
Manuscript accepted on :21-Jun-2022
Published online on: --
Plagiarism Check: Yes
Reviewed by: Masoud Mohammadnezhad
Second Review by: Loai Aljerf
Final Approval by: Dr. Patorn Piromchai
Fareedi Mukram Ali1, Ghassan M Iryani2, Mohammed Mousa Bakri1, Sultan Halawi3, Essa Mashyakhi3, Omar Darraj3, Abbas Hobani3
1 Department of Oral and Maxillofacial Surgery, College of Dentistry, Jazan University, Jazan, Kingdom of Saudi Arabia.
2 Faculty of Dentistry, Sana University, Consultant Oral and Maxillofacial Surgeon, Prince Mohammed bin Nasser Hospital, Ministry Of Health, Jazan, Kingdom of Saudi Arabia.
3 General Dental Practitioner, Ministry of Health, Jazan, Kingdom of Saudi Arabia.
Corresponding Author E-mail: faridi17@rediffmail.com
DOI : https://dx.doi.org/10.13005/bpj/2413
Abstract
To evaluate the alterations in blood pressure (BP) and heart rate (HR) among hypertensive and normotensive patients receiving dental local anesthesia using 2% lidocaine with epinephrine. This prospective observational study was carried out at the College of Dentistry, Jazan, KSA. A total of 40 adult patients were included in the study. They were divided into two groups (n=20). Group “A” included normotensive patients and group “B” included controlled hypertensive patients. The BP and HR were measured by a sphygmomanometer and pulse oximeter in three different temporal locations: on arrival to the waiting room, and in clinic before and after administration of local anesthesia. The mean values of the measurements in the three locations; the waiting area, clinic before and after the administration of DLA, were noted. The only significant alterations were found in the Systolic Blood Pressure (SBP) of both hypertensive and normotensive patients before the administration of DLA and in the HR of hypertensive patients again only before the administration of DLA. Endogenous catecholamines are more significant in causing hemodynamic disturbances in dental patients. Hypertensive patients seem to be more vulnerable to these disturbances.
Keywords
Blood Pressure; Epinephrine; Heart Rate; Hypertensive; Local Anesthesia; Normotensive
Download this article as:| Copy the following to cite this article: Ali F. M, Iryani G. M, Bakri M. M, Halawi S, Mashyakhi E, Darraj O, Hobani A. Evaluation of changes in Blood Pressure (BP) and Heart Rate (HR) among controlled Hypertensive and Normotensive Patients before and after receiving Dental Local Anesthesia (DLA) with Adrenaline: A Prospective Study. Biomed Pharmacol J 2022;15(2). |
| Copy the following to cite this URL: Ali F. M, Iryani G. M, Bakri M. M, Halawi S, Mashyakhi E, Darraj O, Hobani A. Evaluation of changes in Blood Pressure (BP) and Heart Rate (HR) among controlled Hypertensive and Normotensive Patients before and after receiving Dental Local Anesthesia (DLA) with Adrenaline: A Prospective Study. Biomed Pharmacol J 2022;15(2). Available from: https://bit.ly/3bDUIcb |
Introduction
Hypertension is becoming an important risk factor for cardiovascular disease worldwide1. One of the intriguing aspects of hypertension is that it remains asymptomatic and many patients are unaware of its presence 2. Studies in KSA have found that the prevalence of hypertension is high and rising. 3,4,5,6,7 The possible causes could be changing pattern of lifestyle, increased prevalence of obesity as well as changing the definition of hypertension to lower normal systolic values in recent guidelines8.
As far as the dental treatment is concerned, the utilization of local anesthesia is the main tool for pain control9. Incorporation of vasoconstrictors like epinephrine in local anesthesia increases the depth and duration of anesthesia and reduces bleeding in the operative field in cases of surgical procedures10, 11. The vasoconstrictor produces some side effects especially when it is absorbed systemically. The anxiety and stress due to dental treatment also cause secretion of endogenous catecholamines 12. It is rather difficult to differentiate if the undesirable side effects are due to the endogenous or exogenous catecholamines13.
Although the treatment protocol for hypertensive patients who are under control is not much changed, but dentists should be aware of the fact that systemic absorption of the agent can create side effects in hypertensive patients despite being within the safe dose range14.
We designed this study in an effort to measure the systolic, diastolic blood pressure and pulse rates at three moments of possible significant alterations among normotensive and controlled hypertensive patients to whom we deliver local anesthesia, in an attempt to evaluate the impact of both endogenous and exogenous catecholamines.
Aim of the study
To analyze the Systolic Blood Pressure (SBP), Diastolic Blood Pressure (DBP) and Heart rate (HR) of normotensive and controlled hypertensive patients before and after administration of local anesthesia with epinephrine. The collected data was used to analyze the effect of endogenous and exogenous catecholamines on the cardiovascular system.
Material and Methods
Study Design and Study Setting
This prospective observational study was carried in the Department of Oral Surgery at the College of Dentistry, Jazan, KSA. Informed written consent from all the participants was obtained. This study was carried in the male clinics and hence only male participants were selected. This study followed the World Medical Association Declaration of Helsinki. College ethical committee clearance was obtained with Institute registration number (IRB.2019/030).
Sample Selection Criteria
In this non-blinded study using convenient sampling technique, “Sample size was calculated based on the previously published study by ogunlewe MO et.al 15. Inclusion criteria were controlled Hypertensive patients with systolic blood pressure (SBP) not exceeding 140mmHg and diastolic blood pressure (DBP) not exceeding 95mmHg. Those undergoing elective oral surgical procedures under Local Anesthesia [(lignocaine 2% with epinephrine 1:100000) Lignospan® standard; Canada]. Age-matched normotensive patients acting as controls were also selected. Exclusion criteria were patients with uncontrolled hypertension, patients with other comorbidities like diabetes mellitus, or cardiovascular diseases other than hypertension and those not willing to participate in the study. Patients who needed more than one cartridge of DLA (1.8ml) were also excluded. Based on the inclusion and exclusion criteria a total of n=20 adult male hypertensive (Group A) and n=20 adult male normotensive patients (Group B) were included in the study.
Study Tools and Data Collection Method
The measurements of Blood pressure and Heart rate were done in three different temporal locations where there are possible chances of hemodynamic alterations. The first measurement was done upon arrival to the dental clinic and the patients will be in the waiting room. The second measurement was when the patient on the Dental chair just before the administration of local anesthesia. The third record was done within 5 minutes after the administration of local anesthesia. All the measurements of BP and HR were taken between 9 AM and 10 AM and the BP was measured by a standard calibrated and validated sphygmomanometer (Yuwell; China) after 5 minutes of rest (or after administration of local anesthesia) with the patient in sitting position with backrest, arm support, legs uncrossed and sphygmomanometer at the level of the heart.
For the validity and reliability of the study, the measurement of the variables such as blood pressure and heart rate were carried out using standardized procedures.
A single operator with the same instrument measured the BP of all the patients to avoid inter-operator bias. The pulse was measured with a pulse oximeter (Omron healthcare co. Ltd; Japan) applied to the left index finger. Two Oral & Maxillofacial surgeons with experience of more than 10 years performed the local anesthesia administration.
Statistical Analysis
The collected data was organized on an excel spreadsheet and statistical analysis was performed by SPSS version 17. Statistical software ANOVA analysis was used to find variations both within the same group and among all groups.
Results
Analysis of SBP changes in Normotensive Patients
The mean values of SBP in group A (Normotensive) in the three different temporal locations were calculated and recorded. It was 122.1 ± 8.27 mmHg in the waiting area, 128.15 ± 7.06 mmHg in the Dental clinic before the administration of local anesthesia and 122.3 ± 6.93 mmHg after the administration of local anesthesia. In order to determine the significance of the differences between the three mean values ANOVA analysis was used and the F value was found to be 2.58 and the F Critical values was 3.15 while the p value was 0.02 hence significant alterations were found. Namely in the SBP readings taken in the clinic just prior to the administration of DLA (Table 1).
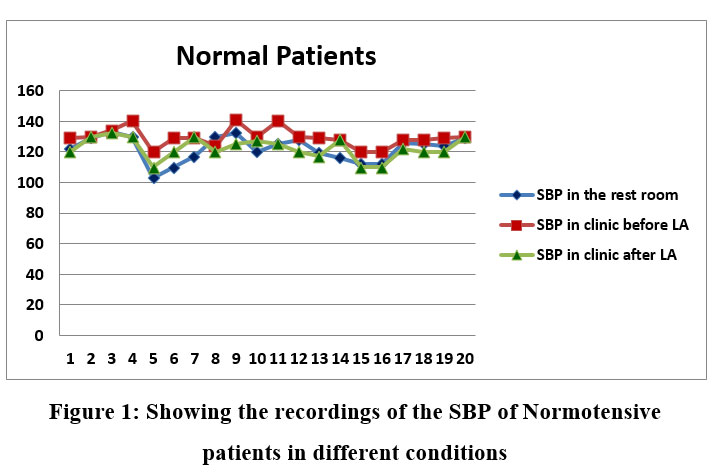 |
Figure 1: Showing the recordings of the SBP of Normotensive patients in different conditions. |
Table 1: ANOVA analysis of the Systolic Blood Pressure [SBP] of Normotensive Patients in the waiting area, in the clinic before LA and in the clinic after LA.
| Source of Variation | SS | df | MS | F | P-value | F crit |
| Between Groups | 691.6 | 2 | 345.8 | 6.804267 | 0.002239* | 3.158843 |
| Within Groups | 2896.8 | 57 | 50.82105 | |||
| Total | 3588.4 | 59 |
* P <0.05 significant
Analysis of DBP Changes in Normotensive Patients
The mean value of DBP in group A in the three different locations was calculated and recorded. In the restroom, the Mean DBP value was 80.8 ± 6.53 mmHg and the mean DBP value in the Dental clinic before the administration of Local Anesthesia was 79.65± 5.57 mmHg and the mean value of DBP after the administration of Local anesthesia was 78.6 ± 3.11mmHg. The ANOVA analysis was used and the F value was found to be 0.87 and the F Critical values were 3.15 the p values were found to be >0.87 hence the differences were not significant (Table 2).
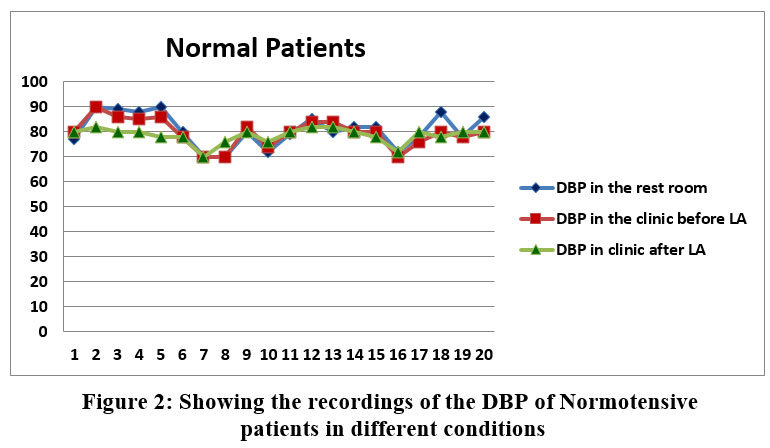 |
Figure 2: Showing the recordings of the DBP of Normotensive patients in different conditions. |
Table 2: ANOVA analysis of the Diastolic Blood Pressure [DBP] of Normotensive Patients in the restroom, in the clinic before LA and in the clinic after LA.
| Source of Variation | SS | df | MS | F | P-value | F crit |
| Between Groups | 48.43333 | 2 | 24.21667 | 0.870032 | 0.424426 | 3.158843 |
| Within Groups | 1586.55 | 57 | 27.83421 | |||
| Total | 1634.983 | 59 |
P > 0.05 not significant
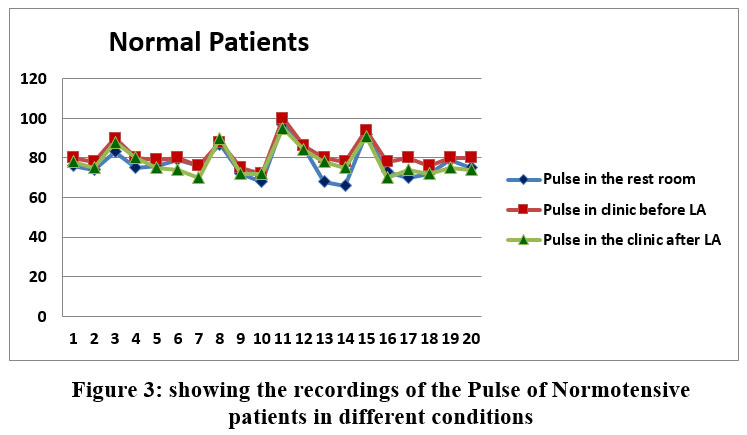 |
Figure 3: Showing the recordings of the Pulse of Normotensive patients in different conditions. |
Table 3: ANOVA analysis of the Pulse of Normotensive Patients in the restroom, in the clinic before LA and in the clinic after LA.
| Source of Variation | SS | df | MS | F | P-value | F crit |
| Between Groups | 209.2333 | 2 | 104.6167 | 1.865029 | 0.164221 | 3.158843 |
| Within Groups | 3197.35 | 57 | 56.09386 | |||
| Total | 3406.583 | 59 |
P > 0.05 not significant
Analysis of SBP changes in Controlled Hypertensive Patients
The mean values of SBP in group B (Hypertensive) in the three different locations were calculated and recorded. It was 121.35 ± 8.48mmHg in the waiting area, 135.45 ± 6.41 mmHg in the Dental clinic before the administration of Local Anesthesia and 128.35 ± 7.35 mmHg after the administration of Local anesthesia. The ANOVA analysis between the readings gave an F value of 17.87 and F Critical value 3.15, and a P value <0.001. Hence the alterations were found to be significant and again specifically in the readings just prior to the administration of the DLA(table 4).
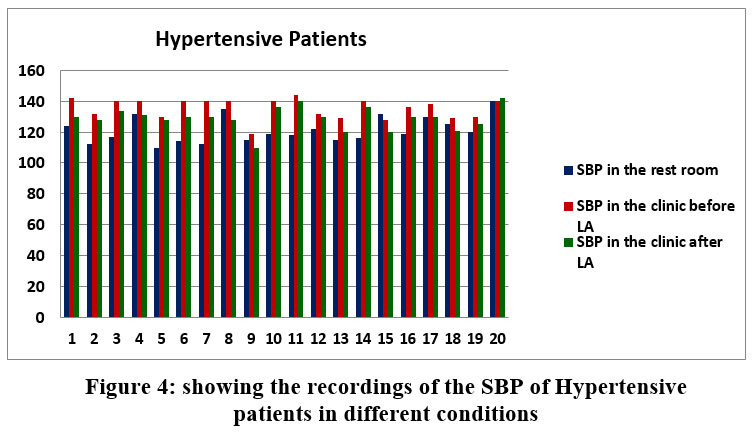 |
Figure 4: Showing the Recordings of the SBP of Hypertensive Patients in different Conditions. |
Table 4: ANOVA analysis of the Systolic Blood Pressure [SBP] of Hypertensive Patients in the Restroom, in the Clinic before LA and in the Clinic after LA.
| Source of Variation | SS | df | MS | F | P-value | F crit |
| Between Groups | 1992.133 | 2 | 996.0667 | 17.87398 | <0.001* | 3.158843 |
| Within Groups | 3176.45 | 57 | 55.72719 | |||
| Total | 5168.583 | 59 |
*Significant
Analysis of DBP Changes in Controlled Hypertensive Patients
The mean value of DBP in group B in the three different locations was calculated and recorded. In the restroom, the Mean DBP value was 88.05 ± 6.37 mmHg and the mean DBP value in the Dental clinic before the administration of DLA was 84.02 ± 8.67 mmHg and the mean value of DBP after the administration of DLA was 85.55 ± 8.66 mmHg. The ANOVA analysis between the readings shows an F value of 1.197998 and F Critical value 3.15, therefore, the P values was 0.3 indicating no significant alterations in the DBP in this group (table 5).
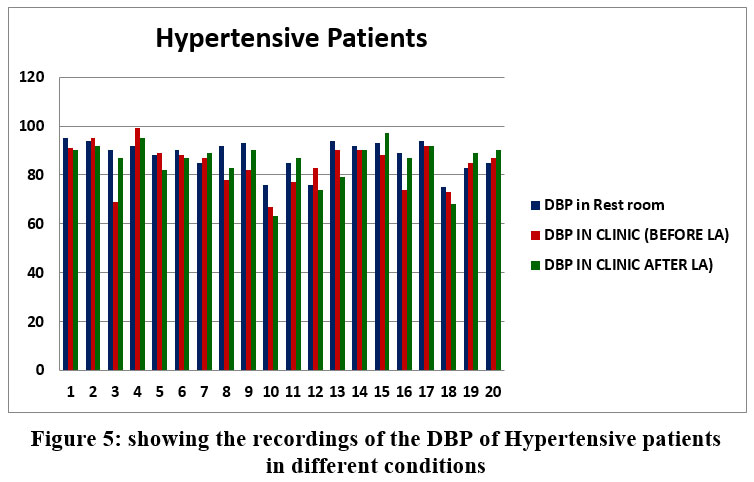 |
Figure 5: Showing the Recordings of the DBP of Hypertensive Patients in different Conditions. |
Table 5: ANOVA Analysis of the Diastolic Blood Pressure [DBP] of Hypertensive Patients in the restroom, in the Clinic before LA and in the Clinic after LA.
| Source of Variation | SS | df | MS | F | P-value | F crit |
| Between Groups | 152.6333 | 2 | 76.31667 | 1.197998 | 0.309282 | 3.158843 |
| Within Groups | 3631.1 | 57 | 63.70351 | |||
| Total | 3783.733 | 59 |
P = > 0.05 Not significant
Analysis of HR changes in Controlled Hypertensive Patients
The mean HR of group B (Hypertensive) in the three different conditions was calculated and recorded. In the restroom the Mean HR was found to be 81.55 ± 9.31 bpm and the mean HR in the Dental clinic before the administration of DLA was 90.4 ± 6.09 bpm and the mean HR after the administration of DLA was 81.85 ± 10.05 bpm. The ANOVA analysis between the groups shows the F value was 6.73 and F Critical value 3.15, therefore, the P value 0.002373 which was found to be significant. The significant alteration was agin in the readings at the clinic prior to the administration of the DLA. (table 6).
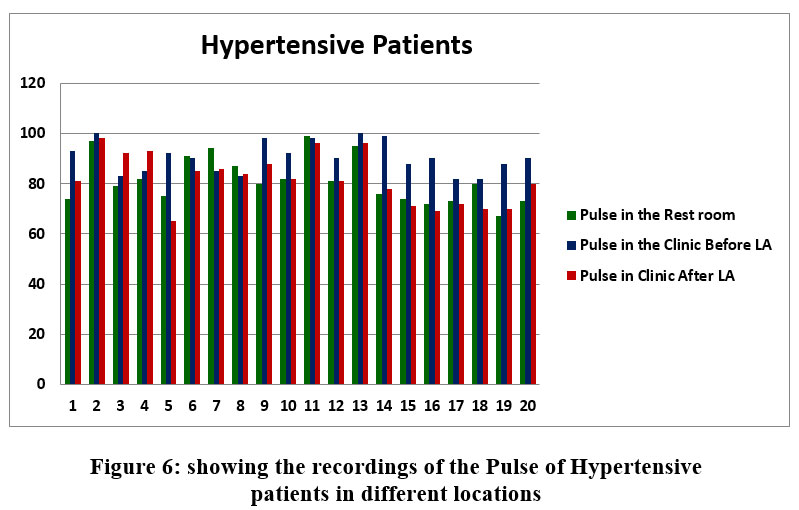 |
Figure 6: Showing the Recordings of the Pulse of Hypertensive Patients in different Locations. |
Table 6: ANOVA Analysis of the Pulse of Hypertensive Patients in the Restroom, in the Clinic before LA and in the Clinic after LA.
| Source of Variation | SS | df | MS | F | P-value | F crit |
| Between Groups | 1010.1 | 2 | 505.05 | 6.731953 | 0.002373* | 3.158843 |
| Within Groups | 4276.3 | 57 | 75.02281 | |||
| Total | 5286.4 | 59 |
*Significant
Discussion
Multiple studies have evaluated the effect of local anesthesia or different local anesthetic agents, with or without vasoconstrictor on hemodynamic parameters among normotensive and hypertensive patients 16,17,18,19,20,21,22. Adrinaline in local anesthesia has been used in dentistry especially in oral surgical procedures to increase the duration and depth of the anesthesia and to reduce the bleeding in the surgical field 23, 24, 25. This not only allows a better pain control but also avoids an exaggerated stress response.
Some studies have shown that while adrenaline as a vasoconstrictor is associated with transient effects in normotensive patients, hemodynamic complications could develop in uncontrolled hypertensive subjects, with possible cardiovascular accidents though such problems would be related to the dose of vasoconstrictor administered and to the local anesthesia used 22, 26.
In this study we used 2% lidocaine hydrochloride local anesthetic drug with 1:100000 epinephrine because of its extensive use in dental practice 27. Aspiration in two planes prior the local anesthesia injection was done to avoid intravascular injection in all the cases. Not a single case reported positive aspiration in our study.
The main aim of this study was to assess the changes in the B.P and H.R in controlled hypertensive patients before, and after administration of local anesthesia containing epinephrine and compare it with a control group (Normotensive patients).
In the present study, we found that the variations were significant in the Systolic Blood Pressure and Heart rate in Group B (controlled hypertensive patients) and only significant variation of group A (normotensive patients) was in the SBP.
In both groups the main variation was noted while the patient was on the dental chair before the administration of local anesthesia. This is explained by the psychological stress the patients had which leads to endogenous adrenaline secretion. The patient’s exposure to an unknown environment changes their physiological balance and causes the release of endogenous catecholamines which alter the blood pressures and heart rate 28,29,30,31. The hypertensive patients are more sensitive to adrenaline and this explains the rise of SBP and HR as compared to the normotensive group which had a significant rise only in the SBP 32.
Similar results were seen from the studies done by (Karanam AK. Reddy BS) 33, (Uzeda, M J) 16. They concluded that the rise in systolic blood pressure is attributed to the stress and anxiety of dental surgery characterizing the “white coat hypertension” and not because of the vasoconstrictor used in the local anesthesia. Whereas in contrast to our study, Shimoji et al34; found that there were no changes in BP or HR at any point of dental procedures and they found no significant difference between pre and post anesthesia period and during the local anesthesia.
The mean SBP in the normotensive patients before the injection of DLA was 128.15 mmHg and the mean SBP after the injection of DLA was 122.3 mmHg. This shows that the apprehension due to stress is present and after the injection of the local anesthetic the mean BP dropped due to the alleviation of stress.
A study by Chaudhary S. et.al19 on the effect on BP and Heart rate after local anesthesia in hypertensive patients found significant fall in DBP and SBP of patients with Hypertension from the time of administering injections up to five minutes. In the present study we observed that the mean BP in the hypertensive group prior to local anesthesia administration 135.45 mmHg and after the local anesthesia administration the mean SBP was 128.95 mmHg agreeing with the results of S Chaudhary et al 19.
Seeing alterations in the SBP but not in the DBP is well expected. Adrenaline induces an increase in SBP while reducing the DBP as explained by Struthers AD et.al35.
The main source of hemodynamic disturbances in hypertensive patients (and also normotensive patients) is the secretion of endogenous epinephrine36, 37. The ongoing debate on the use of vasoconstrictor with the local anesthetic solution in hypertensive patients doesn’t seem to be valid. The use of vasoconstrictors within a limit below the minimal therapeutic dose of 0.04mg of epinephrine with precautions to eliminate rapid systemic uptake would be advantageous 38, 39. Profound anesthesia (pain control) is crucial to prevent stress during treatment which would lead to secretion of catecholamines39. The cardiovascular effects caused by the use of adrenaline in hypertensive patients are negligible as compared to its benefits. It would be more sensible to move the debate into standardizing a protocol for stress reduction and stress assessment with encouragement to utilize anxiolytic medications.
Conclusion
Endogenous catecholamines are more significant in causing hemodynamic disturbances in patients undergoing dental procedures. Hypertensive patients are more vulnerable to these endogenous catecholamines . The precautious utilization of adrenaline supplemented local anesthetic preparations provide profound pain control for longer durations. A pain free experience reduces the stress and this is an important factor in reducing the secretion of catecholamines and hence preventing undesirable cardiovascular events. Precautious use of adrenaline should be strictly followed by avoiding intravascular injections and abiding by the allowed dose.
References
- Zhou, B., Perel, P., Mensah, G.A. et al. Global epidemiology, health burden and effective interventions for elevated blood pressure and hypertension. Nat Rev Cardiol; 18, 785–802 (2021). https://doi.org/10.1038/s41569-021-00559-8.
CrossRef - Greenland P, Knoll MD, Stamler J, Neaton JD, Dyer AR, Garside DB, et al. Major risk factors as antecedents of fatal and nonfatal coronary heart disease events. JAMA; 290(7): 89-7 (2003)
CrossRef - Nazim Uddin K. Prevalence of hypertension in Saudi Arabia. Practitioner East Mediterr Ed; 11: 805-806 (1994).
- Ahmed AF, Mahmoud ME. The prevalence of hypertension in Saudi Arabia. Saudi Med J; 13: 548-551(1992).
- Al-Shammari SA, Ali M, Al-Shammari A. Blood lipid concentrations and other cardiovascular risk factors among Saudis. Fam Pract; 11: 153-158 (1994).
CrossRef - Al-Nozha M, Ali M, Osman A. Arterial Hypertension in Saudi Arabia. Ann Saudi Med; 17: 170-174 (1997).
CrossRef - Mahfouz AA, Al Erian RA. Hypertension in Asir region, south western Saudi Arabia. An epidemiologic study. Southeast Asian J Trop Med Public Health; 24: 284-286 (1993).
- Mansour M. Al-Nozha, Moheeb Abdullah, Mohammed R. Arafah, Mohamed Z. Khalil, Nazeer B. Khan, Yaqoub Y. Al-Mazrou et al. Hypertension in Saudi Arabia. Saudi Med J; 28 (1): 77-84 (2007).
- Aljerf L, AlMasri N. Halothane Anesthesia – Fact or Fallacy? Int J Drug Disc; 2(1):2-7 (2018).
- Bader JD, Bonito AJ, Shugars DA. Cardiovascular Effects of Epinephrine in Hypertensive Dental Patients: Summary. 2002 Mar. In: AHRQ Evidence Report Summaries. Rockville (MD): Agency for Healthcare Research and Quality (US); 1998-2005. 48. Available from: https://www.ncbi.nlm.nih.gov/books/NBK11858/
- Sisk AL. Vasoconstrictors in local anesthesia for dentistry. Anesth Prog; 39(6):187-93(1992).
- Pérusse R, Goulet JP, Turcotte, J.Y. Contraindications to vasoconstrictors in dentistry: Part I. Cardiovascular diseases. Oral surgery, oral medicine, and oral pathology; 74(5):679-86 (1992).
CrossRef - Zhu BT. Catechol-O-Methyltransferase (COMT)-mediated methylation metabolism of endogenous bioactive catechols and modulation by endobiotics and xenobiotics: importance in pathophysiology and pathogenesis. Curr Drug Metab;3(3):321-49 (2002).
CrossRef - Bader JD, Bonito AJ, Shugars DA. A systematic review of the cardiovascular effects of epinephrine on hypertensive dental patients. Oral Surg Oral Med Oral Pathol Oral Radiol Endod; 93(6):647-53 (2002).
CrossRef - Ogunlewe MO, James O, Ajuluchukwu JN, Ladeinde AL, Adeyemo WL, Gbotolorun OM. Evaluation of haemodynamic changes in hypertensive patients during tooth extraction under local anaesthesia. West Indian Med J;60(1):91-5 (2011).
- Uzeda MJ, Moura B, Louro RS, da Silva LE, Calasans-Maia MD. A randomized controlled clinical trial to evaluate blood pressure changes in patients undergoing extraction under local anesthesia with vasopressor use. J Craniofac Surg; 25(3):1108-10 (2014)
CrossRef - Siddiqui HK, Hussain A, Khan FA, Shafi AM, Heyat U. Systemic effects of local anaesthesia in hypertensive patients. Pakistan Oral & Dental Journal; 37(4): 539-542 (2017).
- Muhammad I, Zupash A K, Ibrahim K, Akif Z, Kainat I, Jawad A. The Effect of Local Anesthesia (Lidocaine 2%) with Epinephrine (1:100,000) On Blood Pressure Level of Hypertensive Patients Reported To a Tertiary Care Hospital, Peshawar.Pakistan. Biomed J Sci & Tech Res; 1(6): 1687-1691 (2017).
CrossRef - Chaudhry S, Iqbal HA, Izhar F, Mirza KM, Khan NF, Yasmeen R, Khan AA. Effect on blood pressure and pulse rate after administration of an epinephrine containing dental local anaesthetic in hypertensive patients. J Pak Med Assoc; 61(11):1088-91 (2011).
- Ezmek B, Arslan A, Delilbasi C, Sencift K. Comparison of hemodynamic effects of lidocaine, prilocaine and mepivacaine solutions without vasoconstrictor in hypertensive patients. J Appl Oral Sci; 18(4):354-9 (2010).
CrossRef - Abu-Mostafa N, Al-Showaikhat F, Al-Shubbar F, Al-Zawad K, Al-Zawad F. Hemodynamic changes following injection of local anesthetics with different concentrations of epinephrine during simple tooth extraction: a prospective randomized clinical trial. J Clin Exp Dent.;7(4):e471–e476 (2015)
CrossRef - Akinmoladun VI, Okoje VN, Akinosun OM, Adisa AO, Uchendu OC. Evaluation of the haemodynamic and metabolic effects of local anaesthetic agent in routine dental extractions. J Maxillofac Oral Surg.; 12(4):424-428 (2013).
CrossRef - Karm MH, Kim M, Park FD, Seo KS, Kim HJ. Comparative evaluation of the efficacy, safety, and hemostatic effect of 2% lidocaine with various concentrations of epinephrine. J Dent Anesth Pain Med. 2018 Jun; 18(3):143-149 (2018).
CrossRef - Balakrishnan R, Ebenezer V. Contraindications of Vasoconstrictors in Dentistry. Biomed Pharmacol J; 6(2):409-414 (2013).
CrossRef - Southerland JH, Gill DG, Gangula PR, Halpern LR, Cardona CY, Mouton CP. Dental management in patients with hypertension: challenges and solutions. Clin Cosmet Investig Dent.; 8:111-120 (2016).
CrossRef - Silvestre FJ, Isabel SM, Bautista D, Javier SR. Clinical study of hemodynamic changes during extraction in controlled hypertensive patients. Med Oral Patol Oral Cir Bucal.; 16(3):e354-8 (2011).
CrossRef - Corbett IP, Ramacciato JC, Groppo FC, Meechan JG. A survey of local anaesthetic use among general dental practitioners in the UK attending postgraduate courses on pain control. Br Dent J.; 199:784-7 (2005).
CrossRef - Bronzo AL, Cardoso CG Jr, Ortega KC, Mion D Jr. Felypressin increases blood pressure during dental procedures in hypertensive patients. Arq Bras Cardiol.;99(2):724-31 (2012).
CrossRef - Sanadhya YK, Sandhya S, Jalihal S, Nagarajappa R, Ramesh G, Tak M. Hemodynamic, ventilator, and ECG changes in pediatric patients undergoing extraction. J Indian Soc Pedod Prev Dent.; 31(1):10-6 (2013).
CrossRef - Holroyd SV, Watts DT, Welch JT. The use of epinephrine in local anesthetics for dental patients with cardiovascular disease: a review of the literature. J Oral Surg Anesth Hosp Dent Serv.; 18:492-503 (1960).
- Montebugnoli L, Prati C. Circulatory dynamics during dental extractions in normal, cardiac and transplant patients. J Am Dent Assoc.; 133(4):468-72 (2002).
CrossRef - Niwa H, Sugimura M, Satoh Y, Tanimoto A. Cardiovascular response to epinephrine-containing local anesthesia in patients with cardiovascular disease. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontics. 92(6):610-616 (2001).
CrossRef - Karanam AK, Reddy BS. Effects of lignocaine with adrenaline on blood pressure and pulse rate in normotensive and hypertensive patients undergoing extraction: A clinical study. Journal of Oral Medicine, Oral Surgery, Oral Pathology and Oral Radiology; 3(4):202-204 (2017).
- Shimaoji S, Odanaka H, Takefu H, et al; Influence of Local Anesthesia on Autonomic Nervous activity in healthy young adults evaluation of Heart Rate Variability. Dentistry 6(5): 378 (2016).
CrossRef - Struthers AD, Reid JL, Whitesmith R, Rodger JC. Effect of intravenous adrenaline on electrocardiogram, blood pressure, and serum potassium. Br Heart J.;49(1):90-3. (1983)
CrossRef - Aljerf L, Alhaffar I. ” Aljerf L. and Alhaffar I. Salivary distinctiveness and modifications in males with Diabetes and Behçet’s disease. Biochemistry Research International; 1–12 (2017).
CrossRef - Laragh JH, Angers M, Kelly WG, Lieberman S. Hypotensive Agents and Pressor Substances. The Effect of Epinephrine, Norepinephrine, Angiotensin II, and Others on the Secretory Rate of Aldosterone in Man. JAMA.; 174(3):234–240 (1960)
CrossRef - Holm SW, Cunningham LL, Jr, Bensadoun E, Madsen MJ. Hypertension: classification, pathophysiology, and management during outpatient sedation and local anesthesia. J Oral Maxillofac Surg.;64(1):111–121 (2006)
CrossRef - Little J, Falace D, Miller C, Rhodus N. Dental Management of the Medically Compromised Patient. 6th ed. St. Louis: Mosby; 2002.

