
Abstract
Background
Normocalcemic (incipient) primary hyperparathyroidism (PHPT) is characterized by inappropriately elevated parathyroid hormone (PTH) levels in the setting of normal serum calcium. The biochemical and skeletal outcomes after parathyroidectomy for normocalcemic PHPT are not well-described.
Methods
All patients who underwent parathyroidectomy for normocalcemic PHPT at a single institution were retrospectively reviewed (2006–2016). Pre- and postoperative calcium, PTH, and bone mineral density (BMD) were compared between patients with normalized versus persistently elevated PTH levels > 6 months after parathyroidectomy. Multivariable Cox regression was used to identify risk factors associated with persistently elevated PTH levels after parathyroidectomy.
Result
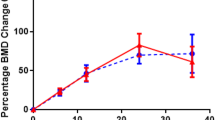
Parathyroidectomy was performed in 71 patients with normocalcemic PHPT, of whom 38 (53.5%) had multi-gland disease. No patients became hypercalcemic, with a median follow-up of 23.1 months. Persistently elevated PTH levels were noted in 33 (46.5%) patients. In multivariable analysis, preoperative PTH > 100 pg/mL was associated with persistently elevated PTH levels after parathyroidectomy. In 38 patients with available pre- and postoperative BMD measurements, the mean preoperative BMD improved + 5.6% (p < 0.01) in patients with normalized PTH, while no significant change was observed in patients with persistently elevated PTH levels (− 2.2%, p = 0.47).
Conclusions
Elevated PTH levels are common after parathyroidectomy for normocalcemic PHPT. Improvements in BMD may be predicated on long-term normalized PTH levels following surgery.


Similar content being viewed by others


References
Yeh MW, Ituarte PH, Zhou HC, et al. Incidence and prevalence of primary hyperparathyroidism in a racially mixed population. J Clin Endocrinol Metab. 2013;98(3):1122–9.
Lowe H, McMahon DJ, Rubin MR, Bilezikian JP, Silverberg SJ. Normocalcemic primary hyperparathyroidism: further characterization of a new clinical phenotype. J Clin Endocrinol Metab. 2007;92(8):3001–5.
Udelsman R, Pasieka JL, Sturgeon C, Young JE, Clark OH. Surgery for asymptomatic primary hyperparathyroidism: proceedings of the third international workshop. J Clin Endocrinol Metab. 2009;94(2):366–72.
Wade TJ, Yen TW, Amin AL, Wang TS. Surgical management of normocalcemic primary hyperparathyroidism. World J Surg. 2012;36(4):761–6.
Koumakis E, Souberbielle JC, Sarfati E, et al. Bone mineral density evolution after successful parathyroidectomy in patients with normocalcemic primary hyperparathyroidism. J Clin Endocrinol Metab. 2013;98(8):3213–20.
Yeh MW, Zhou H, Adams AL, et al. The Relationship of Parathyroidectomy and Bisphosphonates With Fracture Risk in Primary Hyperparathyroidism: An Observational Study. Ann Intern Med. 2016;164(11):715–23.
Bilezikian JP, Brandi ML, Eastell R, et al. Guidelines for the management of asymptomatic primary hyperparathyroidism: summary statement from the Fourth International Workshop. J Clin Endocrinol Metab. 2014;99(10):3561–9.
Calvi LM, Bushinsky DA. When is it appropriate to order an ionized calcium? Journal of the American Society of Nephrology. 2008;19(7):1257–60.
Udelsman R. Six hundred fifty-six consecutive explorations for primary hyperparathyroidism. Ann Surg. 2002;235(5):665–70; discussion 670–2.
Westerdahl J, Bergenfelz A. Unilateral versus bilateral neck exploration for primary hyperparathyroidism: five-year follow-up of a randomized controlled trial. Ann Surg. 2007;246(6):976–80; discussion 980–1.
Ning L, Sippel R, Schaefer S, Chen H. What is the clinical significance of an elevated parathyroid hormone level after curative surgery for primary hyperparathyroidism? Ann Surg. 2009;249(3):469–72.
Carsello CB, Yen TW, Wang TS. Persistent elevation in serum parathyroid hormone levels in normocalcemic patients after parathyroidectomy: does it matter? Surgery. 2012;152(4):575–81; discussion 581–3.
Goldfarb M, Gondek S, Irvin GL, Lew JI. Normocalcemic parathormone elevation after successful parathyroidectomy: long-term analysis of parathormone variations over 10 years. Surgery. 2011;150(6):1076–84.
Yen TW, Wilson SD, Krzywda EA, Sugg SL. The role of parathyroid hormone measurements after surgery for primary hyperparathyroidism. Surgery. 2006;140(4):665–72; discussion 672–4.
Wilhelm SM, Wang TS, Ruan DT, et al. The American Association of Endocrine Surgeons Guidelines for Definitive Management of Primary Hyperparathyroidism. JAMA Surg. 2016;151(10):959–68.
Lee DTW, Chabot JA, Lee JA, Kuo JH. Bone Mineral Density Changes After Curative Parathyroidectomy: An Analysis of Patients with Primary Hyperparathyroidism According to Biochemical Profiles. American Association of Endocrine Surgeons Annual Meeting; 6 May 2018; Durham, NC.
Maruani G, Hertig A, Paillard M, Houillier P. Normocalcemic primary hyperparathyroidism: evidence for a generalized target-tissue resistance to parathyroid hormone. J Clin Endocrinol Metab. 2003;88(10):4641–8.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Sho, S., Kuo, E.J., Chen, A.C. et al. Biochemical and Skeletal Outcomes of Parathyroidectomy for Normocalcemic (Incipient) Primary Hyperparathyroidism. Ann Surg Oncol 26, 539–546 (2019). https://doi.org/10.1245/s10434-018-6998-0
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-018-6998-0