
Abstract
Background
In rectal cancer surgery, proximal ligation of the inferior mesenteric artery (IMA) with radical lymphadenectomy is the accepted standard of care.1 Our purpose is to describe three different standardized technical approaches for the management of the IMA during D3 lymphadenectomy.2
Methods
Operative videos of three robotic D3 lymphadenectomy procedures for rectal cancer were reviewed and annotated with schematic anatomical descriptions for clarification.
Results
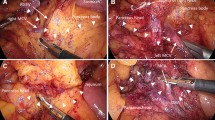
There are three methods for the management of the IMA during D3 lymphadenectomy for rectal cancer. Standard high ligation is technically the simplest to perform and provides excellent mesenteric length but relies solely on marginal vessel blood supply from the middle colic artery.3 Low ligation with ascending left colic artery preservation is more complex technically but affords excellent vascular supply due to preservation of IMA blood flow, while potentially limiting mesenteric length.4 The central vascular sparing technique is the most complex to perform but allows excellent mesenteric length due to the presence of two separate points of mesenteric division, while also potentially improving blood supply due to decreased vascular resistance and improved collateralization. With each technique, central ligation of the inferior mesenteric vein above the splenic flexure tributary is performed to release the mesentery.
Conclusions
The three methods to manage the IMA vary in their technical complexity, preservation of colonic conduit blood supply, and provision of mesenteric length, with associated advantages and disadvantages. The choice of technique is dependent on anatomical and oncological considerations.
Article PDF
Similar content being viewed by others


Avoid common mistakes on your manuscript.
References
Sammour T, Malakorn S, Bednarski BK, et al. Oncological outcomes after robotic proctectomy for rectal cancer: analysis of a prospective database. Ann Surg. 2016 (Epub ahead of print).
Watanabe T, Itabashi M, Shimada Y, et al. Japanese Society for Cancer of the Colon and Rectum (JSCCR) Guidelines 2014 for treatment of colorectal cancer. Int J Clin Oncol. 2015;20(2):207–39.
Komen N, Slieker J, de Kort P, et al. High tie versus low tie in rectal surgery: comparison of anastomotic perfusion. Int J Colorectal Dis. 2011;26(8):1075–8.
Bonnet S, Berger A, Hentati N, et al. High tie versus low tie vascular ligation of the inferior mesenteric artery in colorectal cancer surgery: impact on the gain in colon length and implications on the feasibility of anastomoses. Dis Colon Rectum. 2012;55:515–21.
Authors contribution
All authors made substantial contributions to: conception, design, acquisition of data, analysis and interpretation of data; drafting the article and revising it critically for important intellectual content; and gave final approval of the version to be published.
Conflict of interest
The authors have no conflict of interest to declare.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
In rectal cancer surgery, there is variation in how the vascular dissection is performed. We report operative videos to demonstrate three standardized approaches to robotic D3 lymphadenectomy for rectal cancer. We annotated the videos with schematic anatomical descriptions for clarification (M4 V 196399 kb)
Rights and permissions
About this article

Cite this article
Malakorn, S., Sammour, T., Bednarski, B. et al. Three Different Approaches to the Inferior Mesenteric Artery during Robotic D3 Lymphadenectomy for Rectal Cancer. Ann Surg Oncol 24, 1923 (2017). https://doi.org/10.1245/s10434-017-5792-8
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-017-5792-8