
Abstract
Objective
This study aimed to evaluate and compare learning curves for the retroauricular (RA) and transaxillary (TA) approaches in endoscopic hemithyroidectomy.
Methods
The medical records of 290 patients who underwent hemithyroidectomy by either the RA or TA approach from November 2007 through December 2015 were retrospectively reviewed (113 patients with RA and 177 with TA). The two groups were compared with regard to patient characteristics, perioperative clinical results, and complications. Learning curves for the two approaches were compared based on the number of cases required to reach a consistent operation time and drainage amount.
Results
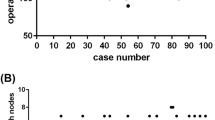
Age at diagnosis, tumor size and location, and thyroid size were not significantly different between the two approach groups. Multiplicity and extrathyroid extension were more prevalent in the RA approach (p = 0.048 and 0.020, respectively). Operation time and hospital day were significantly shorter in the RA approach (p < 0.001 and p = 0.030), while postoperative bleeding was less common in the TA approach (p = 0.021). Operation time and drainage amount stabilized after 50 cases for RA and 90 cases for TA. Additionally, operation time, amount of drainage, hospital stay, and complication rates significantly decreased after stabilization of the learning curve. When comparing the two approaches before stabilization, postoperative bleeding was more frequent in the RA approach (p = 0.044), while no difference was observed after stabilization.
Conclusions
The RA approach seems to be beneficial for reducing operation time and hospital stay, and for stabilization of the learning curve. Postoperative bleeding should be considered during the period of early experience for the RA approach.



Similar content being viewed by others


References
Singer MC, Seybt MW, Terris DJ. Robotic facelift thyroidectomy: I. Preclinical simulation and morphometric assessment. Laryngoscope. 2011;121(8):1631–5.
Terris DJ, Singer MC, Seybt MW. Robotic facelift thyroidectomy: II. Clinical feasibility and safety. Laryngoscope. 2011;121(8):1636–41.
Kang SW, Jeong JJ, Yun JS, et al. Robot-assisted endoscopic surgery for thyroid cancer: experience with the first 100 patients. Surg Endosc. 2009;23(11):2399–406.
Lee DY, Lee KJ, Han WG, et al. Comparison of transaxillary approach, retroauricular approach, and conventional open hemithyroidectomy: a prospective study at single institution. Surgery. 2016;159(2):524–31.
Chung WY. Pros of robotic transaxillary thyroid surgery: its impact on cancer control and surgical quality. Thyroid. 2012;22(10):986–7.
Chung EJ, Park MW, Cho JG, et al. A prospective 1-year comparative study of endoscopic thyroidectomy via a retroauricular approach versus conventional open thyroidectomy at a single institution. Ann Surg Oncol. 2015;22(9):3014–21.
Lewis CM, Chung WY, Holsinger FC. Feasibility and surgical approach of transaxillary robotic thyroidectomy without CO(2) insufflation. Head Neck. 2010;32(1):121–6.
Hyun K, Byon W, Park HJ, Park Y, Park C, Yun JS. Comparison of swallowing disorder following gasless transaxillary endoscopic thyroidectomy versus conventional open thyroidectomy. Surg Endosc. 2014;28(6):1914–20.
Tae K, Song CM, Ji YB, Kim KR, Kim JY, Choi YY. Comparison of surgical completeness between robotic total thyroidectomy versus open thyroidectomy. Laryngoscope. 2014;124(4):1042–7.
Kang SW, Jeong JJ, Nam KH, Chang HS, Chung WY, Park CS. Robot-assisted endoscopic thyroidectomy for thyroid malignancies using a gasless transaxillary approach. J Am Coll Surg. 2009;209(2):e1–7.
Tae K, Ji YB, Jeong JH, Lee SH, Jeong MA, Park CW. Robotic thyroidectomy by a gasless unilateral axillo-breast or axillary approach: our early experiences. Surg Endosc. 2011;25(1):221–8.
Tae K, Ji YB, Jeong JH, Kim KR, Choi WH, Ahn YH. Comparative study of robotic versus endoscopic thyroidectomy by a gasless unilateral axillo-breast or axillary approach. Head Neck. 2013;35(4):477–84.
Lang BH, Wong CK, Tsang JS, Wong KP. A systematic review and meta-analysis comparing outcomes between robotic-assisted thyroidectomy and non-robotic endoscopic thyroidectomy. J Surg Res. 2014;191(2):389–98.
Kiong KL, Iyer NG, Skanthakumar T, et al. Transaxillary thyroidectomies: a comparative learning experience of robotic vs endoscopic thyroidectomies. Otolaryngol Head Neck Surg. 2015;152(5):820–6.
Lee DY, Lim S, Kang SH, et al. A prospective 1-year comparative study of transaxillary total thyroidectomy regarding functional outcomes: is it really promising? Surg Endosc. 2016;30(4):1599–606.
Dincler S, Koller MT, Steurer J, Bachmann LM, Christen D, Buchmann P. Multidimensional analysis of learning curves in laparoscopic sigmoid resection: eight-year results. Dis Colon Rectum. 2003;46(10):1371–8; discussion 1378-1379.
Liu S, Qiu M, Jiang DZ, et al. The learning curve for endoscopic thyroidectomy: a single surgeon’s experience. Surg Endosc. 2009;23(8):1802–6.
Lee J, Yun JH, Nam KH, Soh EY, Chung WY. The learning curve for robotic thyroidectomy: a multicenter study. Ann Surg Oncol. 2011;18(1):226–32.
Ikeda Y, Takami H, Sasaki Y, Takayama J, Niimi M, Kan S. Comparative study of thyroidectomies. Endoscopic surgery versus conventional open surgery. Surg Endosc. 2002;16(12):1741–5.
Sanli O, Tefik T, Erdem S, et al. Prospective evaluation of complications in laparoscopic urology at a mid-volume institution using standardized criteria: experience of 1023 cases including learning curve in 9 years. J Minim Access Surg. 2016;12(1):33–40.
Dal Moro F, Gardiman MP. Scoring surgical skill in Robotic Prostatectomy as adherence to the surgical plan: proposal for a new tool (ScAPSA). Minerva Urol Nefrol. Epub 9 Sep 2015.
Gill J, Booth MI, Stratford J, Dehn TC. The extended learning curve for laparoscopic fundoplication: a cohort analysis of 400 consecutive cases. J Gastrointest Surg. 2007;11(4):487–92.
Disclosures
Doh Young Lee, Dong Ju Oh, Ka Ram Kang, Min-Su Kim, Kyoung Ho Oh, Seung-Kuk Baek, Soon-Young Kwon, Jeong-Soo Woo, and Kwang-Yoon Jung have no disclosures to declare.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Lee, D.Y., Oh, D.J., Kang, K.R. et al. Comparison of Learning Curves for Retroauricular and Transaxillary Endoscopic Hemithyroidectomy. Ann Surg Oncol 23, 4023–4028 (2016). https://doi.org/10.1245/s10434-016-5433-7
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-016-5433-7