
Abstract
Background
Understanding recurrence patterns is vital for guiding treatment. This study describes recurrence patterns for patients with stage IIIB/C head and neck melanoma (HNM) after therapeutic lymph node dissection (TLND) ± adjuvant radiation therapy (RT). We also report outcomes for salvage therapy for patients with isolated regional relapse.
Methods and Materials
A single-institution prospective database of 173 patients with American Joint Committee on Cancer (AJCC) stage IIIB/C HNM undergoing TLND between 1997 and 2012 was retrospectively reviewed. Timing and patterns of recurrence were reviewed. Univariable and multivariable analyses were undertaken using the Kaplan–Meier and Cox regression methods to determine factors predictive of recurrence. Median follow-up was 32 months.
Results
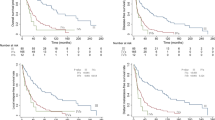
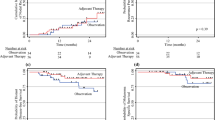
Adjuvant RT was administered to 66/173 (38 %) patients. Patients selected for RT had a higher AJCC stage and had more extracapsular invasion. The 5-year distant, cervical nodal and in-transit recurrence rates were 38, 10, and 13 %, respectively, following surgery alone compared with 60, 17, and 31 %, respectively, for the adjuvant RT group. The head and neck regional 5-year recurrence rate (combining in-basin nodal and in-transit) was 23 % for the entire cohort. Isolated cervical recurrence occurred in 19 patients: 17/19 underwent salvage surgery (10/17 patients received RT after salvage surgery) and 2/19 had RT alone. However, distant recurrence occurred in 12/19 salvage patients, with most occurring within 12 months, while 4/19 were disease free.
Conclusions
Using a selective approach for adjuvant RT, isolated cervical recurrence after TLND is uncommon. Isolated cervical recurrence can be salvaged effectively with further local therapy; however, distant disease frequently follows.


Similar content being viewed by others

References
Martin RC, Shannon KF, Quinn MJ, et al. The management of cervical lymph nodes in patients with cutaneous melanoma. Ann Surg Oncol. 2012;19(12):3926–32.
Burmeister BH, Henderson MA, Ainslie J, et al. Adjuvant radiotherapy versus observation alone for patients at risk of lymph-node field relapse after therapeutic lymphadenectomy for melanoma: a randomised trial. Lancet Oncol. 2012;13(6):589–97.
Siskind V, Whiteman DC, Aitken JF, Martin NG, Green AC. An analysis of risk factors for cutaneous melanoma by anatomical site (Australia). Cancer Causes Control. 2005;16(3):193–9.
Fadaki N, Li R, Parrett B, et al. Is head and neck melanoma different from trunk and extremity melanomas with respect to sentinel lymph node status and clinical outcome? Ann Surg Oncol. 2013;20(9):3089–97.
Balch CM, Gershenwald JE, Soong SJ, et al. Final version of 2009 AJCC melanoma staging and classification. J Clin Oncol. 2009;27(36):6199–206.
O’Brien CJ, Coates AS, Petersen-Schaefer K, et al. Experience with 998 cutaneous melanomas of the head and neck over 30 years. Am J Surg. 1991;162(4):310–4.
Morton DL, Thompson JF, Cochran AJ, et al. Final trial report of sentinel-node biopsy versus nodal observation in melanoma. N Engl J Med. 2014;370(7):599–609.
White RR, Stanley WE, Johnson JL, Tyler DS, Seigler HF. Long-term survival in 2,505 patients with melanoma with regional lymph node metastasis. Ann Surg. 2002;235(6):879–87.
Shen P, Wanek LA, Morton DL. Is adjuvant radiotherapy necessary after positive lymph node dissection in head and neck melanomas? Ann Surg Oncol. 2000;7(8):554–9; discussion 60-1.
Amos CI, Wang LE, Lee JE, et al. Genome-wide association study identifies novel loci predisposing to cutaneous melanoma. Hum Mol Genet. 2011;20(24):5012–23.
O’Brien CJ, Petersen-Schaefer K, Stevens GN, et al. Adjuvant radiotherapy following neck dissection and parotidectomy for metastatic malignant melanoma. Head Neck. 1997;19(7):589–94.
Prens SP, van der Ploeg AP, van Akkooi AC, et al. Outcome after therapeutic lymph node dissection in patients with unknown primary melanoma site. Ann Surg Oncol. 2011;18(13):3586–92.
Young SE, Martinez SR, Faries MB, Essner R, Wanek LA, Morton DL. Can surgical therapy alone achieve long-term cure of melanoma metastatic to regional nodes? Cancer J. 2006;12(3):207–11.
Fisher SR. Elective, therapeutic, and delayed lymph node dissection for malignant melanoma of the head and neck: analysis of 1444 patients from 1970 to 1998. Laryngoscope. 2002;112(1):99–110.
Ballo MT, Strom EA, Zagars GK, et al. Adjuvant irradiation for axillary metastases from malignant melanoma. Int J Radiat Oncol Biol Phys. 2002;52(4):964–72.
Glover AR, Allan CP, Wilkinson MJ, Strauss DC, Thomas JM, Hayes AJ. Outcomes of routine ilioinguinal lymph node dissection for palpable inguinal melanoma nodal metastasis. Br J Surg. 2014;101(7):811–9.
Romano E, Scordo M, Dusza SW, Coit DG, Chapman PB. Site and timing of first relapse in stage III melanoma patients: implications for follow-up guidelines. J Clin Oncol. 2010;28(18): 042–7.
Pinkham MB, Foote MC, Burmeister E, et al. Stage III melanoma in the axilla: patterns of regional recurrence after surgery with and without adjuvant radiation therapy. Int J Radiat Oncol Biol Phys. 2013;86(4):702–8.
Barbour AP, Tang YH, Armour N, et al. BRAF mutation status is an independent prognostic factor for resected stage IIIB and IIIC melanoma: implications for melanoma staging and adjuvant therapy. Eur J Cancer. 2014;50(15):2668–76.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Barbour, S., Mark Smithers, B., Allan, C. et al. Patterns of Recurrence in Patients with Stage IIIB/C Cutaneous Melanoma of the Head and Neck Following Surgery With and Without Adjuvant Radiation Therapy: Is Isolated Regional Recurrence Salvageable?. Ann Surg Oncol 22, 4052–4059 (2015). https://doi.org/10.1245/s10434-014-4356-4
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-014-4356-4