrosc 2007;15:225-7. [Google Scholar]
- 9.Calderaro C, Falciglia F, Giordano M, Aulisa AG, Toniolo RM. Bifocal avulsion of the patellar tendon from the distal patella and tibial tuberosity in a skeletally immature patient: A case report. JBJS Case Connect 2020;10:e20.00065. [Google Scholar]
- 10.Swan K Jr., Rizio L. Combined avulsion fracture of the tibial tubercle and avulsion of the patellar ligament. Orthopedics 2007;30:571-2. [Google Scholar]








