
Abstract
Background
Concern for postoperative complications causing airway compromise has limited widespread acceptance of ambulatory thyroid surgery. We evaluated differences in outcomes and hospital costs in those monitored for a short stay of 6 h (SS), inpatient observation of 6–23 h (IO), or inpatient admission of >23 h (IA).
Methods
We retrospectively reviewed all patients undergoing thyroidectomy from 2006 to 2012. The incidence of postoperative hemorrhage, nerve dysfunction, and hypocalcemia were evaluated, as well as cost data comparing the SS and IO groups.
Results
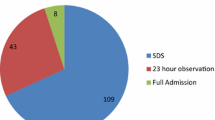
Of 1447 thyroidectomies, 880 (60.8 %) were performed as SS, 401 (27.7 %) as IO, and 166 (11.5 %) as IA. Fewer patients in the SS group (59 %) underwent total thyroidectomy than IO (73 %) and IA (71 %; p < 0.01), and SS patients had smaller thyroid weights (27.9 g) compared with IO and IA (47.2 and 98.9 g, respectively; p < 0.01). Ten (0.69 %) patients developed hematomas requiring reoperation, five of the ten patients received antiplatelet or anticoagulant therapy perioperatively. Only one patient in the IA group bled within the 6- to 23-h period, and no patients with bleeding who were discharged at 6 h would have benefitted from 23-h observation. Twenty-four (1.66 %) recurrent laryngeal nerve injuries were identified, 16 with temporary neuropraxias. In addition, 24 (1.66 %) patients had symptomatic hypocalcemia, which was transient in 17 individuals. Financial data showed higher payments and lower costs associated with SS compared with IO.
Conclusions
Selective SS thyroidectomy can be safe and cost effective, with few overall complications in patients undergoing more complex operations involving larger thyroids who were admitted to hospital.
Similar content being viewed by others


References
Lo Gerfo P, Gates R, Gazetas P Outpatient and short-stay thyroid surgery. Head Neck. 1991;13:97–101.
Leyre P, Desurmont T, Lacoste L et al. Does the risk of compressive hematoma after thyroidectomy authorize 1-day surgery? Langenbecks Arch Surg. 2008;393:733–37.
Snyder SK, Hamid KS, Roberson CR et al. Outpatient thyroidectomy is safe and reasonable: experience with more than 1,000 planned outpatient procedures. J Am Coll Surg. 2010;210:575–582, 582–584.
Burkey SH, van Heerden JA, Thompson GB et al. Reexploration for symptomatic hematomas after cervical exploration. Surgery. 2001;130:914–20.
Weiss A, Lee KC, Brumund KT et al. Risk factors for hematoma after thyroidectomy: results from the nationwide inpatient sample. Surgery. 2014;156:399–404.
Dehal A, Abbas A, Hussain F, Johna S. Risk factors for neck hematoma after thyroid or parathyroid surgery: ten-year analysis of the nationwide inpatient sample database. Perm J. 2015;19:22–8.
Steward DL. The pros and cons of outpatient thyroidectomy. JAMA Otolaryngol Head Neck Surg. 2014;140:1074–76.
Calo PG, Erdas E, Medas F et al. Late bleeding after total thyroidectomy: report of two cases occurring 13 days after operation. Clin Med Insights Case Rep. 2013;6:165–70.
Campbell MJ, McCoy KL, Shen WT et al. A multi-institutional international study of risk factors for hematoma after thyroidectomy. Surgery. 2013;154:1283–89, discussion 1289–1291
Morton RP, Mak V, Moss D, Ahmad Z, Sevao J. Risk of bleeding after thyroid surgery: matched pairs analysis. J Laryngol Otol. 2012;126:285–88.
Hardman JC, Smith JA, Nankivell P, Sharma N, Watkinson JC. Re-operative thyroid surgery: a 20-year prospective cohort study at a tertiary referral centre. Eur Arch Otorhinolaryngol. 2015;272:1503–08.
Promberger R, Ott J, Kober F. Risk factors for postoperative bleeding after thyroid surgery. Br J Surg. 2012;99:373–79.
Dixon JL, Snyder SK, Lairmore TC et al. A novel method for the management of post-thyroidectomy or parathyroidectomy hematoma: a single-institution experience after over 4,000 central neck operations. World J Surg. 2014;38:1262–67.
Bircan HY, Inal A, Ozcelik U et al. LigaSure® versus clamp tie technique for thyroid surgery; decreased operative time versus increased inflammatory effect: a prospective randomized study. Eur Rev Med Pharmacol Sci. 2014;18:1997–2005.
Seybt MW, Terris DJ. Outpatient thyroidectomy: experience in over 200 patients. Laryngoscope. 2010;120:959–63.
Fama F, Linard C, Patti R et al. Short-stay hospitalisation for benign thyroid surgery: a prospective study. Eur Arch Otorhinolaryngol. 2013;270:301–04.
Orosco RK, Lin HW, Bhattacharyya N. Ambulatory thyroidectomy: a multistate study of revisits and complications. Otolaryngol Head Neck Surg. 2015;152(6):1017–23.
Doran HE, Palazzo F. Ambulatory thyroid surgery: do the risks overcome the benefits? Presse Med. 2014;43:291–96.
Trottier DC, Barron P, Moonje V, Tadros S. Outpatient thyroid surgery: should patients be discharged on the day of their procedures? Can J Surg. 2009;52:182–6.
Sun GH, DeMonner S, Davis MM. Epidemiological and economic trends in inpatient and outpatient thyroidectomy in the United States, 1996–2006. Thyroid. 2013;23:727–33.
Vrabec S, Oltmann SC, Clark N, Chen H, Sippel RS. A short-stay unit for thyroidectomy patients increases discharge efficiency. J Surg Res. 2013;184:204–08.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Narayanan, S., Arumugam, D., Mennona, S. et al. An Evaluation of Postoperative Complications and Cost After Short-Stay Thyroid Operations. Ann Surg Oncol 23, 1440–1445 (2016). https://doi.org/10.1245/s10434-015-5004-3
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-015-5004-3