
Abstract
Background
Patients with localized pancreatic cancer (PC) can develop acute cholecystitis during neoadjuvant therapy; optimal management remains undefined.
Methods
Consecutive patients with localized PC who had indwelling biliary stents and received neoadjuvant therapy were reviewed. Time from stent placement to the development of acute cholecystitis was calculated. Patients were categorized as having surgical versus nonoperative management of cholecystitis. Time to PC resection was defined as the time from the start of treatment to pancreatic resection.
Results
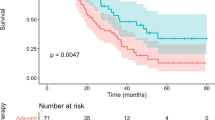
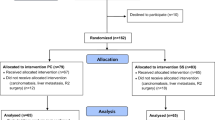
Of the 283 patients with indwelling biliary stents, acute cholecystitis occurred in 17 (6%) patients. The median time from the date of stent placement to the development of cholecystitis was 2.3 months [interquartile range (IQR) 4.6 months]. Acute cholecystitis was managed with cholecystostomy tube placement in 15 (88%) patients and cholecystectomy in 2 (12%). In total, 189 (67%) of the 283 patients completed all intended neoadjuvant therapy and surgery; 10 (59%) of the 17 patients with cholecystitis (10 of 15 managed with a cholecystostomy tube and 0 of 2 managed with cholecystectomy) and 179 (67%) of the 266 patients without cholecystitis (p = 0.47). The median time to PC resection was 3.2 months for the 179 patients without cholecystitis and 3.6 months for the 10 patients with cholecystitis (p = 1.00).
Conclusions
Acute cholecystitis occurred in 6% of patients with indwelling biliary stents during neoadjuvant therapy. Management with a cholecystostomy tube did not delay the completion of neoadjuvant therapy and surgery and should be considered the optimal management of this complication.


Similar content being viewed by others

References
Dimou F, Sineshaw H, Parmar AD, Tamirisa NP, Jemal A, Riall TS. Trends in receipt and timing of multimodality therapy in early-stage pancreatic cancer. J Gastrointest Surg 2016;20:93–103 (discussion).
Evans DB, Varadhachary GR, Crane CH, et al. Preoperative gemcitabine-based chemoradiation for patients with resectable adenocarcinoma of the pancreatic head. J Clin Oncol. 2008;26:3496–502.
Tsai S, Christians KK, George B, et al. A phase II clinical trial of molecular profiled neoadjuvant therapy for localized pancreatic ductal adenocarcinoma. Ann Surg. 2018;268:610-9.
Van Tienhoven G, Versteijne E, Suker M, Groothuis KB, Busch OR, Bonsing BA et al. Preoperative chemoradiotherapy versus immediate surgery for resectable and borderline resectable pancreatic cancer (PREOPANC-1): a randomized, controlled, multicenter phase III trial. J Clin Oncol. 2018; 36:LBA4002.
Christians KK, Heimler JW, George B, et al. Survival of patients with resectable pancreatic cancer who received neoadjuvant therapy. Surgery 2016;159:893–900.
Christians KK, Tsai S, Mahmoud A, et al. Neoadjuvant FOLFIRINOX for borderline resectable pancreas cancer: a new treatment paradigm? Oncologist 2014;19:266–74.
Miura JT, Krepline AN, George B, et al. Use of neoadjuvant therapy in patients 75 years of age and older with pancreatic cancer. Surgery 2015;158:1545–55.
Suk KT, Kim HS, Kim JW, et al. Risk factors for cholecystitis after metal stent placement in malignant biliary obstruction. Gastrointest Endosc. 2006;64:522–9.
Shimizu S, Naitoh I, Nakazawa T, et al. Predictive factors for pancreatitis and cholecystitis in endoscopic covered metal stenting for distal malignant biliary obstruction. J Gastroenterol Hepatol. 2013;28:68–72.
Appel BL, Tolat P, Evans DB, Tsai S. Current staging systems for pancreatic cancer. Cancer 2012;18:539–49.
Papi C, Catarci M, D’Ambrosio L, et al. Timing of cholecystectomy for acute calculous cholecystitis: a meta-analysis. Am J Gastroenterol. 2004;99:147–55.
Gurusamy KS, Davidson C, Gluud C, Davidson BR. Early versus delayed laparoscopic cholecystectomy for people with acute cholecystitis. Cochrane Database Syst Rev. 2013; 6:CD005440.
Decker C, Christein JD, Phadnis MA, Wilcox CM, Varadarajulu S. Biliary metal stents are superior to plastic stents for preoperative biliary decompression in pancreatic cancer. Surg Endosc. 2011;25:2364–7.
Aadam AA, Evans DB, Khan A, Oh Y, Dua K. Efficacy and safety of self-expandable metal stents for biliary decompression in patients receiving neoadjuvant therapy for pancreatic cancer: a prospective study. Gastrointest Endosc. 2012;76:67–75.
Mullen JT, Lee JH, Gomez HF, et al. Pancreaticoduodenectomy after placement of endobiliary metal stents. J Gastrointest Surg. 2005;9:1094–104 (discussion 104-5).
Lillemoe KD, Pitt HA, Kaufman SL, Cameron JL. Acute cholecystitis occurring as a complication of percutaneous transhepatic drainage. Surg Gynecol Obstet. 1989;168:348–52.
Nakai Y, Isayama H, Kawakubo K, et al. Metallic stent with high axial force as a risk factor for cholecystitis in distal malignant biliary obstruction. J Gastroenterol Hepatol. 2014;29:1557–62.
Katabathina VS, Zafar AM, Suri R. Clinical presentation, imaging, and management of acute cholecystitis. Tech Vasc Interv Radiol. 2015;18:256–65.
Alvino DML, Fong ZV, McCarthy CJ, et al. Long-term outcomes following percutaneous cholecystostomy tube placement for treatment of acute calculous cholecystitis. J Gastrointest Surg. 2017;21:761–9.
Funding
We Care Fund for Medical Innovation and Research, Ronald Burklund Eich Pancreatic Cancer Research Fund, Association of VA Surgeons Karl Storz Research Grant.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
None.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Jariwalla, N.R., Khan, A.H., Dua, K. et al. Management of Acute Cholecystitis during Neoadjuvant Therapy in Patients with Pancreatic Adenocarcinoma. Ann Surg Oncol 26, 4515–4521 (2019). https://doi.org/10.1245/s10434-019-07906-7
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-019-07906-7