
Abstract
Background
Adrenocortical carcinoma (ACC) is a rare and aggressive cancer. This report describes factors and outcomes associated with resection of extra-adrenal organs en bloc during index adrenalectomy.
Methods
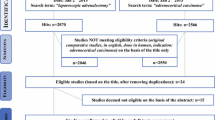
Patients who underwent ACC resection for non-metastatic disease from 1993 to 2014 at 13 participating institutions of the US-ACC Group were included in the study. Factors associated with en bloc resection were assessed by uni- and multivariate analysis. The primary end point was overall survival.
Results
In this study, 167 patients were included and categorized as adrenalectomy with en bloc resection (AdEBR) if they had extra-adrenal organs removed or adrenalectomy (Ad) if they did not. The demographics were similar between the AdEBR (n = 68, 40.7%) and Ad groups, including age, gender, race, American Society of Anesthesiology (ASA) class, and body mass index (BMI). The AdEBR group had larger tumors (13 vs. 10 cm), more open operations (97.1 vs. 63.6%), and more lymph node dissections (LNDs) (36.8 vs. 12.1%). The most common organs removed were kidney (55.9%), liver (27.9%), and spleen (23.5%). Multiple organs were removed in 38.2% (n = 26) of the patients. Margin-negative resections were similar between the two groups. In the multivariate Cox regression adjusted for T and N stages, LND, margin, size, and hormone hypersecretion, en bloc resection was not associated with improved survival (hazard ratio [HR], 1.42; p = 0.323).
Conclusion
The study findings validated current practice by showing that en bloc resection should occur at index adrenalectomy for ACC when a T4 lesion is suspected pre- or intraoperatively, or when it is necessary to avoid tumor rupture. However, in this study, when a negative margin resection was otherwise achieved, removal of extra-adrenal organs en bloc was not associated with additional survival benefit.

Similar content being viewed by others


References
Bilimoria KY, Shen WT, Elaraj D, et al. Adrenocortical carcinoma in the United States. Cancer. 2008;113:3130–6. https://doi.org/10.1002/cncr.23886.
Kebebew E, Reiff E, Duh Q-Y, Clark OH, McMillan A. Extent of disease at presentation and outcome for adrenocortical carcinoma: Have we made progress? World J Surg. 2006;30:872–8. https://doi.org/10.1007/s00268-005-0329-x.
Icard P, Goudet P, Charpenay C, et al. Adrenocortical carcinomas: surgical trends and results of a 253-patient series from the French Association of Endocrine Surgeons study group. World J Surg. 2001;25:891–7. https://doi.org/10.1007/s00268-001-0047-y.
LaFemina J, Brennan MF. Adrenocortical carcinoma: past, present, and future. J Surg Oncol. 2012;106:586–94. https://doi.org/10.1002/jso.23112.
Gaujoux S, Weinandt M, Bonnet S, Reslinger V, Bertherat J, Dousset B. Surgical treatment of adrenal carcinoma. J Visc Surg. 2017;154:335–43. https://doi.org/10.1016/j.jviscsurg.2017.06.010.
Sidhu S, Sywak M, Robinson B, Delbridge L. Adrenocortical cancer: recent clinical and molecular advances. Curr Opinion Oncol. 2003;16:13–8.
Ayala-Ramirez M, Jasim S, Feng L, et al. Adrenocortical carcinoma: clinical outcomes and prognosis of 330 patients at a tertiary care center. Eur J Endocrinol. 2013;169:891–9. https://doi.org/10.1530/eje-13-0519.
Schulick RD, Brennan MF. Long-term survival after complete resection and repeat resection in patients with adrenocortical carcinoma. Ann Surg Oncol. 1999;6:719–26.
Kendrick ML, Lloyd R, Erickson L, et al. Adrenocortical carcinoma: Surgical progress of status quo? Arch Surg. 2001;136:543–9.
Mihai R. Diagnosis, treatment, and outcome of adrenocortical cancer. Br J Surg. 2015;102:291–306. https://doi.org/10.1002/bjs.9743.
Margonis GA, Kim Y, Prescott JD, et al. Adrenocortical carcinoma: impact of surgical margin status on long-term outcomes. Ann Surg Oncol. 2015;23:134–41. https://doi.org/10.1245/s10434-015-4803-x.
Chagpar R, Siperstein AE, Berber E. Adrenocortical cancer update. Surg Clin North Am. 2014;94:669–87. https://doi.org/10.1016/j.suc.2014.02.009.
Hermsen I, Kerkhofs T, Butter den G, et al. Surgery in adrenocortical carcinoma: importance of national cooperation and centralized surgery. Surgery. 2012;152:50–6. https://doi.org/10.1016/j.surg.2012.02.005.
Livhits M, Li N, Yeh MW, Harari A. Surgery is associated with improved survival for adrenocortical cancer, even in metastatic disease. Surgery. 2014;156:1531–41. https://doi.org/10.1016/j.surg.2014.08.047.
Fassnacht M, Johanssen S, Fenske W, et al. Improved survival in patients with stage II adrenocortical carcinoma followed up prospectively by specialized centers. J Clin Endocrinol Metab. 2010;95:4925–32. https://doi.org/10.1210/jc.2010-0803.
Lombardi CP, Raffaelli M, Boniardi M, et al. Adrenocortical carcinoma: effect of hospital volume on patient outcome. Langenbecks Arch Surg. 2011;397:201–7. https://doi.org/10.1007/s00423-011-0866-8.
Gaujoux S, Brennan MF. Clinical review recommendation for standardized surgical management of primary adrenocortical carcinoma. Surgery. 2012;152:123–32. https://doi.org/10.1016/j.surg.2011.09.030.
Grubbs EG, Callender GG, Xing Y, et al. Recurrence of adrenal cortical carcinoma following resection: surgery alone can achieve results equal to surgery plus mitotane. Ann Surg Oncol. 2009;17:263–70. https://doi.org/10.1245/s10434-009-0716-x.
Ip JCY, Pang TCY, Glover AR, et al. Improving outcomes in adrenocortical cancer: an Australian perspective. Ann Surg Oncol. 2014;22:2309–16. https://doi.org/10.1245/s10434-014-4133-4.
Miller BS, Gauger PG, Hammer GD, Doherty GM. Resection of adrenocortical carcinoma is less complete and local recurrence occurs sooner and more often after laparoscopic adrenalectomy than after open adrenalectomy. Surgery. 2012;152:1150–7. https://doi.org/10.1016/j.surg.2012.08.024.
Cooper AB, Habra MA, Grubbs EG, et al. Does laparoscopic adrenalectomy jeopardize oncologic outcomes for patients with adrenocortical carcinoma? Surg Endosc. 2013;27:4026–32. https://doi.org/10.1007/s00464-013-3034-0.
Huynh KT, Lee DY, BJ L, Flaherty DC, Lee J, Goldfarb M. Impact of laparoscopic adrenalectomy on overall survival in patients with nonmetastatic adrenocortical carcinoma. J Am Coll Surg. 2016;223:485–92. https://doi.org/10.1016/j.jamcollsurg.2016.05.015.
Gerry JM, Tran TB, Postlewait LM, et al. Lymphadenectomy for adrenocortical carcinoma: Is there a therapeutic benefit? Ann Surg Oncol. 2016;23:708–13. https://doi.org/10.1245/s10434-016-5536-1.
Reibetanz J, Jurowich C, Erdogan I, et al. Impact of lymphadenectomy on the oncologic outcome of patients with adrenocortical carcinoma. Ann Surg. 2012;255:363–9. https://doi.org/10.1097/sla.0b013e3182367ac3.
Miller BS, Doherty GM. Regional lymphadenectomy for adrenocortical carcinoma. Ann Surg. 2013;257:e13–4. https://doi.org/10.1097/sla.0b013e3182891ee5.
Bittner JG, Gershuni VM, Matthews BD, Moley JF, Brunt LM. Risk factors affecting operative approach, conversion, and morbidity for adrenalectomy: a single-institution series of 402 patients. Surg Endosc. 2013;27:2342–50. https://doi.org/10.1007/s00464-013-2789-7.
Icard P, Louvel A, Chapuis Y. Survival rates and prognostic factors in adrenocortical carcinoma. World J Surg. 2018;16:753–8.
Dindo D, Demartines N, Clavien P-A. Classification of surgical complications. Ann Surg. 2004;240:205–13. https://doi.org/10.1097/01.sla.0000133083.54934.ae.
Grubbs EG, Callender GG, Xing Y, et al. Recurrence of adrenal cortical carcinoma following resection: surgery alone can achieve results equal to surgery plus mitotane. Ann Surg Oncol. 2009;17:263–70. https://doi.org/10.1245/s10434-009-0716-x.
Amini N, Margonis GA, Kim Y, et al. Curative resection of adrenocortical carcinoma: rates and patterns of postoperative recurrence. Ann Surg Oncol. 2015;23:126–33. https://doi.org/10.1245/s10434-015-4810-y.
Chapgar R, Siperstain AE, Berber E. Adrenocortical cancer update. Surg Clin North Am. 2014;94:669–87. https://doi.org/10.1016/j.suc.2014.02.009.
Bellantone R, Ferrante A, Boscherini M, et al. Role of reoperation in recurrence of adrenal cortical carcinoma: tesults from 188 cases collected in the Italian National Registry for Adrenal Cortical Carcinoma. Surgery. 1997;122:1212–8.
Laan DV, Thiels CA, Glasgow A, et al. Adrenocortical carcinoma with inferior vena cava tumor thrombus. Surgery. 2017;161:240–8. https://doi.org/10.1016/j.surg.2016.07.040.
Zhang HM, Perrier ND, Grubbs EG, et al. CT features and quantification of the characteristics of adrenocortical carcinomas on unenhanced and contrast-enhanced studies. Clin Radiol. 2012;67:38–46. https://doi.org/10.1016/j.crad.2011.03.023.
Chiche L, Dousset B, Kieffer E, Chapuis Y. Adrenocortical carcinoma extending into the inferior vena cava: presentation of a 15-patient series and review of the literature. Surgery. 2006;139:15–27. https://doi.org/10.1016/j.surg.2005.05.014.
Hedican SP, Marshall FF. Adrenocortical carcinoma with intracaval extension. J Urol. 1997;158:2056–61.
Keskin S, Tas F, Vatansever S. Adrenocortical carcinoma: clinicopathological features, prognostic factors and outcome. Urol Int. 2013;90:435–8. https://doi.org/10.1159/000345489.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Marincola Smith, P., Kiernan, C.M., Tran, T.B. et al. Role of Additional Organ Resection in Adrenocortical Carcinoma: Analysis of 167 Patients from the U.S. Adrenocortical Carcinoma Database. Ann Surg Oncol 25, 2308–2315 (2018). https://doi.org/10.1245/s10434-018-6546-y
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-018-6546-y