
Abstract
Background
Pelvic radiotherapy (RT) is a standard component of the management for patients with locally advanced rectal cancer or squamous cell carcinoma of the anus. Pelvic RT leads to permanent and irreversible ovarian failure in young women. This study aimed to determine the effectiveness of robotically assisted laparoscopic ovarian transposition (OT) before RT in women with rectal or anal cancer who wanted to preserve normal ovarian function.
Methods
The study reviewed the medical records of all patients treated at our institution from August 2009 to October 2014 who received robotically assisted laparoscopic OT for rectal or anal cancer before RT. Clinical and hormonal data were abstracted to determine ovarian function.
Results
The study identified 22 women with rectal (n = 20) or anal (n = 2) cancer. The median age of the women was 39 years (range 26–45 years). For one patient, OT was technically not feasible. The postoperative course was uneventful in all but one case. Follow-up data on ovarian function were unavailable for 3 patients. The median times from RT initiation to the last gynecologic or hormonal evaluation were 9 months (range 5–47 months) and 10.5 months (range 5–47 months), respectively. At the last gynecologic or hormonal follow-up visit, ovarian function was preserved in 12 (67%) of 18 evaluable patients, including 9 (90%) of 10 patients 40 years of age or younger and 3 (38%) of 8 patients older than 40 years (P = 0.07).
Conclusions
Robotically assisted laparoscopic bilateral OT is safe and can lead to preservation of ovarian function in two-thirds of patients with low gastrointestinal cancer undergoing pelvic RT. It should be considered in this setting, especially for women age 40 years or younger, to avoid premature menopause and its associated sequelae.
Similar content being viewed by others


Colorectal cancer (CRC) is the third most common cancer among women, accounting for approximately 8% of all cancer deaths.1 It is estimated that CRC will be diagnosed in 63,670 women in the United States in 2016, of whom 16,110 will have localized rectal cancers.1 The incidence of rectal cancer among younger adults (ages 20–40 years) has been increasing in recent decades. A predictive model shows that by the year 2030, 23% of rectal cancers will be diagnosed in patients younger than 50 years.2–4
The standard management of locally advanced rectal cancer (stages 2 and 3 disease) involves preoperative pelvic radiotherapy (RT) and concurrent 5-fluorouracil (5-FU) or capecitabine.5
Squamous cell carcinoma (SCC) of the anal canal is a rare malignancy.
As projected, CRC will be diagnosed in slightly more than 7500 new cases in the United States in 2016.1 However, the incidence has risen 2–3% per year during the last two decades due to the widespread prevalence of human papilloma virus (HPV) infection. It occurs more commonly among women.6,7 Fortunately, early-stage disease accounts for a majority of the cases. With definitive chemotherapy and pelvic RT, the treatment of localized anal cancer yields excellent outcomes.5
Given the long survivorship of young patients with rectal and anal cancer, the risk of treatment-associated premature menopause and its consequences, ranging from genitourinary symptoms or hot flushes to increased risk of osteoporosis and cardiovascular events, is a serious consideration.7–11 A recent study of 51 patients showed that 94.1% of these patients experienced persistent amenorrhea after pelvic chemoradiotherapy.12
To minimize radiation-related ovarian damage, ovarian transposition (OT) (oophoropexy), a technique that aims to move the ovaries outside the irradiation field, was developed more than three decades ago. After laparoscopic surgery, preservation of ovarian function can be achieved in 89% of women younger than 40 years who undergo pelvic RT for a variety of malignancies of gynecologic and non-gynecologic origin.13 On this basis, the American Society of Clinical Oncology (ASCO) guidelines state that OT should be discussed as an option for premenopausal women when pelvic RT is planned.14
To date, preservation of ovarian function for patients with anal and rectal cancers undergoing OT has been assessed in case studies or small series. We aimed to determine the efficacy of robotically assisted laparoscopic OT before pelvic RT for patients with anal and rectal cancer interested in preserving reproductive potential and avoiding the deleterious effects of premature menopause.
Methods
In 2009, after institutional review and approval, we instituted an initiative at Memorial Sloan Kettering Cancer Center (MSK) to refer young women with lower gastrointestinal (GI) cancers to be evaluated for robotically assisted laparoscopic OT before pelvic RT. A prospective database of patients undergoing this procedure was maintained. After 5 years, we retrospectively reviewed the medical charts of women with anal and rectal cancers who underwent robotically assisted laparoscopic OT between August 2009 and October 2014. Patient characteristics, treatment plans, and follow-up data were obtained. Pre- and postoperative follicle-stimulating hormone (FSH) and estradiol (E2) serum levels were available for a subset of patients. In the context of absent or infrequent menses, we considered a FSH level higher than 20 mIU/mL and an E2 level lower than 30 pg/mL to be indicative of premature ovarian failure.11 When hormonal levels were lacking, absent or infrequent, menses with concomitant menopausal symptoms were used to define premature ovarian insufficiency. All patients had normal menstrual function before initiation of therapy, OT, or both.
To decrease the risk of paratubal cyst formation and hydrosalpinx, and in light of the potential role of opportunistic salpingectomy in preventing ovarian cancer, our preferred technique was to remove the fallopian tube in addition to performing utero-ovarian ligament transection.15 This allowed for placement of the ovaries well outside the radiation fields.
The infundibulopelvic ligaments were dissected, and the ovaries were secured to the peritoneum in the right and left paracolic gutters with Vicryl suture. We aimed to place the ovaries above the level of L5–S1, corresponding to the superior aspect of the pelvic RT field, by using anatomic landmarks. The ovaries were placed lateral to the ascending and descending colon in the paracolic recesses. The ascending and descending colons were not mobilized from the retroperitoneum. Surgical clips were placed circumferentially to facilitate better visualization during RT simulation planning.
We counseled patients that they would not be able to conceive spontaneously and that the ovaries would not be repositioned in the pelvis. We encouraged them to seek assessment by a fertility specialist to discuss additional fertility preservation options either before or after cancer treatment. We also advised patients that if conversion to laparotomy was needed to complete the procedure, laparoscopic OT would be aborted to avoid excessive delay in their primary cancer therapy.
Descriptive statistics were generated, and the χ 2 test or Fisher’s exact test were used as appropriate. For statistical analysis, SPSS 21.0 (SPSS, Chicago, IL, USA) was used.
Results
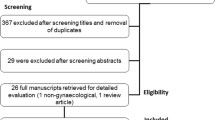
The study identified 22 patients (20 with rectal cancer and two with anal cancer). Ovarian transposition was aborted due to adhesions in one patient with rectal cancer who would have required laparotomy. Descriptive characteristics of the study population are presented in Table 1. Only one patient experienced a postoperative complication (aspiration pneumonia), but this did not lead to significant delay in initiation of RT (19 days). Of the 21 patients undergoing OT, 10 desired future fertility. Egg or embryo freezing before the start of cancer treatment or OT was pursued by 2 patients.
All 19 patients with rectal cancer who underwent OT had locally advanced or metastatic disease (one with stage 2, 15 with stage 3, and 3 with stage 4 disease). Before starting cancer treatment or OT, none of these patients presented with obstructing symptoms requiring diverting colostomy. Induction chemotherapy was administered to 15 patients, with 13 patients receiving it before OT.
The median time from the last chemotherapy dose to OT was 10 days (range 2–28 days). The median time from OT to initiation of pelvic RT was 20 days (range 13–163 days). All the patients underwent CT simulation and radiation oncology treatment planning. Two of the patients received induction chemotherapy after oophoropexy, so the interval between the procedure and initiation of RT was extended to 163 and 131 days, respectively. Excluding these 2 patients, the median time from OT to initiation of radiation was 20 days (range 13–44 days). The radiation dose administered to the patients with rectal cancer ranged from 5000 to 5400 cGy for the rectal tumor to 4500 cGy for the pelvic nodes.
After completion of neoadjuvant treatment, 16 patients underwent either low anterior resection (n = 14) or abdominoperineal resection (n = 2). Adjuvant chemotherapy was offered to 7 patients. The full details of the chemotherapy regimens are presented in Table 2.
The median follow-up time from initiation of RT to the last visit or death was 29 months (range 1–72 months). At the last follow-up visit, 14 patients showed no evidence of recurrent disease, 4 patients were alive with disease, and 1 patient had died of disease. The median times from initiation of RT to the last gynecologic examination or hormonal evaluation were 9 months (range 5–47 months) and 10.5 months (range 5–47 months), respectively.
After neoadjuvant treatment, 4 patients did not undergo gynecologic examination, and 7 patients did not have serum FSH and E2 measured. Menopausal status could not be determined for 3 patients.
Both patients with anal SCC had stage 3 disease and were treated exclusively with a total dose of 5600 cGy to the primary tumor and 4500 cGy to the pelvic nodes, with concurrent 5-FU and mitomycin C. One of these patients underwent pelvic RT 13 days after oophoropexy and was alive without evidence of disease 58.7 months later. She was last seen by a gynecologist 35.3 months after the initiation of RT and received a diagnosis of premature menopause. The second patient started radiation 14 days after OT and was deemed premenopausal at her last gynecologic follow-up visit 5 months later. Unfortunately, she died of disease 12 months after beginning treatment.
Overall, 18 of the 21 patients with anal or rectal cancer were evaluable for ovarian function, as previously defined. At the last gynecologic and/or hormonal follow-up visit, ovarian function was preserved in 12 (67%) of the patients. The 18 assessable patients included 10 patients 40 years of age or younger and 8 patients older than 40 years. Ovarian function was retained in 9 (90%) of the 10 patients age 40 years or younger and 3 (38%) of the 8 patients older than 40 years (P = 0.07).
Discussion
It is well established that ionizing radiation can cause direct DNA damage to ovarian follicles, resulting in follicular atrophy and decreased ovarian follicular reserve. The susceptibility of the oocyte to radiation depends on its growth phase. Primordial follicles are considered to be more radioresistant.16 The degree to which radiation impairs ovarian function is further determined by multiple factors, including radiation dose, age at time of exposure, extent of the irradiation field, and fractionation schedule.16,17 At a radiation dose of less than 2 Gy, half of human follicles are depleted.18 The ovaries of women younger than 40 years are less sensitive to the catastrophic consequences of radiation.19,20 A greater distance of the radiation field from the ovaries and the use of fractionated doses exert a relatively protective effect on ovarian function.17,19,21
The effects of chemotherapy on ovarian function are related to age, dose, and type of drug agent. Alkylating agents exhibit the most potent gonadotoxic properties.19,21 Evidence is sparse regarding the impact on ovarian function of the chemotherapy regimens commonly used for rectal cancer. In some studies, 5-FU is reported to affect the ovaries minimally, although one case of premature ovarian failure after therapy with 5-FU has been published.22,23 Oxaliplatin confers a higher risk for ovarian failure and birth defects (although relatively reassuring data have been recently presented).24,25 A study from MSK showed that administration of 5-FU, leucovorin, and oxaliplatin (FOLFOX) was followed by persistent amenorrhea 1 year after completion of chemotherapy in 13% of CRC patients age 40 years or younger.26 In a similar age group, the incidence of long-term amenorrhea after treatment with FOLFOX, capecitabine and oxaliplatin (CAPOX), or capecitabine for colon cancer was reported to be 4.2%.12
Our findings are consistent with the aforementioned data. We found that ovarian preservation was age dependent. We were able to preserve ovarian function in 90% of patients age 40 years or younger. In contrast, ovarian function was preserved in only 38% of women older than 40. The statistical nonsignificance is most certainly due to the small number of cases. Tolerance of the ovaries to chemotherapy, surgical manipulation, and scatter radiation appears to be much less in women older than 40 years. These data can be logically and reasonably used to argue against transposition for women older than 40 years. However, some clinicians note that a 38% rate of preservation is an improvement over 0%.
Reduction of radiation dose to the ovaries is thought to be the mechanism through which OT can prevent ovarian failure before pelvic RT. It is suggested that the transposed ovaries are exposed to 5–10% of the radiation dose they would otherwise have received in their natural anatomic location.21 The success rate of this strategy depends on the dose of radiation to the ovaries and the patient’s age.22
The existing experience with OT for patients with rectal cancer is limited but encouraging.13,27–32 To our knowledge, only one case report describes outcomes after OT for one patient with anal SCC. According to this case report, normal serum FSH levels and menstrual cycles were restored 8 months after completion of pelvic RT.33
As evidenced by the variable rates of ovarian function preservation, OT has limitations. Findings show that OT cannot overcome the possible gonadotoxic effects of chemotherapy.21 Of equal importance, precise calculation and prevention of radiation scatter are difficult.16,21 The potentially beneficial roles of novel radiation techniques such as intensity-modulated RT (IMRT) and proton RT, which can deliver RT more focally, deserve further investigation.16 Cancer survivors who regain cyclic menses after exposure to RT, chemotherapy, or both are still at higher risk for premature menopause in the long term. Long-term follow-up data on the degree to which OT may prevent premature menopause are largely lacking.19 Finally, OT should be performed only when the risk of ovarian microscopic metastasis is very low.32
Complications after OT have been recorded, although these seem infrequent. The complications include ovarian torsion, ureteral injury, bleeding, development of functional cysts, chronic abdominal pain, and adhesions,21,22,30,34 as well as a greater likelihood of premature menopause. This may be due to possible injuries to the ovarian vessels during the procedure or to other less well-defined mechanisms.32 Disease recurrence at the laparoscopic port site or in the transposed ovaries also has been described.21,22,30,35 The risk for migration of the ovaries should always be considered. In case of two-dimensional opposed-field RT, the standard recommended ovarian position during RT is 4 cm outside the radiation field or 1.5 cm above the iliac crest.36,37 If IMRT is implemented, the planning organ-at-risk volume (PRV) margin is 2 cm in all directions.38 Given the risk for ovarian migration, OT should be performed as close to the time of RT as possible.22
Our study represents the largest series of patients undergoing OT before RT, with or without chemotherapy, for lower gastrointestinal cancers. However, we acknowledge several limitations of this study. These include the retrospective nature of this study, lack of homogeneity with respect to timing and type of chemotherapy regimens, and limited follow-up evaluation. Furthermore, we do not report data on fertility outcomes because at this writing, none of our patients has attempted pregnancy.
Although rare, spontaneous pregnancies in rectal cancer patients after OT can be achieved if tubal function is preserved. Otherwise, in vitro fertilization (IVF) is required.22 However, it is widely known that pelvic RT confers a higher risk for pregnancy-adverse events, including spontaneous miscarriages, preterm labor, low-birth-weight infants, and placental abnormalities through multiple mechanisms.16 Therefore, many patients with rectal or anal cancer who receive RT may eventually need IVF and gestational surrogacy to reproduce despite preservation of ovarian function.21,22 Moreover, the decision to bear children after completion of cancer treatment may be influenced by the disease course or treatment side effects. Nonetheless, the impact of premature menopause should not be minimized when couples are counseled, whether they are interested in having future biologic children or not.
In conclusion, despite its limitations, OT seems to be a safe and effective strategy for preserving ovarian function in patients with rectal or anal cancer who undergo pelvic RT. Recovery from this procedure does not result in clinically meaningful delays in cancer treatment. Continued investigation of ovarian function preservation, whether for reproductive or hormonal reasons, is needed. Prospective trials to evaluate the long-term benefits of minimally invasive OT, including comparison of OT with hormonal replacement therapy alone after pelvic RT, would further establish the benefits of this minimally invasive procedure for younger women (age ≤40 years) with rectal or anal cancer. Until then, based on our single-institution series, robotically assisted laparoscopic OT should be strongly considered for these patients in order to avoid premature menopause and its associated sequelae.
References
Siegel RL, Miller KD, Jemal A. Cancer statistics, 2016. CA Cancer J Clin. 2016;66:7–30.
Inra JA, Syngal S. Colorectal cancer in young adults. Dig Dis Sci. 2015;60:722–33.
Meyer JE, Narang T, Schnoll-Sussman FH, Pochapin MB, Christos PJ, Sherr DL. Increasing incidence of rectal cancer in patients aged younger than 40 years: an analysis of the surveillance, epidemiology, and end results database. Cancer. 2010;116:4354–9.
Bailey CE, Hu CY, You YN, et al. Increasing disparities in the age-related incidences of colon and rectal cancers in the United States, 1975–2010. JAMA Surg. 2015;150:17–22.
National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology. 2016. https://www.nccn.org/professionals/physician_gls/f_guidelines.asp. Accessed 16 Jun 2016.
Joseph DA, Miller JW, Wu X, et al. Understanding the burden of human papillomavirus-associated anal cancers in the U. S. Cancer. 2008;113(10 Suppl):2892–900.
Nelson RA, Levine AM, Bernstein L, Smith DD, Lai LL. Changing patterns of anal canal carcinoma in the United States. J Clin Oncol. 2013;31:1569–75.
O’Connell JB, Maggard MA, Liu JH, Etzioni DA, Livingston EH, Ko CY. Do young colon cancer patients have worse outcomes? World J Surg. 2004;28:558–62.
Quah HM, Joseph R, Schrag D, et al. Young age influences treatment but not outcome of colon cancer. Ann Surg Oncol. 2007;14:2759–65.
Gunderson LL, Winter KA, Ajani JA, et al. Long-term update of US GI intergroup RTOG 98-11 phase III trial for anal carcinoma: survival, relapse, and colostomy failure with concurrent chemoradiation involving fluorouracil/mitomycin versus fluorouracil/cisplatin. J Clin Oncol. 2012;30:4344–51.
Torrealday S, Pal L. Premature menopause. Endocrinol Metab Clin N Am. 2015;44:543–57.
Wan J, Gai Y, Li G, Tao Z, Zhang Z. Incidence of chemotherapy- and chemoradiotherapy-induced amenorrhea in premenopausal women with stage II/III colorectal cancer. Clin Colorectal Cancer. 2015; 14:31–4.
Bisharah M, Tulandi T. Laparoscopic preservation of ovarian function: an underused procedure. Am J Obstet Gynecol. 2003;188:367–70.
Loren AW, Mangu PB, Beck LN, et al. Fertility preservation for patients with cancer: American Society of Clinical Oncology clinical practice guideline update. J Clin Oncol. 2013;31:2500–10.
Society of Gynecologic Oncology. SGO clinical practice statement: salpingectomy for ovarian cancer prevention, 2013. https://www.sgo.org/clinical-practice/guidelines/sgo-clinical-practice-statement-salpingectomy-for-ovarian-cancer-prevention. Accessed 16 Jun 2016.
Wo JY, Viswanathan AN. Impact of radiotherapy on fertility, pregnancy, and neonatal outcomes in female cancer patients. Int J Radiat Oncol Biol Phys. 2009;73:1304–12.
Vassilakopoulou M, Boostandoost E, Papaxoinis G, de La Rouge TM, Khayat D, Psyrri A. Anticancer treatment and fertility: effect of therapeutic modalities on reproductive system and functions. Crit Rev Oncol Hematol. 2016;97:328–34.
Wallace WH, Thomson AB, Kelsey TW. The radiosensitivity of the human oocyte. Hum Reprod. 2003;18:117–21.
Meirow D, Nugent D. The effects of radiotherapy and chemotherapy on female reproduction. Hum Reprod Update. 2001;7:535–43.
Wallace WH, Thomson AB, Saran F, Kelsey TW. Predicting age of ovarian failure after radiation to a field that includes the ovaries. Int J Radiat Oncol Biol Phys. 2005;62:738–44.
Spanos CP, Mamopoulos A, Tsapas A, Syrakos T, Kiskinis D. Female fertility and colorectal cancer. Int J Colorectal Dis. 2008;23:735–43.
O’Neill MT, Ni Dhonnchu T, Brannigan AE. Topic update: effects of colorectal cancer treatments on female fertility and potential methods for fertility preservation. Dis Colon Rectum. 2011;54:363–9.
Azem F, Amit A, Merimsky O, Lessing JB. Successful transfer of frozen-thawed embryos obtained after subtotal colectomy for colorectal cancer and before fluorouracil-based chemotherapy. Gynecol Oncol. 2004;93:263–5.
Marhhom E, Cohen I. Fertility preservation options for women with malignancies. Obstet Gynecol Surv. 2007;62:58–72.
Levi M, Shalgi R, Brenner B, et al. The impact of oxaliplatin on the gonads: from bedside to the bench. Mol Hum Reprod. 2015;21:885–93.
Cercek A, Siegel CL, Capanu M, Reidy-Lagunes D, Saltz LB. Incidence of chemotherapy-induced amenorrhea in premenopausal women treated with adjuvant FOLFOX for colorectal cancer. Clin Colorectal Cancer. 2013;12:163–7.
Tulandi T, Al-Took S. Laparoscopic ovarian suspension before irradiation. Fertil Steril. 1998;70:381–3.
Elizur SE, Tulandi T, Meterissian S, Huang JY, Levin D, Tan SL. Fertility preservation for young women with rectal cancer: a combined approach from one referral center. J Gastrointest Surg. 2009;13:1111–5.
Kurt M, Uncu G, Cetintas SK, Kucuk N, Guler S, Ozkan L. Successful spontaneous pregnancy in a patient with rectal carcinoma treated with pelvic radiotherapy and concurrent chemotherapy: the unique role of laparoscopic lateral ovary transposition. Eur J Gynaecol Oncol. 2007;28:408–10.
Al-Badawi IA, Al-Aker M, AlSubhi J, et al. Laparoscopic ovarian transposition before pelvic irradiation: a Saudi tertiary center experience. Int J Gynecol Cancer. 2010;20:1082–6.
Al-Asari S, Abduljabbar A. Laparoscopic ovarian transposition before pelvic radiation in rectal cancer patient: safety and feasibility. Ann Surg Innov Res. 2012;6:9.
Barahmeh S, Al Masri M, Badran O, et al. Ovarian transposition before pelvic irradiation: indications and functional outcome. J Obstet Gynaecol Res. 2013;39:1533–7.
Treissman MJ, Miller D, McComb PF. Laparoscopic lateral ovarian transposition. Fertil Steril. 1996;65:1229–31.
Gomez-Hidalgo NR, Darin MD, Dalton H, et al. Ovarian torsion after laparoscopic ovarian transposition in patients with gynecologic cancer: a report of two cases. J Minim Invasive Gynecol. 2015;22:687–90.
Picone O, Aucouturier JS, Louboutin A, Coscas Y, Camus E. Abdominal wall metastasis of a cervical adenocarcinoma at the laparoscopic trocar insertion site after ovarian transposition: case report and review of the literature. Gynecol Oncol. 2003;90:446–9.
van Beurden M, Schuster-Uitterhoeve AL, Lammes FB. Feasibility of transposition of the ovaries in the surgical and radiotherapeutical treatment of cervical cancer. Eur J Surg Oncol. 1990;16:141–6.
Hwang JH, Yoo HJ, Park SH, et al. Association between the location of transposed ovary and ovarian function in patients with uterine cervical cancer treated with (postoperative or primary) pelvic radiotherapy. Fertil Steril. 2012;97:1387–93. e1–2.
Soda I, Ishiyama H, Ono S, et al. Assessment of transposed ovarian movement: how much of a safety margin should be added during pelvic radiotherapy? J Radiat Res. 2015;56:354–9.
Acknowledgement
This study was funded in part through the NIH/NCI Support Grant P30 CA008748.
Disclosure
There are no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Sioulas, V.D., Jorge, S., Chern, JY. et al. Robotically Assisted Laparoscopic Ovarian Transposition in Women with Lower Gastrointestinal Cancer Undergoing Pelvic Radiotherapy. Ann Surg Oncol 24, 251–256 (2017). https://doi.org/10.1245/s10434-016-5650-0
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-016-5650-0