
Abstract
Background
Systemic therapy is an essential part of treatment for pancreatic ductal adenocarcinoma (PDAC). However, not all patients receive every cycle of chemotherapy and even if they do, the impact of reduced dose density (DD) on survival is not known.
Patients and Methods
A single institutional prospective database was queried for patients with PDAC who underwent curative resection between 2009 and 2018. The primary outcome was DD, defined as the percentage of total planned chemotherapy actually received and associated survival.
Results
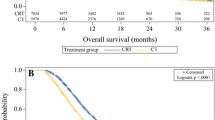
Of the 126 patients included, 38.9% underwent a neoadjuvant approach, which was associated with a greater median number of completed chemotherapy cycles (5 cycles versus 4 cycles, p < 0.01) and a higher median total DD (93.0% versus 65.0%, p < 0.01), compared with an adjuvant treatment approach. In both groups, adjuvant chemotherapy completion rates were low, with only 55 patients completing all adjuvant cycles. After sequential survival analysis, patients who received a DD ≥ 80% had improved median overall survival (OS) (27.1 months versus 18.6 months, p = 0.01), compared with patients who achieved a DD < 80%. On multivariate Cox proportional-hazards modeling, only the presence of lymphovascular invasion (HR: 1.77, 95% CI: 1.04–2.99, p = 0.04) and DD < 80% (HR: 1.91, 95% CI: 1.23–3.00, p = 0.01) were associated with decreased OS.
Conclusions
In this cohort study, patients who received ≥ 80% DD had significantly better OS. DD should be considered an important prognostic metric in pancreatic cancer, and strategies are needed to improve chemotherapy tolerance to improve patient outcomes.



Similar content being viewed by others


References
Neoptolemos JP, Stocken DD, Friess H, et al. A randomized trial of chemoradiotherapy and chemotherapy after resection of pancreatic cancer. NEJM. 2004;350(12):1200–10.
Tzeng CW, Tran Cao HS, Lee JE, et al. Treatment sequencing for resectable pancreatic cancer: influence of early metastases and surgical complications on multimodality therapy completion and survival. J Gastrointest Surg. 2014; 18(1):16-24; discussion 24–15.
Conroy T, Desseigne F, Ychou M, et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. NEJM. 2011;364(19):1817–25.
Von Hoff DD, Ervin T, Arena FP, et al. Increased survival in pancreatic cancer with nab-paclitaxel plus gemcitabine. NEJM. 2013;369(18):1691–703.
Conroy T, Hammel P, Hebbar M, et al. FOLFIRINOX or Gemcitabine as Adjuvant Therapy for Pancreatic Cancer. NEJM. 2018;379(25):2395–406.
Sohal DPS, Duong M, Ahmad SA, et al. Efficacy of perioperative chemotherapy for resectable pancreatic adenocarcinoma: a phase 2 randomized clinical trial. JAMA Oncol. 2021;7(3):421–7.
Altman AM, Wirth K, Marmor S, et al. Completion of adjuvant chemotherapy after upfront surgical resection for pancreatic cancer is uncommon yet associated with improved survival. Ann Surg Oncol. 2019;26(12):4108–16.
Merkow RP, Bilimoria KY, Tomlinson JS, et al. Postoperative complications reduce adjuvant chemotherapy use in resectable pancreatic cancer. Ann Surg. 2014;260(2):372–7.
Neoptolemos JP, Moore MJ, Cox TF, et al. Effect of adjuvant chemotherapy with fluorouracil plus folinic acid or gemcitabine vs observation on survival in patients with resected periampullary adenocarcinoma: the ESPAC-3 periampullary cancer randomized trial. JAMA. 2012;308(2):147–56.
Valle JW, Palmer D, Jackson R, et al. Optimal duration and timing of adjuvant chemotherapy after definitive surgery for ductal adenocarcinoma of the pancreas: ongoing lessons from the ESPAC-3 study. J Clin Oncol. 2014;32(6):504–12.
Liutkauskiene S, Grizas S, Jureniene K, Suipyte J, Statnickaite A, Juozaityte E. Retrospective analysis of the impact of anthracycline dose reduction and chemotherapy delays on the outcomes of early breast cancer molecular subtypes. BMC Cancer. 20 2018;18(1):453.
Veitch Z, Khan OF, Tilley D, et al. Impact of cumulative chemotherapy dose on survival with adjuvant FEC-D chemotherapy for breast cancer. J Natl Compr Canc Netw. 2019;17(8):957–67.
Al-Hawary MM, Francis IR, Chari ST, et al. Pancreatic ductal adenocarcinoma radiology reporting template: consensus statement of the society of abdominal radiology and the american pancreatic association. Gastroenterology. 2014;146(1):291-304.e291.
Network NCC. Pancreatic Cancer (Version 1.2021); https://www.nccn.org/professionals/physician_gls/pdf/pancreatic_blocks.pdf. Accessed January 22, 2021.
Semega JKM, Schrider EA, Creamer JF, U.S. Census Bureau, Current Populations Report. Vol Income and Poverty in the United States: 2019: U.S. Government Publishing Office, Washington, D.C.; 2020:60–270.
Income by Zip Code. https://www.incomebyzipcode.com. Accessed January 15th, 2020.
Maggino L, Malleo G, Marchegiani G, et al. Outcomes of primary chemotherapy for borderline resectable and locally advanced pancreatic ductal adenocarcinoma. JAMA Surg. 2019;154(10):932–42.
Truty MJ, Kendrick ML, Nagorney DM, et al. Factors predicting response, perioperative outcomes, and survival following total neoadjuvant therapy for borderline/locally advanced pancreatic cancer. Ann Surg. 5 2019.
Neoptolemos JP, Palmer DH, Ghaneh P, et al. Comparison of adjuvant gemcitabine and capecitabine with gemcitabine monotherapy in patients with resected pancreatic cancer (ESPAC-4): a multicentre, open-label, randomised, phase 3 trial. Lancet. 2017;389(10073):1011–24.
Uesaka K, Boku N, Fukutomi A, et al. Adjuvant chemotherapy of S-1 versus gemcitabine for resected pancreatic cancer: a phase 3, open-label, randomised, non-inferiority trial (JASPAC 01). Lancet. 2016;388(10041):248–57.
Oettle H, Neuhaus P, Hochhaus A, et al. Adjuvant chemotherapy with gemcitabine and long-term outcomes among patients with resected pancreatic cancer: the CONKO-001 randomized trial. Jama. 2013;310(14):1473–81.
Lee JC, Kim JW, Ahn S, et al. Optimal dose reduction of FOLFIRINOX for preserving tumour response in advanced pancreatic cancer: using cumulative relative dose intensity. Eur J Cancer. 2017;76:125–33.
Murphy JE, Wo JY, Ryan DP, et al. Total neoadjuvant therapy with FOLFIRINOX followed by individualized chemoradiotherapy for borderline resectable pancreatic adenocarcinoma: a phase 2 clinical trial. JAMA oncology. 2018;4(7):963–9.
Acknowledgements
The authors have no acknowledgements.
Funding
The authors have no grants or financial support to report.
Author information
Authors and Affiliations
Contributions
Davendra Sohal: Speakers Bureau Incyte and Genentech. The Institution: research funding Amgen, Apexigen, Bristol-Myers Squibb, Celgene, FibroGen, Genentech, Medimmune, Merck, OncoMed, and Rafael.
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Turner, K.M., Delman, A.M., Vaysburg, D.M. et al. Systemic Therapy for Resected Pancreatic Adenocarcinoma: How Much is Enough?. Ann Surg Oncol 29, 3463–3472 (2022). https://doi.org/10.1245/s10434-022-11363-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-022-11363-0